WO2021067761A1 - Compositions and methods comprising anti-nrp2 antibodies - Google Patents
Compositions and methods comprising anti-nrp2 antibodies Download PDFInfo
- Publication number
- WO2021067761A1 WO2021067761A1 PCT/US2020/054017 US2020054017W WO2021067761A1 WO 2021067761 A1 WO2021067761 A1 WO 2021067761A1 US 2020054017 W US2020054017 W US 2020054017W WO 2021067761 A1 WO2021067761 A1 WO 2021067761A1
- Authority
- WO
- WIPO (PCT)
- Prior art keywords
- nrp2
- optionally
- antibody
- antigen
- polypeptide
- Prior art date
Links
- 239000000203 mixture Substances 0.000 title claims abstract description 104
- 238000000034 method Methods 0.000 title claims abstract description 67
- 230000027455 binding Effects 0.000 claims abstract description 270
- 239000000427 antigen Substances 0.000 claims abstract description 250
- 108091007433 antigens Proteins 0.000 claims abstract description 250
- 102000036639 antigens Human genes 0.000 claims abstract description 250
- 102000004213 Neuropilin-2 Human genes 0.000 claims abstract description 235
- 108090000770 Neuropilin-2 Proteins 0.000 claims abstract description 235
- 239000012634 fragment Substances 0.000 claims abstract description 208
- 108090000765 processed proteins & peptides Proteins 0.000 claims abstract description 185
- 229920001184 polypeptide Polymers 0.000 claims abstract description 181
- 102000004196 processed proteins & peptides Human genes 0.000 claims abstract description 181
- 239000003446 ligand Substances 0.000 claims abstract description 111
- 230000001225 therapeutic effect Effects 0.000 claims abstract description 96
- 101001124191 Homo sapiens Neuropilin-2 Proteins 0.000 claims abstract description 86
- 102000015227 human neuropilin-2 Human genes 0.000 claims abstract description 86
- 208000037265 diseases, disorders, signs and symptoms Diseases 0.000 claims abstract description 59
- 201000010099 disease Diseases 0.000 claims abstract description 57
- 230000000694 effects Effects 0.000 claims abstract description 18
- 230000003993 interaction Effects 0.000 claims abstract description 13
- 230000001404 mediated effect Effects 0.000 claims abstract description 6
- 206010028980 Neoplasm Diseases 0.000 claims description 87
- 239000005557 antagonist Substances 0.000 claims description 83
- 201000011510 cancer Diseases 0.000 claims description 80
- 150000003384 small molecules Chemical class 0.000 claims description 72
- 102000002111 Neuropilin Human genes 0.000 claims description 68
- 108050009450 Neuropilin Proteins 0.000 claims description 68
- 210000004027 cell Anatomy 0.000 claims description 65
- 239000000556 agonist Substances 0.000 claims description 58
- 239000003795 chemical substances by application Substances 0.000 claims description 55
- 102000029746 Histidine-tRNA Ligase Human genes 0.000 claims description 51
- 101710177011 Histidine-tRNA ligase, cytoplasmic Proteins 0.000 claims description 51
- 101710096715 Probable histidine-tRNA ligase, cytoplasmic Proteins 0.000 claims description 51
- -1 FILA-DR Proteins 0.000 claims description 50
- 102000005962 receptors Human genes 0.000 claims description 45
- 108020003175 receptors Proteins 0.000 claims description 45
- 230000003054 hormonal effect Effects 0.000 claims description 44
- 102000037982 Immune checkpoint proteins Human genes 0.000 claims description 37
- 108091008036 Immune checkpoint proteins Proteins 0.000 claims description 37
- 230000007781 signaling event Effects 0.000 claims description 32
- 210000001744 T-lymphocyte Anatomy 0.000 claims description 30
- 108010038664 atrial natriuretic factor receptor B Proteins 0.000 claims description 30
- 102100033179 Vascular endothelial growth factor receptor 3 Human genes 0.000 claims description 29
- 238000006471 dimerization reaction Methods 0.000 claims description 29
- 150000001413 amino acids Chemical class 0.000 claims description 26
- 210000004072 lung Anatomy 0.000 claims description 26
- 102000002022 plexin Human genes 0.000 claims description 26
- 108050009312 plexin Proteins 0.000 claims description 26
- 239000002243 precursor Substances 0.000 claims description 26
- AOJJSUZBOXZQNB-TZSSRYMLSA-N Doxorubicin Chemical compound O([C@H]1C[C@@](O)(CC=2C(O)=C3C(=O)C=4C=CC=C(C=4C(=O)C3=C(O)C=21)OC)C(=O)CO)[C@H]1C[C@H](N)[C@H](O)[C@H](C)O1 AOJJSUZBOXZQNB-TZSSRYMLSA-N 0.000 claims description 24
- 108010073929 Vascular Endothelial Growth Factor A Proteins 0.000 claims description 24
- 210000004185 liver Anatomy 0.000 claims description 24
- 108010061593 Member 14 Tumor Necrosis Factor Receptors Proteins 0.000 claims description 23
- 102100028785 Tumor necrosis factor receptor superfamily member 14 Human genes 0.000 claims description 23
- 238000011282 treatment Methods 0.000 claims description 22
- 229940126546 immune checkpoint molecule Drugs 0.000 claims description 21
- 101000851030 Homo sapiens Vascular endothelial growth factor receptor 3 Proteins 0.000 claims description 19
- 230000001965 increasing effect Effects 0.000 claims description 19
- NWIBSHFKIJFRCO-WUDYKRTCSA-N Mytomycin Chemical compound C1N2C(C(C(C)=C(N)C3=O)=O)=C3[C@@H](COC(N)=O)[C@@]2(OC)[C@@H]2[C@H]1N2 NWIBSHFKIJFRCO-WUDYKRTCSA-N 0.000 claims description 18
- 108010038512 Platelet-Derived Growth Factor Proteins 0.000 claims description 18
- 102000010780 Platelet-Derived Growth Factor Human genes 0.000 claims description 18
- 108010073923 Vascular Endothelial Growth Factor C Proteins 0.000 claims description 18
- 102000009520 Vascular Endothelial Growth Factor C Human genes 0.000 claims description 18
- 229940100198 alkylating agent Drugs 0.000 claims description 18
- 239000002168 alkylating agent Substances 0.000 claims description 18
- 239000002246 antineoplastic agent Substances 0.000 claims description 18
- 229960001156 mitoxantrone Drugs 0.000 claims description 18
- KKZJGLLVHKMTCM-UHFFFAOYSA-N mitoxantrone Chemical compound O=C1C2=C(O)C=CC(O)=C2C(=O)C2=C1C(NCCNCCO)=CC=C2NCCNCCO KKZJGLLVHKMTCM-UHFFFAOYSA-N 0.000 claims description 18
- 102100033177 Vascular endothelial growth factor receptor 2 Human genes 0.000 claims description 17
- 210000000988 bone and bone Anatomy 0.000 claims description 17
- 102000018233 Fibroblast Growth Factor Human genes 0.000 claims description 16
- 108050007372 Fibroblast Growth Factor Proteins 0.000 claims description 16
- 229940127089 cytotoxic agent Drugs 0.000 claims description 16
- 239000003814 drug Substances 0.000 claims description 16
- 229940126864 fibroblast growth factor Drugs 0.000 claims description 16
- 230000014509 gene expression Effects 0.000 claims description 16
- AIFRHYZBTHREPW-UHFFFAOYSA-N β-carboline Chemical compound N1=CC=C2C3=CC=CC=C3NC2=C1 AIFRHYZBTHREPW-UHFFFAOYSA-N 0.000 claims description 16
- 229940045513 CTLA4 antagonist Drugs 0.000 claims description 15
- 102000014105 Semaphorin Human genes 0.000 claims description 15
- 108050003978 Semaphorin Proteins 0.000 claims description 15
- 229960000397 bevacizumab Drugs 0.000 claims description 15
- 201000001441 melanoma Diseases 0.000 claims description 15
- 230000004044 response Effects 0.000 claims description 15
- 102100039688 Insulin-like growth factor 1 receptor Human genes 0.000 claims description 14
- 238000002619 cancer immunotherapy Methods 0.000 claims description 14
- 230000002401 inhibitory effect Effects 0.000 claims description 14
- 229940043355 kinase inhibitor Drugs 0.000 claims description 14
- 239000003757 phosphotransferase inhibitor Substances 0.000 claims description 14
- 229940124597 therapeutic agent Drugs 0.000 claims description 14
- 102100039498 Cytotoxic T-lymphocyte protein 4 Human genes 0.000 claims description 13
- 101000889276 Homo sapiens Cytotoxic T-lymphocyte protein 4 Proteins 0.000 claims description 13
- 101000843187 Homo sapiens Histidine-tRNA ligase, cytoplasmic Proteins 0.000 claims description 13
- 108010019530 Vascular Endothelial Growth Factors Proteins 0.000 claims description 13
- IJGRMHOSHXDMSA-UHFFFAOYSA-N Atomic nitrogen Chemical compound N#N IJGRMHOSHXDMSA-UHFFFAOYSA-N 0.000 claims description 12
- 102100029822 B- and T-lymphocyte attenuator Human genes 0.000 claims description 12
- 101710144268 B- and T-lymphocyte attenuator Proteins 0.000 claims description 12
- 108010074708 B7-H1 Antigen Proteins 0.000 claims description 12
- DLGOEMSEDOSKAD-UHFFFAOYSA-N Carmustine Chemical compound ClCCNC(=O)N(N=O)CCCl DLGOEMSEDOSKAD-UHFFFAOYSA-N 0.000 claims description 12
- GHASVSINZRGABV-UHFFFAOYSA-N Fluorouracil Chemical compound FC1=CNC(=O)NC1=O GHASVSINZRGABV-UHFFFAOYSA-N 0.000 claims description 12
- 101001137987 Homo sapiens Lymphocyte activation gene 3 protein Proteins 0.000 claims description 12
- 101000666896 Homo sapiens V-type immunoglobulin domain-containing suppressor of T-cell activation Proteins 0.000 claims description 12
- GQYIWUVLTXOXAJ-UHFFFAOYSA-N Lomustine Chemical compound ClCCN(N=O)C(=O)NC1CCCCC1 GQYIWUVLTXOXAJ-UHFFFAOYSA-N 0.000 claims description 12
- 102100020862 Lymphocyte activation gene 3 protein Human genes 0.000 claims description 12
- 101100519207 Mus musculus Pdcd1 gene Proteins 0.000 claims description 12
- ZRKWMRDKSOPRRS-UHFFFAOYSA-N N-Methyl-N-nitrosourea Chemical compound O=NN(C)C(N)=O ZRKWMRDKSOPRRS-UHFFFAOYSA-N 0.000 claims description 12
- 102100024216 Programmed cell death 1 ligand 1 Human genes 0.000 claims description 12
- 108010029485 Protein Isoforms Proteins 0.000 claims description 12
- 102000001708 Protein Isoforms Human genes 0.000 claims description 12
- 108010009583 Transforming Growth Factors Proteins 0.000 claims description 12
- 102000009618 Transforming Growth Factors Human genes 0.000 claims description 12
- 101710136122 Tryptophan 2,3-dioxygenase Proteins 0.000 claims description 12
- 102000057288 Tryptophan 2,3-dioxygenases Human genes 0.000 claims description 12
- 102100038282 V-type immunoglobulin domain-containing suppressor of T-cell activation Human genes 0.000 claims description 12
- USZYSDMBJDPRIF-SVEJIMAYSA-N aclacinomycin A Chemical compound O([C@H]1[C@@H](O)C[C@@H](O[C@H]1C)O[C@H]1[C@H](C[C@@H](O[C@H]1C)O[C@H]1C[C@]([C@@H](C2=CC=3C(=O)C4=CC=CC(O)=C4C(=O)C=3C(O)=C21)C(=O)OC)(O)CC)N(C)C)[C@H]1CCC(=O)[C@H](C)O1 USZYSDMBJDPRIF-SVEJIMAYSA-N 0.000 claims description 12
- 229960004176 aclarubicin Drugs 0.000 claims description 12
- 230000000340 anti-metabolite Effects 0.000 claims description 12
- 229940044684 anti-microtubule agent Drugs 0.000 claims description 12
- 229940100197 antimetabolite Drugs 0.000 claims description 12
- 239000002256 antimetabolite Substances 0.000 claims description 12
- 230000003115 biocidal effect Effects 0.000 claims description 12
- 229960005395 cetuximab Drugs 0.000 claims description 12
- 231100000433 cytotoxic Toxicity 0.000 claims description 12
- 230000001472 cytotoxic effect Effects 0.000 claims description 12
- WVYXNIXAMZOZFK-UHFFFAOYSA-N diaziquone Chemical compound O=C1C(NC(=O)OCC)=C(N2CC2)C(=O)C(NC(=O)OCC)=C1N1CC1 WVYXNIXAMZOZFK-UHFFFAOYSA-N 0.000 claims description 12
- 239000003534 dna topoisomerase inhibitor Substances 0.000 claims description 12
- 229960004679 doxorubicin Drugs 0.000 claims description 12
- 229960000390 fludarabine Drugs 0.000 claims description 12
- GIUYCYHIANZCFB-FJFJXFQQSA-N fludarabine phosphate Chemical compound C1=NC=2C(N)=NC(F)=NC=2N1[C@@H]1O[C@H](COP(O)(O)=O)[C@@H](O)[C@@H]1O GIUYCYHIANZCFB-FJFJXFQQSA-N 0.000 claims description 12
- 229960002949 fluorouracil Drugs 0.000 claims description 12
- 102000006639 indoleamine 2,3-dioxygenase Human genes 0.000 claims description 12
- 108020004201 indoleamine 2,3-dioxygenase Proteins 0.000 claims description 12
- 229960004961 mechlorethamine Drugs 0.000 claims description 12
- HAWPXGHAZFHHAD-UHFFFAOYSA-N mechlorethamine Chemical compound ClCCN(C)CCCl HAWPXGHAZFHHAD-UHFFFAOYSA-N 0.000 claims description 12
- 208000002154 non-small cell lung carcinoma Diseases 0.000 claims description 12
- 229960001972 panitumumab Drugs 0.000 claims description 12
- 239000000583 progesterone congener Substances 0.000 claims description 12
- 239000000333 selective estrogen receptor modulator Substances 0.000 claims description 12
- 229940095743 selective estrogen receptor modulator Drugs 0.000 claims description 12
- 210000001519 tissue Anatomy 0.000 claims description 12
- 229940044693 topoisomerase inhibitor Drugs 0.000 claims description 12
- 241001529936 Murinae Species 0.000 claims description 11
- 102100040112 Tumor necrosis factor receptor superfamily member 10B Human genes 0.000 claims description 11
- 210000002966 serum Anatomy 0.000 claims description 11
- 102000007563 Galectins Human genes 0.000 claims description 10
- 108010046569 Galectins Proteins 0.000 claims description 10
- 101000696493 Homo sapiens Histidine-tRNA ligase, mitochondrial Proteins 0.000 claims description 10
- 108060003951 Immunoglobulin Proteins 0.000 claims description 10
- 108010053100 Vascular Endothelial Growth Factor Receptor-3 Proteins 0.000 claims description 10
- 238000004166 bioassay Methods 0.000 claims description 10
- 102000018358 immunoglobulin Human genes 0.000 claims description 10
- 102000006495 integrins Human genes 0.000 claims description 10
- 108010044426 integrins Proteins 0.000 claims description 10
- 229960002621 pembrolizumab Drugs 0.000 claims description 10
- 210000004303 peritoneum Anatomy 0.000 claims description 10
- 208000029729 tumor suppressor gene on chromosome 11 Diseases 0.000 claims description 10
- WYWHKKSPHMUBEB-UHFFFAOYSA-N 6-Mercaptoguanine Natural products N1C(N)=NC(=S)C2=C1N=CN2 WYWHKKSPHMUBEB-UHFFFAOYSA-N 0.000 claims description 9
- 102000003745 Hepatocyte Growth Factor Human genes 0.000 claims description 9
- 108090000100 Hepatocyte Growth Factor Proteins 0.000 claims description 9
- 101000851007 Homo sapiens Vascular endothelial growth factor receptor 2 Proteins 0.000 claims description 9
- 230000000903 blocking effect Effects 0.000 claims description 9
- 238000013508 migration Methods 0.000 claims description 9
- 108090000623 proteins and genes Proteins 0.000 claims description 9
- DOUMFZQKYFQNTF-WUTVXBCWSA-N (R)-rosmarinic acid Chemical compound C([C@H](C(=O)O)OC(=O)\C=C\C=1C=C(O)C(O)=CC=1)C1=CC=C(O)C(O)=C1 DOUMFZQKYFQNTF-WUTVXBCWSA-N 0.000 claims description 8
- 108700012439 CA9 Proteins 0.000 claims description 8
- 101150013553 CD40 gene Proteins 0.000 claims description 8
- 102100024423 Carbonic anhydrase 9 Human genes 0.000 claims description 8
- 108010022366 Carcinoembryonic Antigen Proteins 0.000 claims description 8
- 102100025475 Carcinoembryonic antigen-related cell adhesion molecule 5 Human genes 0.000 claims description 8
- 108010019670 Chimeric Antigen Receptors Proteins 0.000 claims description 8
- 102000004127 Cytokines Human genes 0.000 claims description 8
- 108090000695 Cytokines Proteins 0.000 claims description 8
- 102000001301 EGF receptor Human genes 0.000 claims description 8
- 108060006698 EGF receptor Proteins 0.000 claims description 8
- 102100031940 Epithelial cell adhesion molecule Human genes 0.000 claims description 8
- 102000010956 Glypican Human genes 0.000 claims description 8
- 108050001154 Glypican Proteins 0.000 claims description 8
- 108050007237 Glypican-3 Proteins 0.000 claims description 8
- 239000000579 Gonadotropin-Releasing Hormone Substances 0.000 claims description 8
- 108010017213 Granulocyte-Macrophage Colony-Stimulating Factor Proteins 0.000 claims description 8
- 102100039620 Granulocyte-macrophage colony-stimulating factor Human genes 0.000 claims description 8
- 101000920667 Homo sapiens Epithelial cell adhesion molecule Proteins 0.000 claims description 8
- 101000599951 Homo sapiens Insulin-like growth factor I Proteins 0.000 claims description 8
- 101000623901 Homo sapiens Mucin-16 Proteins 0.000 claims description 8
- 101000830689 Homo sapiens Protein tyrosine phosphatase type IVA 3 Proteins 0.000 claims description 8
- 101710184277 Insulin-like growth factor 1 receptor Proteins 0.000 claims description 8
- 102100037852 Insulin-like growth factor I Human genes 0.000 claims description 8
- 102000014150 Interferons Human genes 0.000 claims description 8
- 108010050904 Interferons Proteins 0.000 claims description 8
- 102100023123 Mucin-16 Human genes 0.000 claims description 8
- 229940124060 PD-1 antagonist Drugs 0.000 claims description 8
- 108700030875 Programmed Cell Death 1 Ligand 2 Proteins 0.000 claims description 8
- 102100024213 Programmed cell death 1 ligand 2 Human genes 0.000 claims description 8
- 102100023832 Prolyl endopeptidase FAP Human genes 0.000 claims description 8
- 102000006010 Protein Disulfide-Isomerase Human genes 0.000 claims description 8
- 102100024601 Protein tyrosine phosphatase type IVA 3 Human genes 0.000 claims description 8
- 102100029198 SLAM family member 7 Human genes 0.000 claims description 8
- 101710083287 SLAM family member 7 Proteins 0.000 claims description 8
- 101000857870 Squalus acanthias Gonadoliberin Proteins 0.000 claims description 8
- 108091008874 T cell receptors Proteins 0.000 claims description 8
- 102000016266 T-Cell Antigen Receptors Human genes 0.000 claims description 8
- 102100024834 T-cell immunoreceptor with Ig and ITIM domains Human genes 0.000 claims description 8
- 101710090983 T-cell immunoreceptor with Ig and ITIM domains Proteins 0.000 claims description 8
- 102100036922 Tumor necrosis factor ligand superfamily member 13B Human genes 0.000 claims description 8
- 102100040245 Tumor necrosis factor receptor superfamily member 5 Human genes 0.000 claims description 8
- 102100036856 Tumor necrosis factor receptor superfamily member 9 Human genes 0.000 claims description 8
- 102000009519 Vascular Endothelial Growth Factor D Human genes 0.000 claims description 8
- 108010073919 Vascular Endothelial Growth Factor D Proteins 0.000 claims description 8
- 108010053099 Vascular Endothelial Growth Factor Receptor-2 Proteins 0.000 claims description 8
- 210000004556 brain Anatomy 0.000 claims description 8
- 229940022399 cancer vaccine Drugs 0.000 claims description 8
- 238000009566 cancer vaccine Methods 0.000 claims description 8
- 230000001419 dependent effect Effects 0.000 claims description 8
- 108010072257 fibroblast activation protein alpha Proteins 0.000 claims description 8
- XLXSAKCOAKORKW-AQJXLSMYSA-N gonadorelin Chemical compound C([C@@H](C(=O)NCC(=O)N[C@@H](CC(C)C)C(=O)N[C@@H](CCCNC(N)=N)C(=O)N1[C@@H](CCC1)C(=O)NCC(N)=O)NC(=O)[C@H](CO)NC(=O)[C@H](CC=1C2=CC=CC=C2NC=1)NC(=O)[C@H](CC=1N=CNC=1)NC(=O)[C@H]1NC(=O)CC1)C1=CC=C(O)C=C1 XLXSAKCOAKORKW-AQJXLSMYSA-N 0.000 claims description 8
- 229940035638 gonadotropin-releasing hormone Drugs 0.000 claims description 8
- 238000009169 immunotherapy Methods 0.000 claims description 8
- 229940079322 interferon Drugs 0.000 claims description 8
- 108020004999 messenger RNA Proteins 0.000 claims description 8
- 244000309459 oncolytic virus Species 0.000 claims description 8
- 229960005547 pelareorep Drugs 0.000 claims description 8
- 238000011533 pre-incubation Methods 0.000 claims description 8
- 108020003519 protein disulfide isomerase Proteins 0.000 claims description 8
- 230000004936 stimulating effect Effects 0.000 claims description 8
- 229950008461 talimogene laherparepvec Drugs 0.000 claims description 8
- 210000003171 tumor-infiltrating lymphocyte Anatomy 0.000 claims description 8
- 101000610604 Homo sapiens Tumor necrosis factor receptor superfamily member 10B Proteins 0.000 claims description 7
- 238000001514 detection method Methods 0.000 claims description 7
- 230000012010 growth Effects 0.000 claims description 7
- 230000000492 lymphangiogenic effect Effects 0.000 claims description 7
- 230000005012 migration Effects 0.000 claims description 7
- 238000003786 synthesis reaction Methods 0.000 claims description 7
- RCSZIBSPHRZNRQ-BTZXMIIFSA-N (2S)-2-amino-6-[6-[[(2S)-1-[[(2S)-1-[[(3R,4S,5S)-1-[(2S)-2-[(1R,2R)-3-[[(2S)-3-(1H-indol-3-yl)-1-(oxazinan-2-yl)-1-oxopropan-2-yl]amino]-1-methoxy-2-methyl-3-oxopropyl]pyrrolidin-1-yl]-3-methoxy-5-methyl-1-oxoheptan-4-yl]-methylamino]-3-methyl-1-oxobutan-2-yl]amino]-3-methyl-1-oxobutan-2-yl]-methylamino]hexanoylamino]hexanoic acid Chemical compound OC(=O)[C@@H](N)CCCCNC(=O)CCCCCN(C)[C@@H](C(C)C)C(=O)N[C@@H](C(C)C)C(=O)N(C)[C@@H]([C@@H](C)CC)[C@H](OC)CC(=O)N1CCC[C@H]1[C@H](OC)[C@@H](C)C(=O)N[C@H](C(=O)N1OCCCC1)CC1=CNC2=CC=CC=C12 RCSZIBSPHRZNRQ-BTZXMIIFSA-N 0.000 claims description 6
- BXTJCSYMGFJEID-XMTADJHZSA-N (2s)-2-[[(2r,3r)-3-[(2s)-1-[(3r,4s,5s)-4-[[(2s)-2-[[(2s)-2-[6-[3-[(2r)-2-amino-2-carboxyethyl]sulfanyl-2,5-dioxopyrrolidin-1-yl]hexanoyl-methylamino]-3-methylbutanoyl]amino]-3-methylbutanoyl]-methylamino]-3-methoxy-5-methylheptanoyl]pyrrolidin-2-yl]-3-met Chemical compound C([C@H](NC(=O)[C@H](C)[C@@H](OC)[C@@H]1CCCN1C(=O)C[C@H]([C@H]([C@@H](C)CC)N(C)C(=O)[C@@H](NC(=O)[C@H](C(C)C)N(C)C(=O)CCCCCN1C(C(SC[C@H](N)C(O)=O)CC1=O)=O)C(C)C)OC)C(O)=O)C1=CC=CC=C1 BXTJCSYMGFJEID-XMTADJHZSA-N 0.000 claims description 6
- FPVKHBSQESCIEP-UHFFFAOYSA-N (8S)-3-(2-deoxy-beta-D-erythro-pentofuranosyl)-3,6,7,8-tetrahydroimidazo[4,5-d][1,3]diazepin-8-ol Natural products C1C(O)C(CO)OC1N1C(NC=NCC2O)=C2N=C1 FPVKHBSQESCIEP-UHFFFAOYSA-N 0.000 claims description 6
- BKWJAKQVGHWELA-UHFFFAOYSA-N 1-[6-(2-hydroxypropan-2-yl)-2-pyridinyl]-6-[4-(4-methyl-1-piperazinyl)anilino]-2-prop-2-enyl-3-pyrazolo[3,4-d]pyrimidinone Chemical compound C1CN(C)CCN1C(C=C1)=CC=C1NC1=NC=C2C(=O)N(CC=C)N(C=3N=C(C=CC=3)C(C)(C)O)C2=N1 BKWJAKQVGHWELA-UHFFFAOYSA-N 0.000 claims description 6
- ZADWXFSZEAPBJS-JTQLQIEISA-N 1-methyl-L-tryptophan Chemical compound C1=CC=C2N(C)C=C(C[C@H](N)C(O)=O)C2=C1 ZADWXFSZEAPBJS-JTQLQIEISA-N 0.000 claims description 6
- NDMPLJNOPCLANR-UHFFFAOYSA-N 3,4-dihydroxy-15-(4-hydroxy-18-methoxycarbonyl-5,18-seco-ibogamin-18-yl)-16-methoxy-1-methyl-6,7-didehydro-aspidospermidine-3-carboxylic acid methyl ester Natural products C1C(CC)(O)CC(CC2(C(=O)OC)C=3C(=CC4=C(C56C(C(C(O)C7(CC)C=CCN(C67)CC5)(O)C(=O)OC)N4C)C=3)OC)CN1CCC1=C2NC2=CC=CC=C12 NDMPLJNOPCLANR-UHFFFAOYSA-N 0.000 claims description 6
- AOJJSUZBOXZQNB-VTZDEGQISA-N 4'-epidoxorubicin Chemical compound O([C@H]1C[C@@](O)(CC=2C(O)=C3C(=O)C=4C=CC=C(C=4C(=O)C3=C(O)C=21)OC)C(=O)CO)[C@H]1C[C@H](N)[C@@H](O)[C@H](C)O1 AOJJSUZBOXZQNB-VTZDEGQISA-N 0.000 claims description 6
- JARCFMKMOFFIGZ-UHFFFAOYSA-N 4,6-dioxo-n-phenyl-2-sulfanylidene-1,3-diazinane-5-carboxamide Chemical compound O=C1NC(=S)NC(=O)C1C(=O)NC1=CC=CC=C1 JARCFMKMOFFIGZ-UHFFFAOYSA-N 0.000 claims description 6
- XAUDJQYHKZQPEU-KVQBGUIXSA-N 5-aza-2'-deoxycytidine Chemical compound O=C1N=C(N)N=CN1[C@@H]1O[C@H](CO)[C@@H](O)C1 XAUDJQYHKZQPEU-KVQBGUIXSA-N 0.000 claims description 6
- NMUSYJAQQFHJEW-KVTDHHQDSA-N 5-azacytidine Chemical compound O=C1N=C(N)N=CN1[C@H]1[C@H](O)[C@H](O)[C@@H](CO)O1 NMUSYJAQQFHJEW-KVTDHHQDSA-N 0.000 claims description 6
- STQGQHZAVUOBTE-UHFFFAOYSA-N 7-Cyan-hept-2t-en-4,6-diinsaeure Natural products C1=2C(O)=C3C(=O)C=4C(OC)=CC=CC=4C(=O)C3=C(O)C=2CC(O)(C(C)=O)CC1OC1CC(N)C(O)C(C)O1 STQGQHZAVUOBTE-UHFFFAOYSA-N 0.000 claims description 6
- WLCZTRVUXYALDD-IBGZPJMESA-N 7-[[(2s)-2,6-bis(2-methoxyethoxycarbonylamino)hexanoyl]amino]heptoxy-methylphosphinic acid Chemical compound COCCOC(=O)NCCCC[C@H](NC(=O)OCCOC)C(=O)NCCCCCCCOP(C)(O)=O WLCZTRVUXYALDD-IBGZPJMESA-N 0.000 claims description 6
- 229940122815 Aromatase inhibitor Drugs 0.000 claims description 6
- MLDQJTXFUGDVEO-UHFFFAOYSA-N BAY-43-9006 Chemical compound C1=NC(C(=O)NC)=CC(OC=2C=CC(NC(=O)NC=3C=C(C(Cl)=CC=3)C(F)(F)F)=CC=2)=C1 MLDQJTXFUGDVEO-UHFFFAOYSA-N 0.000 claims description 6
- 206010005003 Bladder cancer Diseases 0.000 claims description 6
- 108010006654 Bleomycin Proteins 0.000 claims description 6
- 208000003174 Brain Neoplasms Diseases 0.000 claims description 6
- 206010006187 Breast cancer Diseases 0.000 claims description 6
- 208000026310 Breast neoplasm Diseases 0.000 claims description 6
- COVZYZSDYWQREU-UHFFFAOYSA-N Busulfan Chemical compound CS(=O)(=O)OCCCCOS(C)(=O)=O COVZYZSDYWQREU-UHFFFAOYSA-N 0.000 claims description 6
- FVLVBPDQNARYJU-XAHDHGMMSA-N C[C@H]1CCC(CC1)NC(=O)N(CCCl)N=O Chemical compound C[C@H]1CCC(CC1)NC(=O)N(CCCl)N=O FVLVBPDQNARYJU-XAHDHGMMSA-N 0.000 claims description 6
- KLWPJMFMVPTNCC-UHFFFAOYSA-N Camptothecin Natural products CCC1(O)C(=O)OCC2=C1C=C3C4Nc5ccccc5C=C4CN3C2=O KLWPJMFMVPTNCC-UHFFFAOYSA-N 0.000 claims description 6
- GAGWJHPBXLXJQN-UORFTKCHSA-N Capecitabine Chemical compound C1=C(F)C(NC(=O)OCCCCC)=NC(=O)N1[C@H]1[C@H](O)[C@H](O)[C@@H](C)O1 GAGWJHPBXLXJQN-UORFTKCHSA-N 0.000 claims description 6
- GAGWJHPBXLXJQN-UHFFFAOYSA-N Capecitabine Natural products C1=C(F)C(NC(=O)OCCCCC)=NC(=O)N1C1C(O)C(O)C(C)O1 GAGWJHPBXLXJQN-UHFFFAOYSA-N 0.000 claims description 6
- 102100025064 Cellular tumor antigen p53 Human genes 0.000 claims description 6
- PTOAARAWEBMLNO-KVQBGUIXSA-N Cladribine Chemical compound C1=NC=2C(N)=NC(Cl)=NC=2N1[C@H]1C[C@H](O)[C@@H](CO)O1 PTOAARAWEBMLNO-KVQBGUIXSA-N 0.000 claims description 6
- 206010009944 Colon cancer Diseases 0.000 claims description 6
- 208000001333 Colorectal Neoplasms Diseases 0.000 claims description 6
- CMSMOCZEIVJLDB-UHFFFAOYSA-N Cyclophosphamide Chemical compound ClCCN(CCCl)P1(=O)NCCCO1 CMSMOCZEIVJLDB-UHFFFAOYSA-N 0.000 claims description 6
- UHDGCWIWMRVCDJ-CCXZUQQUSA-N Cytarabine Chemical compound O=C1N=C(N)C=CN1[C@H]1[C@@H](O)[C@H](O)[C@@H](CO)O1 UHDGCWIWMRVCDJ-CCXZUQQUSA-N 0.000 claims description 6
- 108010092160 Dactinomycin Proteins 0.000 claims description 6
- ZBNZXTGUTAYRHI-UHFFFAOYSA-N Dasatinib Chemical compound C=1C(N2CCN(CCO)CC2)=NC(C)=NC=1NC(S1)=NC=C1C(=O)NC1=C(C)C=CC=C1Cl ZBNZXTGUTAYRHI-UHFFFAOYSA-N 0.000 claims description 6
- SAMRUMKYXPVKPA-VFKOLLTISA-N Enocitabine Chemical compound O=C1N=C(NC(=O)CCCCCCCCCCCCCCCCCCCCC)C=CN1[C@H]1[C@@H](O)[C@H](O)[C@@H](CO)O1 SAMRUMKYXPVKPA-VFKOLLTISA-N 0.000 claims description 6
- HTIJFSOGRVMCQR-UHFFFAOYSA-N Epirubicin Natural products COc1cccc2C(=O)c3c(O)c4CC(O)(CC(OC5CC(N)C(=O)C(C)O5)c4c(O)c3C(=O)c12)C(=O)CO HTIJFSOGRVMCQR-UHFFFAOYSA-N 0.000 claims description 6
- 101000721661 Homo sapiens Cellular tumor antigen p53 Proteins 0.000 claims description 6
- 101001034652 Homo sapiens Insulin-like growth factor 1 receptor Proteins 0.000 claims description 6
- 229940123502 Hormone receptor antagonist Drugs 0.000 claims description 6
- XDXDZDZNSLXDNA-TZNDIEGXSA-N Idarubicin Chemical compound C1[C@H](N)[C@H](O)[C@H](C)O[C@H]1O[C@@H]1C2=C(O)C(C(=O)C3=CC=CC=C3C3=O)=C3C(O)=C2C[C@@](O)(C(C)=O)C1 XDXDZDZNSLXDNA-TZNDIEGXSA-N 0.000 claims description 6
- XDXDZDZNSLXDNA-UHFFFAOYSA-N Idarubicin Natural products C1C(N)C(O)C(C)OC1OC1C2=C(O)C(C(=O)C3=CC=CC=C3C3=O)=C3C(O)=C2CC(O)(C(C)=O)C1 XDXDZDZNSLXDNA-UHFFFAOYSA-N 0.000 claims description 6
- 108090000723 Insulin-Like Growth Factor I Proteins 0.000 claims description 6
- FBOZXECLQNJBKD-ZDUSSCGKSA-N L-methotrexate Chemical compound C=1N=C2N=C(N)N=C(N)C2=NC=1CN(C)C1=CC=C(C(=O)N[C@@H](CCC(O)=O)C(O)=O)C=C1 FBOZXECLQNJBKD-ZDUSSCGKSA-N 0.000 claims description 6
- 239000005517 L01XE01 - Imatinib Substances 0.000 claims description 6
- 239000005411 L01XE02 - Gefitinib Substances 0.000 claims description 6
- 239000005551 L01XE03 - Erlotinib Substances 0.000 claims description 6
- 239000002147 L01XE04 - Sunitinib Substances 0.000 claims description 6
- 239000005511 L01XE05 - Sorafenib Substances 0.000 claims description 6
- 239000002067 L01XE06 - Dasatinib Substances 0.000 claims description 6
- 239000002136 L01XE07 - Lapatinib Substances 0.000 claims description 6
- 239000005536 L01XE08 - Nilotinib Substances 0.000 claims description 6
- 239000003798 L01XE11 - Pazopanib Substances 0.000 claims description 6
- 239000002118 L01XE12 - Vandetanib Substances 0.000 claims description 6
- 239000002145 L01XE14 - Bosutinib Substances 0.000 claims description 6
- 239000002146 L01XE16 - Crizotinib Substances 0.000 claims description 6
- 239000002144 L01XE18 - Ruxolitinib Substances 0.000 claims description 6
- 239000002138 L01XE21 - Regorafenib Substances 0.000 claims description 6
- 239000002137 L01XE24 - Ponatinib Substances 0.000 claims description 6
- 239000002176 L01XE26 - Cabozantinib Substances 0.000 claims description 6
- 239000002177 L01XE27 - Ibrutinib Substances 0.000 claims description 6
- 206010025282 Lymphoedema Diseases 0.000 claims description 6
- 239000005462 Mubritinib Substances 0.000 claims description 6
- ZDZOTLJHXYCWBA-VCVYQWHSSA-N N-debenzoyl-N-(tert-butoxycarbonyl)-10-deacetyltaxol Chemical compound O([C@H]1[C@H]2[C@@](C([C@H](O)C3=C(C)[C@@H](OC(=O)[C@H](O)[C@@H](NC(=O)OC(C)(C)C)C=4C=CC=CC=4)C[C@]1(O)C3(C)C)=O)(C)[C@@H](O)C[C@H]1OC[C@]12OC(=O)C)C(=O)C1=CC=CC=C1 ZDZOTLJHXYCWBA-VCVYQWHSSA-N 0.000 claims description 6
- YJQPYGGHQPGBLI-UHFFFAOYSA-N Novobiocin Natural products O1C(C)(C)C(OC)C(OC(N)=O)C(O)C1OC1=CC=C(C(O)=C(NC(=O)C=2C=C(CC=C(C)C)C(O)=CC=2)C(=O)O2)C2=C1C YJQPYGGHQPGBLI-UHFFFAOYSA-N 0.000 claims description 6
- 206010033128 Ovarian cancer Diseases 0.000 claims description 6
- 206010061535 Ovarian neoplasm Diseases 0.000 claims description 6
- 108091008606 PDGF receptors Proteins 0.000 claims description 6
- 229930012538 Paclitaxel Natural products 0.000 claims description 6
- KMSKQZKKOZQFFG-HSUXVGOQSA-N Pirarubicin Chemical compound O([C@H]1[C@@H](N)C[C@@H](O[C@H]1C)O[C@H]1C[C@@](O)(CC=2C(O)=C3C(=O)C=4C=CC=C(C=4C(=O)C3=C(O)C=21)OC)C(=O)CO)[C@H]1CCCCO1 KMSKQZKKOZQFFG-HSUXVGOQSA-N 0.000 claims description 6
- 102000011653 Platelet-Derived Growth Factor Receptors Human genes 0.000 claims description 6
- RJKFOVLPORLFTN-LEKSSAKUSA-N Progesterone Chemical class C1CC2=CC(=O)CC[C@]2(C)[C@@H]2[C@@H]1[C@@H]1CC[C@H](C(=O)C)[C@@]1(C)CC2 RJKFOVLPORLFTN-LEKSSAKUSA-N 0.000 claims description 6
- 206010060862 Prostate cancer Diseases 0.000 claims description 6
- 208000000236 Prostatic Neoplasms Diseases 0.000 claims description 6
- 208000006265 Renal cell carcinoma Diseases 0.000 claims description 6
- LOGJQOUIVKBFGH-UHFFFAOYSA-N SU6656 Chemical compound C1CCCC(N2)=C1C=C2C=C1C(=O)NC2=CC=C(S(=O)(=O)N(C)C)C=C21 LOGJQOUIVKBFGH-UHFFFAOYSA-N 0.000 claims description 6
- 102000013275 Somatomedins Human genes 0.000 claims description 6
- ZSJLQEPLLKMAKR-UHFFFAOYSA-N Streptozotocin Natural products O=NN(C)C(=O)NC1C(O)OC(CO)C(O)C1O ZSJLQEPLLKMAKR-UHFFFAOYSA-N 0.000 claims description 6
- 229940123237 Taxane Drugs 0.000 claims description 6
- BPEGJWRSRHCHSN-UHFFFAOYSA-N Temozolomide Chemical compound O=C1N(C)N=NC2=C(C(N)=O)N=CN21 BPEGJWRSRHCHSN-UHFFFAOYSA-N 0.000 claims description 6
- FOCVUCIESVLUNU-UHFFFAOYSA-N Thiotepa Chemical compound C1CN1P(N1CC1)(=S)N1CC1 FOCVUCIESVLUNU-UHFFFAOYSA-N 0.000 claims description 6
- 239000004012 Tofacitinib Substances 0.000 claims description 6
- 208000007097 Urinary Bladder Neoplasms Diseases 0.000 claims description 6
- JXLYSJRDGCGARV-WWYNWVTFSA-N Vinblastine Natural products O=C(O[C@H]1[C@](O)(C(=O)OC)[C@@H]2N(C)c3c(cc(c(OC)c3)[C@]3(C(=O)OC)c4[nH]c5c(c4CCN4C[C@](O)(CC)C[C@H](C3)C4)cccc5)[C@@]32[C@H]2[C@@]1(CC)C=CCN2CC3)C JXLYSJRDGCGARV-WWYNWVTFSA-N 0.000 claims description 6
- 229940122803 Vinca alkaloid Drugs 0.000 claims description 6
- 229930183665 actinomycin Natural products 0.000 claims description 6
- 229950009557 adavosertib Drugs 0.000 claims description 6
- 210000004100 adrenal gland Anatomy 0.000 claims description 6
- 229960002833 aflibercept Drugs 0.000 claims description 6
- 108010081667 aflibercept Proteins 0.000 claims description 6
- 229950008459 alacizumab pegol Drugs 0.000 claims description 6
- 229960000473 altretamine Drugs 0.000 claims description 6
- BBDAGFIXKZCXAH-CCXZUQQUSA-N ancitabine Chemical compound N=C1C=CN2[C@@H]3O[C@H](CO)[C@@H](O)[C@@H]3OC2=N1 BBDAGFIXKZCXAH-CCXZUQQUSA-N 0.000 claims description 6
- 229950000242 ancitabine Drugs 0.000 claims description 6
- 239000003098 androgen Substances 0.000 claims description 6
- 230000002491 angiogenic effect Effects 0.000 claims description 6
- 229940045799 anthracyclines and related substance Drugs 0.000 claims description 6
- 230000002280 anti-androgenic effect Effects 0.000 claims description 6
- 230000003432 anti-folate effect Effects 0.000 claims description 6
- 239000000051 antiandrogen Substances 0.000 claims description 6
- 229940127074 antifolate Drugs 0.000 claims description 6
- 229940045719 antineoplastic alkylating agent nitrosoureas Drugs 0.000 claims description 6
- 229950006900 aprutumab ixadotin Drugs 0.000 claims description 6
- 239000003886 aromatase inhibitor Substances 0.000 claims description 6
- 229960003005 axitinib Drugs 0.000 claims description 6
- RITAVMQDGBJQJZ-FMIVXFBMSA-N axitinib Chemical compound CNC(=O)C1=CC=CC=C1SC1=CC=C(C(\C=C\C=2N=CC=CC=2)=NN2)C2=C1 RITAVMQDGBJQJZ-FMIVXFBMSA-N 0.000 claims description 6
- 229960002756 azacitidine Drugs 0.000 claims description 6
- 150000001541 aziridines Chemical class 0.000 claims description 6
- 229950009566 bemarituzumab Drugs 0.000 claims description 6
- 230000015572 biosynthetic process Effects 0.000 claims description 6
- OYVAGSVQBOHSSS-UAPAGMARSA-O bleomycin A2 Chemical class N([C@H](C(=O)N[C@H](C)[C@@H](O)[C@H](C)C(=O)N[C@@H]([C@H](O)C)C(=O)NCCC=1SC=C(N=1)C=1SC=C(N=1)C(=O)NCCC[S+](C)C)[C@@H](O[C@H]1[C@H]([C@@H](O)[C@H](O)[C@H](CO)O1)O[C@@H]1[C@H]([C@@H](OC(N)=O)[C@H](O)[C@@H](CO)O1)O)C=1N=CNC=1)C(=O)C1=NC([C@H](CC(N)=O)NC[C@H](N)C(N)=O)=NC(N)=C1C OYVAGSVQBOHSSS-UAPAGMARSA-O 0.000 claims description 6
- 229960003736 bosutinib Drugs 0.000 claims description 6
- UBPYILGKFZZVDX-UHFFFAOYSA-N bosutinib Chemical compound C1=C(Cl)C(OC)=CC(NC=2C3=CC(OC)=C(OCCCN4CCN(C)CC4)C=C3N=CC=2C#N)=C1Cl UBPYILGKFZZVDX-UHFFFAOYSA-N 0.000 claims description 6
- 229960002092 busulfan Drugs 0.000 claims description 6
- 229960001292 cabozantinib Drugs 0.000 claims description 6
- ONIQOQHATWINJY-UHFFFAOYSA-N cabozantinib Chemical compound C=12C=C(OC)C(OC)=CC2=NC=CC=1OC(C=C1)=CC=C1NC(=O)C1(C(=O)NC=2C=CC(F)=CC=2)CC1 ONIQOQHATWINJY-UHFFFAOYSA-N 0.000 claims description 6
- VSJKWCGYPAHWDS-FQEVSTJZSA-N camptothecin Chemical compound C1=CC=C2C=C(CN3C4=CC5=C(C3=O)COC(=O)[C@]5(O)CC)C4=NC2=C1 VSJKWCGYPAHWDS-FQEVSTJZSA-N 0.000 claims description 6
- 229940127093 camptothecin Drugs 0.000 claims description 6
- 229960004117 capecitabine Drugs 0.000 claims description 6
- 229960004562 carboplatin Drugs 0.000 claims description 6
- 229960005243 carmustine Drugs 0.000 claims description 6
- 229960004630 chlorambucil Drugs 0.000 claims description 6
- JCKYGMPEJWAADB-UHFFFAOYSA-N chlorambucil Chemical compound OC(=O)CCCC1=CC=C(N(CCCl)CCCl)C=C1 JCKYGMPEJWAADB-UHFFFAOYSA-N 0.000 claims description 6
- 229950006647 cixutumumab Drugs 0.000 claims description 6
- 229960002436 cladribine Drugs 0.000 claims description 6
- 229960000928 clofarabine Drugs 0.000 claims description 6
- WDDPHFBMKLOVOX-AYQXTPAHSA-N clofarabine Chemical compound C1=NC=2C(N)=NC(Cl)=NC=2N1[C@@H]1O[C@H](CO)[C@@H](O)[C@@H]1F WDDPHFBMKLOVOX-AYQXTPAHSA-N 0.000 claims description 6
- 229960002271 cobimetinib Drugs 0.000 claims description 6
- RESIMIUSNACMNW-BXRWSSRYSA-N cobimetinib fumarate Chemical compound OC(=O)\C=C\C(O)=O.C1C(O)([C@H]2NCCCC2)CN1C(=O)C1=CC=C(F)C(F)=C1NC1=CC=C(I)C=C1F.C1C(O)([C@H]2NCCCC2)CN1C(=O)C1=CC=C(F)C(F)=C1NC1=CC=C(I)C=C1F RESIMIUSNACMNW-BXRWSSRYSA-N 0.000 claims description 6
- 239000003246 corticosteroid Substances 0.000 claims description 6
- 229960005061 crizotinib Drugs 0.000 claims description 6
- KTEIFNKAUNYNJU-GFCCVEGCSA-N crizotinib Chemical compound O([C@H](C)C=1C(=C(F)C=CC=1Cl)Cl)C(C(=NC=1)N)=CC=1C(=C1)C=NN1C1CCNCC1 KTEIFNKAUNYNJU-GFCCVEGCSA-N 0.000 claims description 6
- 229960004397 cyclophosphamide Drugs 0.000 claims description 6
- 229960000684 cytarabine Drugs 0.000 claims description 6
- 229960003901 dacarbazine Drugs 0.000 claims description 6
- 229960002482 dalotuzumab Drugs 0.000 claims description 6
- 229960002448 dasatinib Drugs 0.000 claims description 6
- 229960000975 daunorubicin Drugs 0.000 claims description 6
- STQGQHZAVUOBTE-VGBVRHCVSA-N daunorubicin Chemical compound O([C@H]1C[C@@](O)(CC=2C(O)=C3C(=O)C=4C=CC=C(C=4C(=O)C3=C(O)C=21)OC)C(C)=O)[C@H]1C[C@H](N)[C@H](O)[C@H](C)O1 STQGQHZAVUOBTE-VGBVRHCVSA-N 0.000 claims description 6
- 229960003603 decitabine Drugs 0.000 claims description 6
- 229950008925 depatuxizumab mafodotin Drugs 0.000 claims description 6
- 229960003957 dexamethasone Drugs 0.000 claims description 6
- UREBDLICKHMUKA-CXSFZGCWSA-N dexamethasone Chemical compound C1CC2=CC(=O)C=C[C@]2(C)[C@]2(F)[C@@H]1[C@@H]1C[C@@H](C)[C@@](C(=O)CO)(O)[C@@]1(C)C[C@@H]2O UREBDLICKHMUKA-CXSFZGCWSA-N 0.000 claims description 6
- 229950002389 diaziquone Drugs 0.000 claims description 6
- VSJKWCGYPAHWDS-UHFFFAOYSA-N dl-camptothecin Natural products C1=CC=C2C=C(CN3C4=CC5=C(C3=O)COC(=O)C5(O)CC)C4=NC2=C1 VSJKWCGYPAHWDS-UHFFFAOYSA-N 0.000 claims description 6
- 229960003668 docetaxel Drugs 0.000 claims description 6
- 229950011487 enocitabine Drugs 0.000 claims description 6
- 229950000521 entrectinib Drugs 0.000 claims description 6
- 229960001904 epirubicin Drugs 0.000 claims description 6
- 229950004444 erdafitinib Drugs 0.000 claims description 6
- 229960001433 erlotinib Drugs 0.000 claims description 6
- AAKJLRGGTJKAMG-UHFFFAOYSA-N erlotinib Chemical compound C=12C=C(OCCOC)C(OCCOC)=CC2=NC=NC=1NC1=CC=CC(C#C)=C1 AAKJLRGGTJKAMG-UHFFFAOYSA-N 0.000 claims description 6
- 229940011871 estrogen Drugs 0.000 claims description 6
- 239000000262 estrogen Substances 0.000 claims description 6
- VJJPUSNTGOMMGY-MRVIYFEKSA-N etoposide Chemical compound COC1=C(O)C(OC)=CC([C@@H]2C3=CC=4OCOC=4C=C3[C@@H](O[C@H]3[C@@H]([C@@H](O)[C@@H]4O[C@H](C)OC[C@H]4O3)O)[C@@H]3[C@@H]2C(OC3)=O)=C1 VJJPUSNTGOMMGY-MRVIYFEKSA-N 0.000 claims description 6
- 229960005420 etoposide Drugs 0.000 claims description 6
- 229950008085 figitumumab Drugs 0.000 claims description 6
- 150000005699 fluoropyrimidines Chemical class 0.000 claims description 6
- 239000004052 folic acid antagonist Substances 0.000 claims description 6
- YAKWPXVTIGTRJH-UHFFFAOYSA-N fotemustine Chemical compound CCOP(=O)(OCC)C(C)NC(=O)N(CCCl)N=O YAKWPXVTIGTRJH-UHFFFAOYSA-N 0.000 claims description 6
- 229960004783 fotemustine Drugs 0.000 claims description 6
- 229950004003 fresolimumab Drugs 0.000 claims description 6
- 229950002140 futuximab Drugs 0.000 claims description 6
- 229950004896 ganitumab Drugs 0.000 claims description 6
- 229960002584 gefitinib Drugs 0.000 claims description 6
- XGALLCVXEZPNRQ-UHFFFAOYSA-N gefitinib Chemical compound C=12C=C(OCCCN3CCOCC3)C(OC)=CC2=NC=NC=1NC1=CC=C(F)C(Cl)=C1 XGALLCVXEZPNRQ-UHFFFAOYSA-N 0.000 claims description 6
- 229960005277 gemcitabine Drugs 0.000 claims description 6
- SDUQYLNIPVEERB-QPPQHZFASA-N gemcitabine Chemical compound O=C1N=C(N)C=CN1[C@H]1C(F)(F)[C@H](O)[C@@H](CO)O1 SDUQYLNIPVEERB-QPPQHZFASA-N 0.000 claims description 6
- 206010073071 hepatocellular carcinoma Diseases 0.000 claims description 6
- UUVWYPNAQBNQJQ-UHFFFAOYSA-N hexamethylmelamine Chemical compound CN(C)C1=NC(N(C)C)=NC(N(C)C)=N1 UUVWYPNAQBNQJQ-UHFFFAOYSA-N 0.000 claims description 6
- 229940088597 hormone Drugs 0.000 claims description 6
- 239000005556 hormone Substances 0.000 claims description 6
- 239000003689 hormone receptor blocking agent Substances 0.000 claims description 6
- 229960001507 ibrutinib Drugs 0.000 claims description 6
- XYFPWWZEPKGCCK-GOSISDBHSA-N ibrutinib Chemical compound C1=2C(N)=NC=NC=2N([C@H]2CN(CCC2)C(=O)C=C)N=C1C(C=C1)=CC=C1OC1=CC=CC=C1 XYFPWWZEPKGCCK-GOSISDBHSA-N 0.000 claims description 6
- 229950006359 icrucumab Drugs 0.000 claims description 6
- 229960000908 idarubicin Drugs 0.000 claims description 6
- 229960001101 ifosfamide Drugs 0.000 claims description 6
- HOMGKSMUEGBAAB-UHFFFAOYSA-N ifosfamide Chemical compound ClCCNP1(=O)OCCCN1CCCl HOMGKSMUEGBAAB-UHFFFAOYSA-N 0.000 claims description 6
- KTUFNOKKBVMGRW-UHFFFAOYSA-N imatinib Chemical compound C1CN(C)CCN1CC1=CC=C(C(=O)NC=2C=C(NC=3N=C(C=CN=3)C=3C=NC=CC=3)C(C)=CC=2)C=C1 KTUFNOKKBVMGRW-UHFFFAOYSA-N 0.000 claims description 6
- 229960002411 imatinib Drugs 0.000 claims description 6
- 229950005646 imgatuzumab Drugs 0.000 claims description 6
- 239000003112 inhibitor Substances 0.000 claims description 6
- 229960004768 irinotecan Drugs 0.000 claims description 6
- UWKQSNNFCGGAFS-XIFFEERXSA-N irinotecan Chemical compound C1=C2C(CC)=C3CN(C(C4=C([C@@](C(=O)OC4)(O)CC)C=4)=O)C=4C3=NC2=CC=C1OC(=O)N(CC1)CCC1N1CCCCC1 UWKQSNNFCGGAFS-XIFFEERXSA-N 0.000 claims description 6
- 229950009645 istiratumab Drugs 0.000 claims description 6
- 229960004891 lapatinib Drugs 0.000 claims description 6
- BCFGMOOMADDAQU-UHFFFAOYSA-N lapatinib Chemical compound O1C(CNCCS(=O)(=O)C)=CC=C1C1=CC=C(N=CN=C2NC=3C=C(Cl)C(OCC=4C=C(F)C=CC=4)=CC=3)C2=C1 BCFGMOOMADDAQU-UHFFFAOYSA-N 0.000 claims description 6
- 229950010860 laprituximab emtansine Drugs 0.000 claims description 6
- 229960003784 lenvatinib Drugs 0.000 claims description 6
- WOSKHXYHFSIKNG-UHFFFAOYSA-N lenvatinib Chemical compound C=12C=C(C(N)=O)C(OC)=CC2=NC=CC=1OC(C=C1Cl)=CC=C1NC(=O)NC1CC1 WOSKHXYHFSIKNG-UHFFFAOYSA-N 0.000 claims description 6
- 229960002247 lomustine Drugs 0.000 claims description 6
- 208000002502 lymphedema Diseases 0.000 claims description 6
- 229950008001 matuzumab Drugs 0.000 claims description 6
- 229960001924 melphalan Drugs 0.000 claims description 6
- SGDBTWWWUNNDEQ-LBPRGKRZSA-N melphalan Chemical compound OC(=O)[C@@H](N)CC1=CC=C(N(CCCl)CCCl)C=C1 SGDBTWWWUNNDEQ-LBPRGKRZSA-N 0.000 claims description 6
- GLVAUDGFNGKCSF-UHFFFAOYSA-N mercaptopurine Chemical compound S=C1NC=NC2=C1NC=N2 GLVAUDGFNGKCSF-UHFFFAOYSA-N 0.000 claims description 6
- 229960001428 mercaptopurine Drugs 0.000 claims description 6
- 208000037819 metastatic cancer Diseases 0.000 claims description 6
- 208000011575 metastatic malignant neoplasm Diseases 0.000 claims description 6
- 229950005555 metelimumab Drugs 0.000 claims description 6
- 229960000485 methotrexate Drugs 0.000 claims description 6
- 229960004584 methylprednisolone Drugs 0.000 claims description 6
- 229960004857 mitomycin Drugs 0.000 claims description 6
- QXYYYPFGTSJXNS-UHFFFAOYSA-N mitozolomide Chemical compound N1=NN(CCCl)C(=O)N2C1=C(C(=O)N)N=C2 QXYYYPFGTSJXNS-UHFFFAOYSA-N 0.000 claims description 6
- 229950005967 mitozolomide Drugs 0.000 claims description 6
- 229950005674 modotuximab Drugs 0.000 claims description 6
- 229950002212 mubritinib Drugs 0.000 claims description 6
- ZTFBIUXIQYRUNT-MDWZMJQESA-N mubritinib Chemical compound C1=CC(C(F)(F)F)=CC=C1\C=C\C1=NC(COC=2C=CC(CCCCN3N=NC=C3)=CC=2)=CO1 ZTFBIUXIQYRUNT-MDWZMJQESA-N 0.000 claims description 6
- OLAHOMJCDNXHFI-UHFFFAOYSA-N n'-(3,5-dimethoxyphenyl)-n'-[3-(1-methylpyrazol-4-yl)quinoxalin-6-yl]-n-propan-2-ylethane-1,2-diamine Chemical compound COC1=CC(OC)=CC(N(CCNC(C)C)C=2C=C3N=C(C=NC3=CC=2)C2=CN(C)N=C2)=C1 OLAHOMJCDNXHFI-UHFFFAOYSA-N 0.000 claims description 6
- HAYYBYPASCDWEQ-UHFFFAOYSA-N n-[5-[(3,5-difluorophenyl)methyl]-1h-indazol-3-yl]-4-(4-methylpiperazin-1-yl)-2-(oxan-4-ylamino)benzamide Chemical compound C1CN(C)CCN1C(C=C1NC2CCOCC2)=CC=C1C(=O)NC(C1=C2)=NNC1=CC=C2CC1=CC(F)=CC(F)=C1 HAYYBYPASCDWEQ-UHFFFAOYSA-N 0.000 claims description 6
- 229940121585 naxitamab Drugs 0.000 claims description 6
- 229960000513 necitumumab Drugs 0.000 claims description 6
- 229960000801 nelarabine Drugs 0.000 claims description 6
- IXOXBSCIXZEQEQ-UHTZMRCNSA-N nelarabine Chemical compound C1=NC=2C(OC)=NC(N)=NC=2N1[C@@H]1O[C@H](CO)[C@@H](O)[C@@H]1O IXOXBSCIXZEQEQ-UHTZMRCNSA-N 0.000 claims description 6
- 229960001346 nilotinib Drugs 0.000 claims description 6
- HHZIURLSWUIHRB-UHFFFAOYSA-N nilotinib Chemical compound C1=NC(C)=CN1C1=CC(NC(=O)C=2C=C(NC=3N=C(C=CN=3)C=3C=NC=CC=3)C(C)=CC=2)=CC(C(F)(F)F)=C1 HHZIURLSWUIHRB-UHFFFAOYSA-N 0.000 claims description 6
- 229950010203 nimotuzumab Drugs 0.000 claims description 6
- 229910052757 nitrogen Inorganic materials 0.000 claims description 6
- 229960003301 nivolumab Drugs 0.000 claims description 6
- 229960002950 novobiocin Drugs 0.000 claims description 6
- YJQPYGGHQPGBLI-KGSXXDOSSA-N novobiocin Chemical compound O1C(C)(C)[C@H](OC)[C@@H](OC(N)=O)[C@@H](O)[C@@H]1OC1=CC=C(C(O)=C(NC(=O)C=2C=C(CC=C(C)C)C(O)=CC=2)C(=O)O2)C2=C1C YJQPYGGHQPGBLI-KGSXXDOSSA-N 0.000 claims description 6
- 229950008516 olaratumab Drugs 0.000 claims description 6
- DWAFYCQODLXJNR-BNTLRKBRSA-L oxaliplatin Chemical compound O1C(=O)C(=O)O[Pt]11N[C@@H]2CCCC[C@H]2N1 DWAFYCQODLXJNR-BNTLRKBRSA-L 0.000 claims description 6
- 229960001756 oxaliplatin Drugs 0.000 claims description 6
- 229960001592 paclitaxel Drugs 0.000 claims description 6
- 208000008443 pancreatic carcinoma Diseases 0.000 claims description 6
- 229960000639 pazopanib Drugs 0.000 claims description 6
- CUIHSIWYWATEQL-UHFFFAOYSA-N pazopanib Chemical compound C1=CC2=C(C)N(C)N=C2C=C1N(C)C(N=1)=CC=NC=1NC1=CC=C(C)C(S(N)(=O)=O)=C1 CUIHSIWYWATEQL-UHFFFAOYSA-N 0.000 claims description 6
- 229960003407 pegaptanib Drugs 0.000 claims description 6
- 229960005079 pemetrexed Drugs 0.000 claims description 6
- QOFFJEBXNKRSPX-ZDUSSCGKSA-N pemetrexed Chemical compound C1=N[C]2NC(N)=NC(=O)C2=C1CCC1=CC=C(C(=O)N[C@@H](CCC(O)=O)C(O)=O)C=C1 QOFFJEBXNKRSPX-ZDUSSCGKSA-N 0.000 claims description 6
- 229960002340 pentostatin Drugs 0.000 claims description 6
- FPVKHBSQESCIEP-JQCXWYLXSA-N pentostatin Chemical compound C1[C@H](O)[C@@H](CO)O[C@H]1N1C(N=CNC[C@H]2O)=C2N=C1 FPVKHBSQESCIEP-JQCXWYLXSA-N 0.000 claims description 6
- 229960001221 pirarubicin Drugs 0.000 claims description 6
- 229960001131 ponatinib Drugs 0.000 claims description 6
- PHXJVRSECIGDHY-UHFFFAOYSA-N ponatinib Chemical compound C1CN(C)CCN1CC(C(=C1)C(F)(F)F)=CC=C1NC(=O)C1=CC=C(C)C(C#CC=2N3N=CC=CC3=NC=2)=C1 PHXJVRSECIGDHY-UHFFFAOYSA-N 0.000 claims description 6
- 229960005205 prednisolone Drugs 0.000 claims description 6
- OIGNJSKKLXVSLS-VWUMJDOOSA-N prednisolone Chemical compound O=C1C=C[C@]2(C)[C@H]3[C@@H](O)C[C@](C)([C@@](CC4)(O)C(=O)CO)[C@@H]4[C@@H]3CCC2=C1 OIGNJSKKLXVSLS-VWUMJDOOSA-N 0.000 claims description 6
- CPTBDICYNRMXFX-UHFFFAOYSA-N procarbazine Chemical compound CNNCC1=CC=C(C(=O)NC(C)C)C=C1 CPTBDICYNRMXFX-UHFFFAOYSA-N 0.000 claims description 6
- 229960000624 procarbazine Drugs 0.000 claims description 6
- ZADWXFSZEAPBJS-UHFFFAOYSA-N racemic N-methyl tryptophan Natural products C1=CC=C2N(C)C=C(CC(N)C(O)=O)C2=C1 ZADWXFSZEAPBJS-UHFFFAOYSA-N 0.000 claims description 6
- 229960002633 ramucirumab Drugs 0.000 claims description 6
- 229960003876 ranibizumab Drugs 0.000 claims description 6
- 230000009467 reduction Effects 0.000 claims description 6
- 229960004836 regorafenib Drugs 0.000 claims description 6
- FNHKPVJBJVTLMP-UHFFFAOYSA-N regorafenib Chemical compound C1=NC(C(=O)NC)=CC(OC=2C=C(F)C(NC(=O)NC=3C=C(C(Cl)=CC=3)C(F)(F)F)=CC=2)=C1 FNHKPVJBJVTLMP-UHFFFAOYSA-N 0.000 claims description 6
- 229950001808 robatumumab Drugs 0.000 claims description 6
- 229960000215 ruxolitinib Drugs 0.000 claims description 6
- HFNKQEVNSGCOJV-OAHLLOKOSA-N ruxolitinib Chemical compound C1([C@@H](CC#N)N2N=CC(=C2)C=2C=3C=CNC=3N=CN=2)CCCC1 HFNKQEVNSGCOJV-OAHLLOKOSA-N 0.000 claims description 6
- FVLVBPDQNARYJU-UHFFFAOYSA-N semustine Chemical compound CC1CCC(NC(=O)N(CCCl)N=O)CC1 FVLVBPDQNARYJU-UHFFFAOYSA-N 0.000 claims description 6
- 229960003440 semustine Drugs 0.000 claims description 6
- NHXLMOGPVYXJNR-ATOGVRKGSA-N somatostatin Chemical class C([C@H]1C(=O)N[C@H](C(N[C@@H](CO)C(=O)N[C@@H](CSSC[C@@H](C(=O)N[C@@H](CCCCN)C(=O)N[C@@H](CC(N)=O)C(=O)N[C@@H](CC=2C=CC=CC=2)C(=O)N[C@@H](CC=2C=CC=CC=2)C(=O)N[C@@H](CC=2C3=CC=CC=C3NC=2)C(=O)N[C@@H](CCCCN)C(=O)N[C@H](C(=O)N1)[C@@H](C)O)NC(=O)CNC(=O)[C@H](C)N)C(O)=O)=O)[C@H](O)C)C1=CC=CC=C1 NHXLMOGPVYXJNR-ATOGVRKGSA-N 0.000 claims description 6
- 229960003787 sorafenib Drugs 0.000 claims description 6
- 229960001052 streptozocin Drugs 0.000 claims description 6
- ZSJLQEPLLKMAKR-GKHCUFPYSA-N streptozocin Chemical compound O=NN(C)C(=O)N[C@H]1[C@@H](O)O[C@H](CO)[C@@H](O)[C@@H]1O ZSJLQEPLLKMAKR-GKHCUFPYSA-N 0.000 claims description 6
- 229960001796 sunitinib Drugs 0.000 claims description 6
- WINHZLLDWRZWRT-ATVHPVEESA-N sunitinib Chemical compound CCN(CC)CCNC(=O)C1=C(C)NC(\C=C/2C3=CC(F)=CC=C3NC\2=O)=C1C WINHZLLDWRZWRT-ATVHPVEESA-N 0.000 claims description 6
- RCINICONZNJXQF-MZXODVADSA-N taxol Chemical compound O([C@@H]1[C@@]2(C[C@@H](C(C)=C(C2(C)C)[C@H](C([C@]2(C)[C@@H](O)C[C@H]3OC[C@]3([C@H]21)OC(C)=O)=O)OC(=O)C)OC(=O)[C@H](O)[C@@H](NC(=O)C=1C=CC=CC=1)C=1C=CC=CC=1)O)C(=O)C1=CC=CC=C1 RCINICONZNJXQF-MZXODVADSA-N 0.000 claims description 6
- 229960004964 temozolomide Drugs 0.000 claims description 6
- 229960001278 teniposide Drugs 0.000 claims description 6
- NRUKOCRGYNPUPR-QBPJDGROSA-N teniposide Chemical compound COC1=C(O)C(OC)=CC([C@@H]2C3=CC=4OCOC=4C=C3[C@@H](O[C@H]3[C@@H]([C@@H](O)[C@@H]4O[C@@H](OC[C@H]4O3)C=3SC=CC=3)O)[C@@H]3[C@@H]2C(OC3)=O)=C1 NRUKOCRGYNPUPR-QBPJDGROSA-N 0.000 claims description 6
- 150000004905 tetrazines Chemical class 0.000 claims description 6
- 229960001196 thiotepa Drugs 0.000 claims description 6
- 229960003087 tioguanine Drugs 0.000 claims description 6
- 229960001350 tofacitinib Drugs 0.000 claims description 6
- UJLAWZDWDVHWOW-YPMHNXCESA-N tofacitinib Chemical compound C[C@@H]1CCN(C(=O)CC#N)C[C@@H]1N(C)C1=NC=NC2=C1C=CN2 UJLAWZDWDVHWOW-YPMHNXCESA-N 0.000 claims description 6
- 229940060960 tomuzotuximab Drugs 0.000 claims description 6
- 229960000303 topotecan Drugs 0.000 claims description 6
- UCFGDBYHRUNTLO-QHCPKHFHSA-N topotecan Chemical compound C1=C(O)C(CN(C)C)=C2C=C(CN3C4=CC5=C(C3=O)COC(=O)[C@]5(O)CC)C4=NC2=C1 UCFGDBYHRUNTLO-QHCPKHFHSA-N 0.000 claims description 6
- 229950005808 tovetumab Drugs 0.000 claims description 6
- 229960000575 trastuzumab Drugs 0.000 claims description 6
- 201000005112 urinary bladder cancer Diseases 0.000 claims description 6
- 229960000241 vandetanib Drugs 0.000 claims description 6
- UHTHHESEBZOYNR-UHFFFAOYSA-N vandetanib Chemical compound COC1=CC(C(/N=CN2)=N/C=3C(=CC(Br)=CC=3)F)=C2C=C1OCC1CCN(C)CC1 UHTHHESEBZOYNR-UHFFFAOYSA-N 0.000 claims description 6
- 229960003048 vinblastine Drugs 0.000 claims description 6
- JXLYSJRDGCGARV-XQKSVPLYSA-N vincaleukoblastine Chemical compound C([C@@H](C[C@]1(C(=O)OC)C=2C(=CC3=C([C@]45[C@H]([C@@]([C@H](OC(C)=O)[C@]6(CC)C=CCN([C@H]56)CC4)(O)C(=O)OC)N3C)C=2)OC)C[C@@](C2)(O)CC)N2CCC2=C1NC1=CC=CC=C21 JXLYSJRDGCGARV-XQKSVPLYSA-N 0.000 claims description 6
- 229960004528 vincristine Drugs 0.000 claims description 6
- OGWKCGZFUXNPDA-XQKSVPLYSA-N vincristine Chemical compound C([N@]1C[C@@H](C[C@]2(C(=O)OC)C=3C(=CC4=C([C@]56[C@H]([C@@]([C@H](OC(C)=O)[C@]7(CC)C=CCN([C@H]67)CC5)(O)C(=O)OC)N4C=O)C=3)OC)C[C@@](C1)(O)CC)CC1=C2NC2=CC=CC=C12 OGWKCGZFUXNPDA-XQKSVPLYSA-N 0.000 claims description 6
- OGWKCGZFUXNPDA-UHFFFAOYSA-N vincristine Natural products C1C(CC)(O)CC(CC2(C(=O)OC)C=3C(=CC4=C(C56C(C(C(OC(C)=O)C7(CC)C=CCN(C67)CC5)(O)C(=O)OC)N4C=O)C=3)OC)CN1CCC1=C2NC2=CC=CC=C12 OGWKCGZFUXNPDA-UHFFFAOYSA-N 0.000 claims description 6
- 229960004355 vindesine Drugs 0.000 claims description 6
- UGGWPQSBPIFKDZ-KOTLKJBCSA-N vindesine Chemical compound C([C@@H](C[C@]1(C(=O)OC)C=2C(=CC3=C([C@]45[C@H]([C@@]([C@H](O)[C@]6(CC)C=CCN([C@H]56)CC4)(O)C(N)=O)N3C)C=2)OC)C[C@@](C2)(O)CC)N2CCC2=C1N=C1[C]2C=CC=C1 UGGWPQSBPIFKDZ-KOTLKJBCSA-N 0.000 claims description 6
- 229960002066 vinorelbine Drugs 0.000 claims description 6
- 229950008250 zalutumumab Drugs 0.000 claims description 6
- 101100080540 Mus musculus Nrp2 gene Proteins 0.000 claims description 5
- 230000000295 complement effect Effects 0.000 claims description 5
- 230000006870 function Effects 0.000 claims description 5
- 208000005017 glioblastoma Diseases 0.000 claims description 5
- 230000028993 immune response Effects 0.000 claims description 5
- 230000035772 mutation Effects 0.000 claims description 5
- 102000004169 proteins and genes Human genes 0.000 claims description 5
- ZADWXFSZEAPBJS-SNVBAGLBSA-N (2r)-2-amino-3-(1-methylindol-3-yl)propanoic acid Chemical compound C1=CC=C2N(C)C=C(C[C@@H](N)C(O)=O)C2=C1 ZADWXFSZEAPBJS-SNVBAGLBSA-N 0.000 claims description 4
- YPBKTZBXSBLTDK-PKNBQFBNSA-N (3e)-3-[(3-bromo-4-fluoroanilino)-nitrosomethylidene]-4-[2-(sulfamoylamino)ethylamino]-1,2,5-oxadiazole Chemical compound NS(=O)(=O)NCCNC1=NON\C1=C(N=O)/NC1=CC=C(F)C(Br)=C1 YPBKTZBXSBLTDK-PKNBQFBNSA-N 0.000 claims description 4
- TZCPCKNHXULUIY-RGULYWFUSA-N 1,2-distearoyl-sn-glycero-3-phosphoserine Chemical compound CCCCCCCCCCCCCCCCCC(=O)OC[C@H](COP(O)(=O)OC[C@H](N)C(O)=O)OC(=O)CCCCCCCCCCCCCCCCC TZCPCKNHXULUIY-RGULYWFUSA-N 0.000 claims description 4
- BJHCYTJNPVGSBZ-YXSASFKJSA-N 1-[4-[6-amino-5-[(Z)-methoxyiminomethyl]pyrimidin-4-yl]oxy-2-chlorophenyl]-3-ethylurea Chemical compound CCNC(=O)Nc1ccc(Oc2ncnc(N)c2\C=N/OC)cc1Cl BJHCYTJNPVGSBZ-YXSASFKJSA-N 0.000 claims description 4
- 108010082808 4-1BB Ligand Proteins 0.000 claims description 4
- 102100030310 5,6-dihydroxyindole-2-carboxylic acid oxidase Human genes 0.000 claims description 4
- 208000031261 Acute myeloid leukaemia Diseases 0.000 claims description 4
- 108010028006 B-Cell Activating Factor Proteins 0.000 claims description 4
- 102100038080 B-cell receptor CD22 Human genes 0.000 claims description 4
- 102100024222 B-lymphocyte antigen CD19 Human genes 0.000 claims description 4
- 102100022005 B-lymphocyte antigen CD20 Human genes 0.000 claims description 4
- 229940125565 BMS-986016 Drugs 0.000 claims description 4
- 102100021663 Baculoviral IAP repeat-containing protein 5 Human genes 0.000 claims description 4
- 101710149863 C-C chemokine receptor type 4 Proteins 0.000 claims description 4
- 102100024217 CAMPATH-1 antigen Human genes 0.000 claims description 4
- 102100032976 CCR4-NOT transcription complex subunit 6 Human genes 0.000 claims description 4
- 229940116741 CD137 agonist Drugs 0.000 claims description 4
- 102100038077 CD226 antigen Human genes 0.000 claims description 4
- 229940121697 CD27 agonist Drugs 0.000 claims description 4
- 102100027207 CD27 antigen Human genes 0.000 claims description 4
- 229940123205 CD28 agonist Drugs 0.000 claims description 4
- 229940123189 CD40 agonist Drugs 0.000 claims description 4
- 108010065524 CD52 Antigen Proteins 0.000 claims description 4
- 101100454808 Caenorhabditis elegans lgg-2 gene Proteins 0.000 claims description 4
- 101100217502 Caenorhabditis elegans lgg-3 gene Proteins 0.000 claims description 4
- 229940124957 Cervarix Drugs 0.000 claims description 4
- 241000709698 Coxsackievirus A21 Species 0.000 claims description 4
- 108700022150 Designed Ankyrin Repeat Proteins Proteins 0.000 claims description 4
- 229940124884 Engerix-B Drugs 0.000 claims description 4
- 108010001687 Enterotoxin Receptors Proteins 0.000 claims description 4
- 108010066687 Epithelial Cell Adhesion Molecule Proteins 0.000 claims description 4
- 102000018651 Epithelial Cell Adhesion Molecule Human genes 0.000 claims description 4
- 108091008794 FGF receptors Proteins 0.000 claims description 4
- 102000044168 Fibroblast Growth Factor Receptor Human genes 0.000 claims description 4
- 206010016654 Fibrosis Diseases 0.000 claims description 4
- 102000010451 Folate receptor alpha Human genes 0.000 claims description 4
- 108050001931 Folate receptor alpha Proteins 0.000 claims description 4
- 229940124897 Gardasil Drugs 0.000 claims description 4
- 208000032612 Glial tumor Diseases 0.000 claims description 4
- 201000010915 Glioblastoma multiforme Diseases 0.000 claims description 4
- 206010018338 Glioma Diseases 0.000 claims description 4
- 102100041003 Glutamate carboxypeptidase 2 Human genes 0.000 claims description 4
- ZWZWYGMENQVNFU-UHFFFAOYSA-N Glycerophosphorylserin Natural products OC(=O)C(N)COP(O)(=O)OCC(O)CO ZWZWYGMENQVNFU-UHFFFAOYSA-N 0.000 claims description 4
- 208000009329 Graft vs Host Disease Diseases 0.000 claims description 4
- 102100022662 Guanylyl cyclase C Human genes 0.000 claims description 4
- 102100030595 HLA class II histocompatibility antigen gamma chain Human genes 0.000 claims description 4
- 241000282412 Homo Species 0.000 claims description 4
- 101000773083 Homo sapiens 5,6-dihydroxyindole-2-carboxylic acid oxidase Proteins 0.000 claims description 4
- 101000884305 Homo sapiens B-cell receptor CD22 Proteins 0.000 claims description 4
- 101000980825 Homo sapiens B-lymphocyte antigen CD19 Proteins 0.000 claims description 4
- 101000897405 Homo sapiens B-lymphocyte antigen CD20 Proteins 0.000 claims description 4
- 101000884298 Homo sapiens CD226 antigen Proteins 0.000 claims description 4
- 101000914511 Homo sapiens CD27 antigen Proteins 0.000 claims description 4
- 101000892862 Homo sapiens Glutamate carboxypeptidase 2 Proteins 0.000 claims description 4
- 101001082627 Homo sapiens HLA class II histocompatibility antigen gamma chain Proteins 0.000 claims description 4
- 101001046677 Homo sapiens Integrin alpha-V Proteins 0.000 claims description 4
- 101000777628 Homo sapiens Leukocyte antigen CD37 Proteins 0.000 claims description 4
- 101000878605 Homo sapiens Low affinity immunoglobulin epsilon Fc receptor Proteins 0.000 claims description 4
- 101001133056 Homo sapiens Mucin-1 Proteins 0.000 claims description 4
- 101000934338 Homo sapiens Myeloid cell surface antigen CD33 Proteins 0.000 claims description 4
- 101000581981 Homo sapiens Neural cell adhesion molecule 1 Proteins 0.000 claims description 4
- 101001098352 Homo sapiens OX-2 membrane glycoprotein Proteins 0.000 claims description 4
- 101000934341 Homo sapiens T-cell surface glycoprotein CD5 Proteins 0.000 claims description 4
- 101000914514 Homo sapiens T-cell-specific surface glycoprotein CD28 Proteins 0.000 claims description 4
- 101000914484 Homo sapiens T-lymphocyte activation antigen CD80 Proteins 0.000 claims description 4
- 101000801433 Homo sapiens Trophoblast glycoprotein Proteins 0.000 claims description 4
- 101000610605 Homo sapiens Tumor necrosis factor receptor superfamily member 10A Proteins 0.000 claims description 4
- 101000851376 Homo sapiens Tumor necrosis factor receptor superfamily member 8 Proteins 0.000 claims description 4
- 241000701806 Human papillomavirus Species 0.000 claims description 4
- 108010073816 IgE Receptors Proteins 0.000 claims description 4
- 102000009438 IgE Receptors Human genes 0.000 claims description 4
- 102100022337 Integrin alpha-V Human genes 0.000 claims description 4
- 102000003816 Interleukin-13 Human genes 0.000 claims description 4
- 108090000176 Interleukin-13 Proteins 0.000 claims description 4
- 108010002350 Interleukin-2 Proteins 0.000 claims description 4
- 102000000588 Interleukin-2 Human genes 0.000 claims description 4
- 108090001005 Interleukin-6 Proteins 0.000 claims description 4
- 102000004889 Interleukin-6 Human genes 0.000 claims description 4
- 108010002586 Interleukin-7 Proteins 0.000 claims description 4
- 208000008839 Kidney Neoplasms Diseases 0.000 claims description 4
- 102100031586 Leukocyte antigen CD37 Human genes 0.000 claims description 4
- 102100038007 Low affinity immunoglobulin epsilon Fc receptor Human genes 0.000 claims description 4
- 206010058467 Lung neoplasm malignant Diseases 0.000 claims description 4
- 206010025323 Lymphomas Diseases 0.000 claims description 4
- 102000003735 Mesothelin Human genes 0.000 claims description 4
- 108090000015 Mesothelin Proteins 0.000 claims description 4
- 206010027406 Mesothelioma Diseases 0.000 claims description 4
- 206010027476 Metastases Diseases 0.000 claims description 4
- 102100034256 Mucin-1 Human genes 0.000 claims description 4
- 108010063954 Mucins Proteins 0.000 claims description 4
- 208000033776 Myeloid Acute Leukemia Diseases 0.000 claims description 4
- 102100025243 Myeloid cell surface antigen CD33 Human genes 0.000 claims description 4
- 102100027347 Neural cell adhesion molecule 1 Human genes 0.000 claims description 4
- 102100028762 Neuropilin-1 Human genes 0.000 claims description 4
- 108090000772 Neuropilin-1 Proteins 0.000 claims description 4
- 102100037589 OX-2 membrane glycoprotein Human genes 0.000 claims description 4
- 229940121678 PD-L2 antagonist Drugs 0.000 claims description 4
- 206010061902 Pancreatic neoplasm Diseases 0.000 claims description 4
- 102100035703 Prostatic acid phosphatase Human genes 0.000 claims description 4
- 206010038389 Renal cancer Diseases 0.000 claims description 4
- ZZAFFYPNLYCDEP-HNNXBMFYSA-N Rosmarinsaeure Natural products OC(=O)[C@H](Cc1cccc(O)c1O)OC(=O)C=Cc2ccc(O)c(O)c2 ZZAFFYPNLYCDEP-HNNXBMFYSA-N 0.000 claims description 4
- 102100027751 Semaphorin-3F Human genes 0.000 claims description 4
- 101710199445 Semaphorin-3F Proteins 0.000 claims description 4
- 241001632234 Senecavirus Species 0.000 claims description 4
- 241000837158 Senecavirus A Species 0.000 claims description 4
- 206010041067 Small cell lung cancer Diseases 0.000 claims description 4
- 208000005718 Stomach Neoplasms Diseases 0.000 claims description 4
- 108010002687 Survivin Proteins 0.000 claims description 4
- 102100025244 T-cell surface glycoprotein CD5 Human genes 0.000 claims description 4
- 102100027213 T-cell-specific surface glycoprotein CD28 Human genes 0.000 claims description 4
- 102100027222 T-lymphocyte activation antigen CD80 Human genes 0.000 claims description 4
- 229940123803 TIM3 antagonist Drugs 0.000 claims description 4
- 102000007000 Tenascin Human genes 0.000 claims description 4
- 108010008125 Tenascin Proteins 0.000 claims description 4
- 208000024770 Thyroid neoplasm Diseases 0.000 claims description 4
- 102000040945 Transcription factor Human genes 0.000 claims description 4
- 108091023040 Transcription factor Proteins 0.000 claims description 4
- 102100023935 Transmembrane glycoprotein NMB Human genes 0.000 claims description 4
- 101710170091 Transmembrane glycoprotein NMB Proteins 0.000 claims description 4
- 102100033579 Trophoblast glycoprotein Human genes 0.000 claims description 4
- 108060008683 Tumor Necrosis Factor Receptor Proteins 0.000 claims description 4
- 102100040113 Tumor necrosis factor receptor superfamily member 10A Human genes 0.000 claims description 4
- 101710178278 Tumor necrosis factor receptor superfamily member 10B Proteins 0.000 claims description 4
- 102100036857 Tumor necrosis factor receptor superfamily member 8 Human genes 0.000 claims description 4
- 229940124922 Twinrix Drugs 0.000 claims description 4
- 208000002495 Uterine Neoplasms Diseases 0.000 claims description 4
- 108091008605 VEGF receptors Proteins 0.000 claims description 4
- 108010053096 Vascular Endothelial Growth Factor Receptor-1 Proteins 0.000 claims description 4
- 102000009484 Vascular Endothelial Growth Factor Receptors Human genes 0.000 claims description 4
- 102100033178 Vascular endothelial growth factor receptor 1 Human genes 0.000 claims description 4
- 108010065472 Vimentin Proteins 0.000 claims description 4
- 108010026331 alpha-Fetoproteins Proteins 0.000 claims description 4
- MXKCYTKUIDTFLY-ZNNSSXPHSA-N alpha-L-Fucp-(1->2)-beta-D-Galp-(1->4)-[alpha-L-Fucp-(1->3)]-beta-D-GlcpNAc-(1->3)-D-Galp Chemical compound O[C@H]1[C@H](O)[C@H](O)[C@H](C)O[C@H]1O[C@H]1[C@H](O[C@H]2[C@@H]([C@@H](NC(C)=O)[C@H](O[C@H]3[C@H]([C@@H](CO)OC(O)[C@@H]3O)O)O[C@@H]2CO)O[C@H]2[C@H]([C@H](O)[C@H](O)[C@H](C)O2)O)O[C@H](CO)[C@H](O)[C@@H]1O MXKCYTKUIDTFLY-ZNNSSXPHSA-N 0.000 claims description 4
- 230000004075 alteration Effects 0.000 claims description 4
- 229960003852 atezolizumab Drugs 0.000 claims description 4
- 230000004900 autophagic degradation Effects 0.000 claims description 4
- 229950002916 avelumab Drugs 0.000 claims description 4
- 230000004071 biological effect Effects 0.000 claims description 4
- 230000010261 cell growth Effects 0.000 claims description 4
- 229950007409 dacetuzumab Drugs 0.000 claims description 4
- 230000008021 deposition Effects 0.000 claims description 4
- 238000011161 development Methods 0.000 claims description 4
- 230000018109 developmental process Effects 0.000 claims description 4
- 229950009791 durvalumab Drugs 0.000 claims description 4
- 239000012636 effector Substances 0.000 claims description 4
- 210000001163 endosome Anatomy 0.000 claims description 4
- 229950010640 ensituximab Drugs 0.000 claims description 4
- 229950006370 epacadostat Drugs 0.000 claims description 4
- 230000004761 fibrosis Effects 0.000 claims description 4
- 206010017758 gastric cancer Diseases 0.000 claims description 4
- 208000024908 graft versus host disease Diseases 0.000 claims description 4
- 201000010536 head and neck cancer Diseases 0.000 claims description 4
- 208000014829 head and neck neoplasm Diseases 0.000 claims description 4
- SPSXSWRZQFPVTJ-ZQQKUFEYSA-N hepatitis b vaccine Chemical compound C([C@H](NC(=O)[C@H]([C@@H](C)O)NC(=O)[C@H]([C@@H](C)O)NC(=O)[C@H](CO)NC(=O)[C@H](CC(N)=O)NC(=O)[C@H](CC=1C2=CC=CC=C2NC=1)NC(=O)[C@H](CCC(N)=O)NC(=O)[C@@H](N)CCSC)C(=O)N[C@@H](CC1N=CN=C1)C(=O)N[C@@H](CCC(N)=O)C(=O)N[C@@H]([C@@H](C)O)C(=O)N[C@@H](CC(C)C)C(=O)N[C@@H](CCC(N)=O)C(=O)N[C@@H](CC(O)=O)C(=O)N1[C@@H](CCC1)C(=O)N[C@@H](CCCNC(N)=N)C(=O)N[C@@H](C(C)C)C(=O)OC(=O)CNC(=O)CNC(=O)[C@H](C)NC(=O)[C@H]1N(CCC1)C(=O)[C@H](CC=1C=CC=CC=1)NC(=O)[C@H](CC=1C=CC(O)=CC=1)NC(=O)[C@H](CC(C)C)NC(=O)CNC(=O)[C@@H](N)CCCNC(N)=N)C1=CC=CC=C1 SPSXSWRZQFPVTJ-ZQQKUFEYSA-N 0.000 claims description 4
- 229940124736 hepatitis-B vaccine Drugs 0.000 claims description 4
- 231100000844 hepatocellular carcinoma Toxicity 0.000 claims description 4
- 238000005734 heterodimerization reaction Methods 0.000 claims description 4
- 238000000338 in vitro Methods 0.000 claims description 4
- 208000027866 inflammatory disease Diseases 0.000 claims description 4
- 108010074108 interleukin-21 Proteins 0.000 claims description 4
- 230000009545 invasion Effects 0.000 claims description 4
- 229960005386 ipilimumab Drugs 0.000 claims description 4
- 201000010982 kidney cancer Diseases 0.000 claims description 4
- 201000005202 lung cancer Diseases 0.000 claims description 4
- 208000020816 lung neoplasm Diseases 0.000 claims description 4
- 230000001926 lymphatic effect Effects 0.000 claims description 4
- 208000015486 malignant pancreatic neoplasm Diseases 0.000 claims description 4
- 230000009401 metastasis Effects 0.000 claims description 4
- 230000001394 metastastic effect Effects 0.000 claims description 4
- 206010061289 metastatic neoplasm Diseases 0.000 claims description 4
- 201000002528 pancreatic cancer Diseases 0.000 claims description 4
- 229950010773 pidilizumab Drugs 0.000 claims description 4
- 102000040430 polynucleotide Human genes 0.000 claims description 4
- 108091033319 polynucleotide Proteins 0.000 claims description 4
- 239000002157 polynucleotide Substances 0.000 claims description 4
- 108010043671 prostatic acid phosphatase Proteins 0.000 claims description 4
- 229940034080 provenge Drugs 0.000 claims description 4
- JFINOWIINSTUNY-UHFFFAOYSA-N pyrrolidin-3-ylmethanesulfonamide Chemical compound NS(=O)(=O)CC1CCNC1 JFINOWIINSTUNY-UHFFFAOYSA-N 0.000 claims description 4
- DOUMFZQKYFQNTF-MRXNPFEDSA-N rosemarinic acid Natural products C([C@H](C(=O)O)OC(=O)C=CC=1C=C(O)C(O)=CC=1)C1=CC=C(O)C(O)=C1 DOUMFZQKYFQNTF-MRXNPFEDSA-N 0.000 claims description 4
- TVHVQJFBWRLYOD-UHFFFAOYSA-N rosmarinic acid Natural products OC(=O)C(Cc1ccc(O)c(O)c1)OC(=Cc2ccc(O)c(O)c2)C=O TVHVQJFBWRLYOD-UHFFFAOYSA-N 0.000 claims description 4
- 229960000714 sipuleucel-t Drugs 0.000 claims description 4
- 208000000587 small cell lung carcinoma Diseases 0.000 claims description 4
- 210000002460 smooth muscle Anatomy 0.000 claims description 4
- 201000011549 stomach cancer Diseases 0.000 claims description 4
- 239000000758 substrate Substances 0.000 claims description 4
- 101150047061 tag-72 gene Proteins 0.000 claims description 4
- 201000002510 thyroid cancer Diseases 0.000 claims description 4
- 229950007217 tremelimumab Drugs 0.000 claims description 4
- 102000003298 tumor necrosis factor receptor Human genes 0.000 claims description 4
- 206010046766 uterine cancer Diseases 0.000 claims description 4
- 229950003520 utomilumab Drugs 0.000 claims description 4
- 229950001067 varlilumab Drugs 0.000 claims description 4
- 210000005048 vimentin Anatomy 0.000 claims description 4
- 108010069784 vitespin Proteins 0.000 claims description 4
- 102100038078 CD276 antigen Human genes 0.000 claims description 3
- 102100032912 CD44 antigen Human genes 0.000 claims description 3
- 101150029707 ERBB2 gene Proteins 0.000 claims description 3
- 102000006354 HLA-DR Antigens Human genes 0.000 claims description 3
- 108010058597 HLA-DR Antigens Proteins 0.000 claims description 3
- 102100022623 Hepatocyte growth factor receptor Human genes 0.000 claims description 3
- 101000884279 Homo sapiens CD276 antigen Proteins 0.000 claims description 3
- 101000868273 Homo sapiens CD44 antigen Proteins 0.000 claims description 3
- 241000282567 Macaca fascicularis Species 0.000 claims description 3
- 108010089836 Proto-Oncogene Proteins c-met Proteins 0.000 claims description 3
- 229940124942 Recombivax HB Drugs 0.000 claims description 3
- 108700033496 Recombivax HB Proteins 0.000 claims description 3
- 230000000259 anti-tumor effect Effects 0.000 claims description 3
- 210000003719 b-lymphocyte Anatomy 0.000 claims description 3
- 230000012292 cell migration Effects 0.000 claims description 3
- 230000001413 cellular effect Effects 0.000 claims description 3
- 230000001086 cytosolic effect Effects 0.000 claims description 3
- 230000035168 lymphangiogenesis Effects 0.000 claims description 3
- 230000001537 neural effect Effects 0.000 claims description 3
- 229960002566 papillomavirus vaccine Drugs 0.000 claims description 3
- 230000036961 partial effect Effects 0.000 claims description 3
- 230000037361 pathway Effects 0.000 claims description 3
- 210000003491 skin Anatomy 0.000 claims description 3
- 108091023037 Aptamer Proteins 0.000 claims description 2
- 208000032791 BCR-ABL1 positive chronic myelogenous leukemia Diseases 0.000 claims description 2
- 206010005949 Bone cancer Diseases 0.000 claims description 2
- 208000018084 Bone neoplasm Diseases 0.000 claims description 2
- 206010055113 Breast cancer metastatic Diseases 0.000 claims description 2
- 206010007953 Central nervous system lymphoma Diseases 0.000 claims description 2
- 206010008342 Cervix carcinoma Diseases 0.000 claims description 2
- 208000010833 Chronic myeloid leukaemia Diseases 0.000 claims description 2
- 206010059866 Drug resistance Diseases 0.000 claims description 2
- 208000000461 Esophageal Neoplasms Diseases 0.000 claims description 2
- 206010018691 Granuloma Diseases 0.000 claims description 2
- 102000009465 Growth Factor Receptors Human genes 0.000 claims description 2
- 108010009202 Growth Factor Receptors Proteins 0.000 claims description 2
- 208000017604 Hodgkin disease Diseases 0.000 claims description 2
- 208000021519 Hodgkin lymphoma Diseases 0.000 claims description 2
- 208000010747 Hodgkins lymphoma Diseases 0.000 claims description 2
- 101000934489 Homo sapiens Nucleosome-remodeling factor subunit BPTF Proteins 0.000 claims description 2
- 101000886818 Homo sapiens PDZ domain-containing protein GIPC1 Proteins 0.000 claims description 2
- 101000886822 Homo sapiens PDZ domain-containing protein GIPC2 Proteins 0.000 claims description 2
- 101000886826 Homo sapiens PDZ domain-containing protein GIPC3 Proteins 0.000 claims description 2
- 102100026120 IgG receptor FcRn large subunit p51 Human genes 0.000 claims description 2
- 101710177940 IgG receptor FcRn large subunit p51 Proteins 0.000 claims description 2
- 108010067060 Immunoglobulin Variable Region Proteins 0.000 claims description 2
- 102000017727 Immunoglobulin Variable Region Human genes 0.000 claims description 2
- 108010034143 Inflammasomes Proteins 0.000 claims description 2
- 206010061218 Inflammation Diseases 0.000 claims description 2
- 108010085895 Laminin Proteins 0.000 claims description 2
- 102000007547 Laminin Human genes 0.000 claims description 2
- 208000032420 Latent Infection Diseases 0.000 claims description 2
- 208000019693 Lung disease Diseases 0.000 claims description 2
- 206010025219 Lymphangioma Diseases 0.000 claims description 2
- 208000028018 Lymphocytic leukaemia Diseases 0.000 claims description 2
- 208000000172 Medulloblastoma Diseases 0.000 claims description 2
- 206010027480 Metastatic malignant melanoma Diseases 0.000 claims description 2
- 208000033761 Myelogenous Chronic BCR-ABL Positive Leukemia Diseases 0.000 claims description 2
- 208000015914 Non-Hodgkin lymphomas Diseases 0.000 claims description 2
- 102100025062 Nucleosome-remodeling factor subunit BPTF Human genes 0.000 claims description 2
- 206010030113 Oedema Diseases 0.000 claims description 2
- 206010030155 Oesophageal carcinoma Diseases 0.000 claims description 2
- 102100039983 PDZ domain-containing protein GIPC1 Human genes 0.000 claims description 2
- 102100039984 PDZ domain-containing protein GIPC2 Human genes 0.000 claims description 2
- 102100039982 PDZ domain-containing protein GIPC3 Human genes 0.000 claims description 2
- 206010057249 Phagocytosis Diseases 0.000 claims description 2
- 208000007913 Pituitary Neoplasms Diseases 0.000 claims description 2
- 201000005746 Pituitary adenoma Diseases 0.000 claims description 2
- 206010061538 Pituitary tumour benign Diseases 0.000 claims description 2
- 206010057846 Primitive neuroectodermal tumour Diseases 0.000 claims description 2
- 208000034541 Rare lymphatic malformation Diseases 0.000 claims description 2
- 206010039491 Sarcoma Diseases 0.000 claims description 2
- 102100027979 Semaphorin-3B Human genes 0.000 claims description 2
- 101710199438 Semaphorin-3B Proteins 0.000 claims description 2
- 102100027980 Semaphorin-3C Human genes 0.000 claims description 2
- 101710199433 Semaphorin-3C Proteins 0.000 claims description 2
- 102100027746 Semaphorin-3D Human genes 0.000 claims description 2
- 101710199434 Semaphorin-3D Proteins 0.000 claims description 2
- 102100027750 Semaphorin-3G Human genes 0.000 claims description 2
- 101710199439 Semaphorin-3G Proteins 0.000 claims description 2
- 208000033749 Small cell carcinoma of the bladder Diseases 0.000 claims description 2
- 208000004732 Systemic Vasculitis Diseases 0.000 claims description 2
- 208000024313 Testicular Neoplasms Diseases 0.000 claims description 2
- 206010057644 Testis cancer Diseases 0.000 claims description 2
- 102000004887 Transforming Growth Factor beta Human genes 0.000 claims description 2
- 108090001012 Transforming Growth Factor beta Proteins 0.000 claims description 2
- 208000006105 Uterine Cervical Neoplasms Diseases 0.000 claims description 2
- 206010047115 Vasculitis Diseases 0.000 claims description 2
- 208000014070 Vestibular schwannoma Diseases 0.000 claims description 2
- 238000010521 absorption reaction Methods 0.000 claims description 2
- 208000004064 acoustic neuroma Diseases 0.000 claims description 2
- 102000035181 adaptor proteins Human genes 0.000 claims description 2
- 108091005764 adaptor proteins Proteins 0.000 claims description 2
- 208000026935 allergic disease Diseases 0.000 claims description 2
- 230000000172 allergic effect Effects 0.000 claims description 2
- 230000025194 apoptotic cell clearance Effects 0.000 claims description 2
- 208000006673 asthma Diseases 0.000 claims description 2
- 208000010668 atopic eczema Diseases 0.000 claims description 2
- 230000005784 autoimmunity Effects 0.000 claims description 2
- 230000014461 bone development Effects 0.000 claims description 2
- 230000010072 bone remodeling Effects 0.000 claims description 2
- 230000021164 cell adhesion Effects 0.000 claims description 2
- 230000009087 cell motility Effects 0.000 claims description 2
- 201000010881 cervical cancer Diseases 0.000 claims description 2
- 230000008859 change Effects 0.000 claims description 2
- 230000001684 chronic effect Effects 0.000 claims description 2
- 230000006378 damage Effects 0.000 claims description 2
- 238000012217 deletion Methods 0.000 claims description 2
- 230000037430 deletion Effects 0.000 claims description 2
- 208000035475 disorder Diseases 0.000 claims description 2
- 230000003511 endothelial effect Effects 0.000 claims description 2
- 201000004101 esophageal cancer Diseases 0.000 claims description 2
- 208000021045 exocrine pancreatic carcinoma Diseases 0.000 claims description 2
- 230000003176 fibrotic effect Effects 0.000 claims description 2
- 230000002068 genetic effect Effects 0.000 claims description 2
- 208000002409 gliosarcoma Diseases 0.000 claims description 2
- 239000003102 growth factor Substances 0.000 claims description 2
- 239000001963 growth medium Substances 0.000 claims description 2
- 230000002489 hematologic effect Effects 0.000 claims description 2
- 210000002865 immune cell Anatomy 0.000 claims description 2
- 230000005931 immune cell recruitment Effects 0.000 claims description 2
- 230000006054 immunological memory Effects 0.000 claims description 2
- 230000003308 immunostimulating effect Effects 0.000 claims description 2
- 208000015181 infectious disease Diseases 0.000 claims description 2
- 230000004054 inflammatory process Effects 0.000 claims description 2
- 230000000977 initiatory effect Effects 0.000 claims description 2
- 229940102223 injectable solution Drugs 0.000 claims description 2
- 238000007918 intramuscular administration Methods 0.000 claims description 2
- 238000007912 intraperitoneal administration Methods 0.000 claims description 2
- 238000001990 intravenous administration Methods 0.000 claims description 2
- 208000032839 leukemia Diseases 0.000 claims description 2
- 208000003747 lymphoid leukemia Diseases 0.000 claims description 2
- 230000036210 malignancy Effects 0.000 claims description 2
- 230000035800 maturation Effects 0.000 claims description 2
- 206010027191 meningioma Diseases 0.000 claims description 2
- 208000021039 metastatic melanoma Diseases 0.000 claims description 2
- 230000001617 migratory effect Effects 0.000 claims description 2
- 230000004899 motility Effects 0.000 claims description 2
- 210000003205 muscle Anatomy 0.000 claims description 2
- 230000000414 obstructive effect Effects 0.000 claims description 2
- 230000020477 pH reduction Effects 0.000 claims description 2
- 230000037324 pain perception Effects 0.000 claims description 2
- 210000001428 peripheral nervous system Anatomy 0.000 claims description 2
- 230000008782 phagocytosis Effects 0.000 claims description 2
- 208000021310 pituitary gland adenoma Diseases 0.000 claims description 2
- 208000016800 primary central nervous system lymphoma Diseases 0.000 claims description 2
- 208000029340 primitive neuroectodermal tumor Diseases 0.000 claims description 2
- 208000009954 pyoderma gangrenosum Diseases 0.000 claims description 2
- 238000007634 remodeling Methods 0.000 claims description 2
- 206010039073 rheumatoid arthritis Diseases 0.000 claims description 2
- 201000000306 sarcoidosis Diseases 0.000 claims description 2
- 239000012679 serum free medium Substances 0.000 claims description 2
- 230000015590 smooth muscle cell migration Effects 0.000 claims description 2
- 229950007213 spartalizumab Drugs 0.000 claims description 2
- 238000007920 subcutaneous administration Methods 0.000 claims description 2
- 230000002459 sustained effect Effects 0.000 claims description 2
- 201000000596 systemic lupus erythematosus Diseases 0.000 claims description 2
- 201000003120 testicular cancer Diseases 0.000 claims description 2
- ZRKFYGHZFMAOKI-QMGMOQQFSA-N tgfbeta Chemical compound C([C@H](NC(=O)[C@H](C(C)C)NC(=O)CNC(=O)[C@H](CCC(O)=O)NC(=O)[C@H](CCCNC(N)=N)NC(=O)[C@H](CC(N)=O)NC(=O)[C@H](CC(C)C)NC(=O)[C@H]([C@@H](C)O)NC(=O)[C@H](CCC(O)=O)NC(=O)[C@H]([C@@H](C)O)NC(=O)[C@H](CC(C)C)NC(=O)CNC(=O)[C@H](C)NC(=O)[C@H](CO)NC(=O)[C@H](CCC(N)=O)NC(=O)[C@@H](NC(=O)[C@H](C)NC(=O)[C@H](C)NC(=O)[C@@H](NC(=O)[C@H](CC(C)C)NC(=O)[C@@H](N)CCSC)C(C)C)[C@@H](C)CC)C(=O)N[C@@H]([C@@H](C)O)C(=O)N[C@@H](C(C)C)C(=O)N[C@@H](CC=1C=CC=CC=1)C(=O)N[C@@H](C)C(=O)N1[C@@H](CCC1)C(=O)N[C@@H]([C@@H](C)O)C(=O)N[C@@H](CC(N)=O)C(=O)N[C@@H](CCC(O)=O)C(=O)N[C@@H](C)C(=O)N[C@@H](CC=1C=CC=CC=1)C(=O)N[C@@H](CCCNC(N)=N)C(=O)N[C@@H](C)C(=O)N[C@@H](CC(C)C)C(=O)N1[C@@H](CCC1)C(=O)N1[C@@H](CCC1)C(=O)N[C@@H](CCCNC(N)=N)C(=O)N[C@@H](CCC(O)=O)C(=O)N[C@@H](CCCNC(N)=N)C(=O)N[C@@H](CO)C(=O)N[C@@H](CCCNC(N)=N)C(=O)N[C@@H](CC(C)C)C(=O)N[C@@H](CC(C)C)C(O)=O)C1=CC=C(O)C=C1 ZRKFYGHZFMAOKI-QMGMOQQFSA-N 0.000 claims description 2
- 230000007704 transition Effects 0.000 claims description 2
- 206010044412 transitional cell carcinoma Diseases 0.000 claims description 2
- 201000007710 urinary bladder small cell neuroendocrine carcinoma Diseases 0.000 claims description 2
- 210000001215 vagina Anatomy 0.000 claims description 2
- 230000008728 vascular permeability Effects 0.000 claims description 2
- 210000004509 vascular smooth muscle cell Anatomy 0.000 claims description 2
- 230000029663 wound healing Effects 0.000 claims description 2
- 102000005789 Vascular Endothelial Growth Factors Human genes 0.000 claims 6
- 102000009524 Vascular Endothelial Growth Factor A Human genes 0.000 claims 5
- FDKXTQMXEQVLRF-ZHACJKMWSA-N (E)-dacarbazine Chemical compound CN(C)\N=N\c1[nH]cnc1C(N)=O FDKXTQMXEQVLRF-ZHACJKMWSA-N 0.000 claims 3
- VHRSUDSXCMQTMA-PJHHCJLFSA-N 6alpha-methylprednisolone Chemical compound C([C@@]12C)=CC(=O)C=C1[C@@H](C)C[C@@H]1[C@@H]2[C@@H](O)C[C@]2(C)[C@@](O)(C(=O)CO)CC[C@H]21 VHRSUDSXCMQTMA-PJHHCJLFSA-N 0.000 claims 3
- 190000008236 carboplatin Chemical compound 0.000 claims 3
- MNRILEROXIRVNJ-UHFFFAOYSA-N tioguanine Chemical compound N1C(N)=NC(=S)C2=NC=N[C]21 MNRILEROXIRVNJ-UHFFFAOYSA-N 0.000 claims 3
- GBABOYUKABKIAF-GHYRFKGUSA-N vinorelbine Chemical compound C1N(CC=2C3=CC=CC=C3NC=22)CC(CC)=C[C@H]1C[C@]2(C(=O)OC)C1=CC([C@]23[C@H]([C@]([C@H](OC(C)=O)[C@]4(CC)C=CCN([C@H]34)CC2)(O)C(=O)OC)N2C)=C2C=C1OC GBABOYUKABKIAF-GHYRFKGUSA-N 0.000 claims 3
- 102100025570 Cancer/testis antigen 1 Human genes 0.000 claims 2
- 101000856237 Homo sapiens Cancer/testis antigen 1 Proteins 0.000 claims 2
- 108010065805 Interleukin-12 Proteins 0.000 claims 2
- CZCIKBSVHDNIDH-UHFFFAOYSA-N Nalpha-methyl-DL-tryptophan Natural products C1=CC=C2C(CC(NC)C(O)=O)=CNC2=C1 CZCIKBSVHDNIDH-UHFFFAOYSA-N 0.000 claims 2
- 102100032101 Tumor necrosis factor ligand superfamily member 9 Human genes 0.000 claims 2
- 102000013127 Vimentin Human genes 0.000 claims 2
- 102000013529 alpha-Fetoproteins Human genes 0.000 claims 2
- 101100112922 Candida albicans CDR3 gene Proteins 0.000 claims 1
- 241000711475 Feline infectious peritonitis virus Species 0.000 claims 1
- 102000014160 PTEN Phosphohydrolase Human genes 0.000 claims 1
- 108010011536 PTEN Phosphohydrolase Proteins 0.000 claims 1
- 210000000440 neutrophil Anatomy 0.000 claims 1
- 229940114241 recombivax Drugs 0.000 claims 1
- 229960005486 vaccine Drugs 0.000 claims 1
- 230000007783 downstream signaling Effects 0.000 abstract description 2
- 229940024606 amino acid Drugs 0.000 description 24
- 235000001014 amino acid Nutrition 0.000 description 22
- 102100039037 Vascular endothelial growth factor A Human genes 0.000 description 17
- 239000000126 substance Substances 0.000 description 9
- 238000007792 addition Methods 0.000 description 7
- 238000010494 dissociation reaction Methods 0.000 description 7
- 230000005593 dissociations Effects 0.000 description 7
- 241000699666 Mus <mouse, genus> Species 0.000 description 6
- 208000003721 Triple Negative Breast Neoplasms Diseases 0.000 description 6
- 238000003556 assay Methods 0.000 description 6
- 229960004316 cisplatin Drugs 0.000 description 6
- 208000022679 triple-negative breast carcinoma Diseases 0.000 description 6
- 231100000491 EC50 Toxicity 0.000 description 5
- 241001465754 Metazoa Species 0.000 description 4
- DQLATGHUWYMOKM-UHFFFAOYSA-L cisplatin Chemical compound N[Pt](N)(Cl)Cl DQLATGHUWYMOKM-UHFFFAOYSA-L 0.000 description 4
- 238000010293 colony formation assay Methods 0.000 description 4
- 230000000875 corresponding effect Effects 0.000 description 4
- 235000018102 proteins Nutrition 0.000 description 4
- 230000009870 specific binding Effects 0.000 description 4
- OMJKFYKNWZZKTK-POHAHGRESA-N (5z)-5-(dimethylaminohydrazinylidene)imidazole-4-carboxamide Chemical compound CN(C)N\N=C1/N=CN=C1C(N)=O OMJKFYKNWZZKTK-POHAHGRESA-N 0.000 description 3
- 102100031004 Histidine-tRNA ligase, cytoplasmic Human genes 0.000 description 3
- FQISKWAFAHGMGT-SGJOWKDISA-M Methylprednisolone sodium succinate Chemical compound [Na+].C([C@@]12C)=CC(=O)C=C1[C@@H](C)C[C@@H]1[C@@H]2[C@@H](O)C[C@]2(C)[C@@](O)(C(=O)COC(=O)CCC([O-])=O)CC[C@H]21 FQISKWAFAHGMGT-SGJOWKDISA-M 0.000 description 3
- VSRXQHXAPYXROS-UHFFFAOYSA-N azanide;cyclobutane-1,1-dicarboxylic acid;platinum(2+) Chemical compound [NH2-].[NH2-].[Pt+2].OC(=O)C1(C(O)=O)CCC1 VSRXQHXAPYXROS-UHFFFAOYSA-N 0.000 description 3
- 230000001900 immune effect Effects 0.000 description 3
- 230000005764 inhibitory process Effects 0.000 description 3
- 230000003834 intracellular effect Effects 0.000 description 3
- GBABOYUKABKIAF-IELIFDKJSA-N vinorelbine Chemical compound C1N(CC=2C3=CC=CC=C3NC=22)CC(CC)=C[C@H]1C[C@]2(C(=O)OC)C1=CC([C@]23[C@H]([C@@]([C@H](OC(C)=O)[C@]4(CC)C=CCN([C@H]34)CC2)(O)C(=O)OC)N2C)=C2C=C1OC GBABOYUKABKIAF-IELIFDKJSA-N 0.000 description 3
- 102000002627 4-1BB Ligand Human genes 0.000 description 2
- 102100023635 Alpha-fetoprotein Human genes 0.000 description 2
- 102000052866 Amino Acyl-tRNA Synthetases Human genes 0.000 description 2
- 108700028939 Amino Acyl-tRNA Synthetases Proteins 0.000 description 2
- 238000012413 Fluorescence activated cell sorting analysis Methods 0.000 description 2
- 101000654674 Homo sapiens Semaphorin-6A Proteins 0.000 description 2
- 102000015728 Mucins Human genes 0.000 description 2
- 102100032795 Semaphorin-6A Human genes 0.000 description 2
- 238000000692 Student's t-test Methods 0.000 description 2
- 102100035071 Vimentin Human genes 0.000 description 2
- 230000009471 action Effects 0.000 description 2
- 229910052799 carbon Inorganic materials 0.000 description 2
- 239000013043 chemical agent Substances 0.000 description 2
- 238000002512 chemotherapy Methods 0.000 description 2
- 229940044683 chemotherapy drug Drugs 0.000 description 2
- 230000007423 decrease Effects 0.000 description 2
- 229940079593 drug Drugs 0.000 description 2
- 239000000463 material Substances 0.000 description 2
- 238000010561 standard procedure Methods 0.000 description 2
- 230000014616 translation Effects 0.000 description 2
- 230000004614 tumor growth Effects 0.000 description 2
- VEVRNHHLCPGNDU-MUGJNUQGSA-N (2s)-2-amino-5-[1-[(5s)-5-amino-5-carboxypentyl]-3,5-bis[(3s)-3-amino-3-carboxypropyl]pyridin-1-ium-4-yl]pentanoate Chemical compound OC(=O)[C@@H](N)CCCC[N+]1=CC(CC[C@H](N)C(O)=O)=C(CCC[C@H](N)C([O-])=O)C(CC[C@H](N)C(O)=O)=C1 VEVRNHHLCPGNDU-MUGJNUQGSA-N 0.000 description 1
- XWHHYOYVRVGJJY-UHFFFAOYSA-N 4-fluorophenylalanine Chemical compound OC(=O)C(N)CC1=CC=C(F)C=C1 XWHHYOYVRVGJJY-UHFFFAOYSA-N 0.000 description 1
- 229920001817 Agar Polymers 0.000 description 1
- 239000004475 Arginine Substances 0.000 description 1
- 241000894006 Bacteria Species 0.000 description 1
- OKTJSMMVPCPJKN-UHFFFAOYSA-N Carbon Chemical compound [C] OKTJSMMVPCPJKN-UHFFFAOYSA-N 0.000 description 1
- 102000014914 Carrier Proteins Human genes 0.000 description 1
- 241000282693 Cercopithecidae Species 0.000 description 1
- 108010047041 Complementarity Determining Regions Proteins 0.000 description 1
- 208000028006 Corneal injury Diseases 0.000 description 1
- 206010011968 Decreased immune responsiveness Diseases 0.000 description 1
- 101001067189 Homo sapiens Plexin-A1 Proteins 0.000 description 1
- LCWXJXMHJVIJFK-UHFFFAOYSA-N Hydroxylysine Natural products NCC(O)CC(N)CC(O)=O LCWXJXMHJVIJFK-UHFFFAOYSA-N 0.000 description 1
- PMMYEEVYMWASQN-DMTCNVIQSA-N Hydroxyproline Chemical compound O[C@H]1CN[C@H](C(O)=O)C1 PMMYEEVYMWASQN-DMTCNVIQSA-N 0.000 description 1
- SNDPXSYFESPGGJ-BYPYZUCNSA-N L-2-aminopentanoic acid Chemical compound CCC[C@H](N)C(O)=O SNDPXSYFESPGGJ-BYPYZUCNSA-N 0.000 description 1
- AHLPHDHHMVZTML-BYPYZUCNSA-N L-Ornithine Chemical compound NCCC[C@H](N)C(O)=O AHLPHDHHMVZTML-BYPYZUCNSA-N 0.000 description 1
- RHGKLRLOHDJJDR-BYPYZUCNSA-N L-citrulline Chemical compound NC(=O)NCCC[C@H]([NH3+])C([O-])=O RHGKLRLOHDJJDR-BYPYZUCNSA-N 0.000 description 1
- GGLZPLKKBSSKCX-YFKPBYRVSA-N L-ethionine Chemical compound CCSCC[C@H](N)C(O)=O GGLZPLKKBSSKCX-YFKPBYRVSA-N 0.000 description 1
- FFFHZYDWPBMWHY-VKHMYHEASA-N L-homocysteine Chemical compound OC(=O)[C@@H](N)CCS FFFHZYDWPBMWHY-VKHMYHEASA-N 0.000 description 1
- SNDPXSYFESPGGJ-UHFFFAOYSA-N L-norVal-OH Natural products CCCC(N)C(O)=O SNDPXSYFESPGGJ-UHFFFAOYSA-N 0.000 description 1
- LRQKBLKVPFOOQJ-YFKPBYRVSA-N L-norleucine Chemical compound CCCC[C@H]([NH3+])C([O-])=O LRQKBLKVPFOOQJ-YFKPBYRVSA-N 0.000 description 1
- 206010027458 Metastases to lung Diseases 0.000 description 1
- 101600105505 Mus musculus Vascular endothelial growth factor C (isoform 1) Proteins 0.000 description 1
- RHGKLRLOHDJJDR-UHFFFAOYSA-N Ndelta-carbamoyl-DL-ornithine Natural products OC(=O)C(N)CCCNC(N)=O RHGKLRLOHDJJDR-UHFFFAOYSA-N 0.000 description 1
- AHLPHDHHMVZTML-UHFFFAOYSA-N Orn-delta-NH2 Natural products NCCCC(N)C(O)=O AHLPHDHHMVZTML-UHFFFAOYSA-N 0.000 description 1
- UTJLXEIPEHZYQJ-UHFFFAOYSA-N Ornithine Natural products OC(=O)C(C)CCCN UTJLXEIPEHZYQJ-UHFFFAOYSA-N 0.000 description 1
- 102000038030 PI3Ks Human genes 0.000 description 1
- 108091007960 PI3Ks Proteins 0.000 description 1
- 102100032543 Phosphatidylinositol 3,4,5-trisphosphate 3-phosphatase and dual-specificity protein phosphatase PTEN Human genes 0.000 description 1
- 101710132081 Phosphatidylinositol 3,4,5-trisphosphate 3-phosphatase and dual-specificity protein phosphatase PTEN Proteins 0.000 description 1
- 102100034382 Plexin-A1 Human genes 0.000 description 1
- 108020004511 Recombinant DNA Proteins 0.000 description 1
- 238000005411 Van der Waals force Methods 0.000 description 1
- 239000008272 agar Substances 0.000 description 1
- 125000003275 alpha amino acid group Chemical group 0.000 description 1
- 238000004458 analytical method Methods 0.000 description 1
- 238000010171 animal model Methods 0.000 description 1
- 230000002001 anti-metastasis Effects 0.000 description 1
- 229940125644 antibody drug Drugs 0.000 description 1
- 230000000890 antigenic effect Effects 0.000 description 1
- 230000006907 apoptotic process Effects 0.000 description 1
- ODKSFYDXXFIFQN-UHFFFAOYSA-N arginine Natural products OC(=O)C(N)CCCNC(N)=N ODKSFYDXXFIFQN-UHFFFAOYSA-N 0.000 description 1
- 230000003376 axonal effect Effects 0.000 description 1
- 230000008901 benefit Effects 0.000 description 1
- 239000011230 binding agent Substances 0.000 description 1
- 108091008324 binding proteins Proteins 0.000 description 1
- 230000033228 biological regulation Effects 0.000 description 1
- 238000004364 calculation method Methods 0.000 description 1
- 231100000504 carcinogenesis Toxicity 0.000 description 1
- 230000024245 cell differentiation Effects 0.000 description 1
- 230000003915 cell function Effects 0.000 description 1
- 230000033077 cellular process Effects 0.000 description 1
- 230000036755 cellular response Effects 0.000 description 1
- 230000004637 cellular stress Effects 0.000 description 1
- 125000003636 chemical group Chemical group 0.000 description 1
- 239000003153 chemical reaction reagent Substances 0.000 description 1
- 229960002173 citrulline Drugs 0.000 description 1
- 235000013477 citrulline Nutrition 0.000 description 1
- 230000009918 complex formation Effects 0.000 description 1
- 238000007796 conventional method Methods 0.000 description 1
- 210000004087 cornea Anatomy 0.000 description 1
- YSMODUONRAFBET-UHFFFAOYSA-N delta-DL-hydroxylysine Natural products NCC(O)CCC(N)C(O)=O YSMODUONRAFBET-UHFFFAOYSA-N 0.000 description 1
- 230000003831 deregulation Effects 0.000 description 1
- 238000001212 derivatisation Methods 0.000 description 1
- 238000010586 diagram Methods 0.000 description 1
- 238000010790 dilution Methods 0.000 description 1
- 239000012895 dilution Substances 0.000 description 1
- PMMYEEVYMWASQN-UHFFFAOYSA-N dl-hydroxyproline Natural products OC1C[NH2+]C(C([O-])=O)C1 PMMYEEVYMWASQN-UHFFFAOYSA-N 0.000 description 1
- 238000004520 electroporation Methods 0.000 description 1
- 230000012202 endocytosis Effects 0.000 description 1
- 238000005516 engineering process Methods 0.000 description 1
- 238000006911 enzymatic reaction Methods 0.000 description 1
- YSMODUONRAFBET-UHNVWZDZSA-N erythro-5-hydroxy-L-lysine Chemical compound NC[C@H](O)CC[C@H](N)C(O)=O YSMODUONRAFBET-UHNVWZDZSA-N 0.000 description 1
- 235000019197 fats Nutrition 0.000 description 1
- 238000009472 formulation Methods 0.000 description 1
- 102000037865 fusion proteins Human genes 0.000 description 1
- 108020001507 fusion proteins Proteins 0.000 description 1
- 230000013632 homeostatic process Effects 0.000 description 1
- 230000028996 humoral immune response Effects 0.000 description 1
- 239000001257 hydrogen Substances 0.000 description 1
- 229910052739 hydrogen Inorganic materials 0.000 description 1
- 230000002209 hydrophobic effect Effects 0.000 description 1
- QJHBJHUKURJDLG-UHFFFAOYSA-N hydroxy-L-lysine Natural products NCCCCC(NO)C(O)=O QJHBJHUKURJDLG-UHFFFAOYSA-N 0.000 description 1
- 229960002591 hydroxyproline Drugs 0.000 description 1
- 230000002163 immunogen Effects 0.000 description 1
- 230000002779 inactivation Effects 0.000 description 1
- 230000001939 inductive effect Effects 0.000 description 1
- 238000011081 inoculation Methods 0.000 description 1
- RGXCTRIQQODGIZ-UHFFFAOYSA-O isodesmosine Chemical compound OC(=O)C(N)CCCC[N+]1=CC(CCC(N)C(O)=O)=CC(CCC(N)C(O)=O)=C1CCCC(N)C(O)=O RGXCTRIQQODGIZ-UHFFFAOYSA-O 0.000 description 1
- 230000021633 leukocyte mediated immunity Effects 0.000 description 1
- 108020001756 ligand binding domains Proteins 0.000 description 1
- 238000004246 ligand exchange chromatography Methods 0.000 description 1
- 238000001638 lipofection Methods 0.000 description 1
- 238000004020 luminiscence type Methods 0.000 description 1
- 210000005073 lymphatic endothelial cell Anatomy 0.000 description 1
- 210000001365 lymphatic vessel Anatomy 0.000 description 1
- 210000004698 lymphocyte Anatomy 0.000 description 1
- 239000003550 marker Substances 0.000 description 1
- 238000005259 measurement Methods 0.000 description 1
- 230000007246 mechanism Effects 0.000 description 1
- 210000004379 membrane Anatomy 0.000 description 1
- 239000012528 membrane Substances 0.000 description 1
- 229920000609 methyl cellulose Polymers 0.000 description 1
- 239000001923 methylcellulose Substances 0.000 description 1
- 230000002906 microbiologic effect Effects 0.000 description 1
- 230000004048 modification Effects 0.000 description 1
- 238000012986 modification Methods 0.000 description 1
- 230000003387 muscular Effects 0.000 description 1
- 210000004897 n-terminal region Anatomy 0.000 description 1
- 238000002515 oligonucleotide synthesis Methods 0.000 description 1
- 230000008520 organization Effects 0.000 description 1
- 229960003104 ornithine Drugs 0.000 description 1
- 239000004031 partial agonist Substances 0.000 description 1
- 239000008194 pharmaceutical composition Substances 0.000 description 1
- 239000000825 pharmaceutical preparation Substances 0.000 description 1
- 230000026731 phosphorylation Effects 0.000 description 1
- 238000006366 phosphorylation reaction Methods 0.000 description 1
- 229920001282 polysaccharide Polymers 0.000 description 1
- 239000005017 polysaccharide Substances 0.000 description 1
- 150000004804 polysaccharides Chemical class 0.000 description 1
- 239000013641 positive control Substances 0.000 description 1
- 238000012809 post-inoculation Methods 0.000 description 1
- 230000008569 process Effects 0.000 description 1
- 239000000047 product Substances 0.000 description 1
- 230000035755 proliferation Effects 0.000 description 1
- 238000001243 protein synthesis Methods 0.000 description 1
- 238000000746 purification Methods 0.000 description 1
- 238000010188 recombinant method Methods 0.000 description 1
- 230000002829 reductive effect Effects 0.000 description 1
- 238000011160 research Methods 0.000 description 1
- 230000000717 retained effect Effects 0.000 description 1
- 230000002441 reversible effect Effects 0.000 description 1
- 230000035945 sensitivity Effects 0.000 description 1
- 230000011664 signaling Effects 0.000 description 1
- 241000894007 species Species 0.000 description 1
- 238000001228 spectrum Methods 0.000 description 1
- 230000002269 spontaneous effect Effects 0.000 description 1
- 238000010186 staining Methods 0.000 description 1
- 230000000638 stimulation Effects 0.000 description 1
- 238000006467 substitution reaction Methods 0.000 description 1
- 230000004083 survival effect Effects 0.000 description 1
- 230000002195 synergetic effect Effects 0.000 description 1
- 230000008685 targeting Effects 0.000 description 1
- 238000012360 testing method Methods 0.000 description 1
- 230000030968 tissue homeostasis Effects 0.000 description 1
- 239000003053 toxin Substances 0.000 description 1
- 231100000765 toxin Toxicity 0.000 description 1
- 108700012359 toxins Proteins 0.000 description 1
- 230000009466 transformation Effects 0.000 description 1
- 238000012384 transportation and delivery Methods 0.000 description 1
- 238000011269 treatment regimen Methods 0.000 description 1
- 230000001875 tumorinhibitory effect Effects 0.000 description 1
- 230000002792 vascular Effects 0.000 description 1
Classifications
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K16/00—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies
- C07K16/18—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans
- C07K16/28—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans against receptors, cell surface antigens or cell surface determinants
- C07K16/2863—Immunoglobulins [IGs], e.g. monoclonal or polyclonal antibodies against material from animals or humans against receptors, cell surface antigens or cell surface determinants against receptors for growth factors, growth regulators
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
- A61K39/395—Antibodies; Immunoglobulins; Immune serum, e.g. antilymphocytic serum
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
- A61K39/395—Antibodies; Immunoglobulins; Immune serum, e.g. antilymphocytic serum
- A61K39/39533—Antibodies; Immunoglobulins; Immune serum, e.g. antilymphocytic serum against materials from animals
- A61K39/3955—Antibodies; Immunoglobulins; Immune serum, e.g. antilymphocytic serum against materials from animals against proteinaceous materials, e.g. enzymes, hormones, lymphokines
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K45/00—Medicinal preparations containing active ingredients not provided for in groups A61K31/00 - A61K41/00
- A61K45/06—Mixtures of active ingredients without chemical characterisation, e.g. antiphlogistics and cardiaca
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P35/00—Antineoplastic agents
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P35/00—Antineoplastic agents
- A61P35/04—Antineoplastic agents specific for metastasis
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
- A61K2039/505—Medicinal preparations containing antigens or antibodies comprising antibodies
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K39/00—Medicinal preparations containing antigens or antibodies
- A61K39/0005—Vertebrate antigens
- A61K39/0011—Cancer antigens
- A61K39/001102—Receptors, cell surface antigens or cell surface determinants
- A61K39/001103—Receptors for growth factors
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K2317/00—Immunoglobulins specific features
- C07K2317/20—Immunoglobulins specific features characterized by taxonomic origin
- C07K2317/24—Immunoglobulins specific features characterized by taxonomic origin containing regions, domains or residues from different species, e.g. chimeric, humanized or veneered
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K2317/00—Immunoglobulins specific features
- C07K2317/30—Immunoglobulins specific features characterized by aspects of specificity or valency
- C07K2317/33—Crossreactivity, e.g. for species or epitope, or lack of said crossreactivity
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K2317/00—Immunoglobulins specific features
- C07K2317/30—Immunoglobulins specific features characterized by aspects of specificity or valency
- C07K2317/34—Identification of a linear epitope shorter than 20 amino acid residues or of a conformational epitope defined by amino acid residues
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K2317/00—Immunoglobulins specific features
- C07K2317/50—Immunoglobulins specific features characterized by immunoglobulin fragments
- C07K2317/52—Constant or Fc region; Isotype
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K2317/00—Immunoglobulins specific features
- C07K2317/70—Immunoglobulins specific features characterized by effect upon binding to a cell or to an antigen
- C07K2317/76—Antagonist effect on antigen, e.g. neutralization or inhibition of binding
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07K—PEPTIDES
- C07K2317/00—Immunoglobulins specific features
- C07K2317/90—Immunoglobulins specific features characterized by (pharmaco)kinetic aspects or by stability of the immunoglobulin
- C07K2317/92—Affinity (KD), association rate (Ka), dissociation rate (Kd) or EC50 value
Definitions
- Embodiments of the present disclosure relate to affinity matured and humanized antibodies and antigen-binding fragments thereof that specifically bind to human neuropilin-2 (NRP2) polypeptides, including those that modulate binding interactions between human NRP2 and at least one NRP2 ligand, and which thereby modulate subsequent NRP2-mediated downstream signaling events, including related therapeutic compositions and methods for modulating NRP2 activity and treating diseases such as NRP2-associated diseases.
- NRP2 neuropilin-2
- tRNA synthetases play important roles in cellular responses beyond their well-characterized role in protein synthesis.
- tRNA synthetases participate in a range of previously-unrecognized roles in responding to cellular stress and tissue homeostasis, in both intracellular and extracellular environments.
- this new pathway of regulation represents a previously unknown mechanism, which acts as a central regulator of cellular processes, including, for example, axonal guidance, endocytosis, cell migration, proliferation, survival, apoptosis, lymphangiogenesis, cellular differentiation, and cell attachment with direct relevance to cancer initiation, growth, metastasis, and chemoresistance, as wells as muscular, vascular, neuronal, bone, and immune homeostasis.
- the deregulation of any of these processes may lead to a spectrum of diseases, which may be addressed by the development of anti-NRP2 antibodies that selectively target the neuropilin- 2 axis.
- the present disclosure provides such antibodies and related embodiments.
- Embodiments of the present disclosure include antibodies or antigen-binding fragments thereof that specifically bind to a human neuropilin-2 (NRP2) polypeptide (anti-NRP2 antibody).
- NPP2 human neuropilin-2
- Certain embodiments include a therapeutic composition, comprising at least one antibody or antigen-binding fragment thereof that specifically binds to a human neuropilin-2 (NRP2) polypeptide (anti-NRP2 antibody), wherein the at least one antibody or antigen-binding fragment thereof comprises: a heavy chain variable region (V H ) sequence that comprises complementary determining region V H CDR1, V H CDR2, and V H CDR3 sequences selected from Table A1 or Table A3 and variants thereof which specifically bind to the human NRP2 polypeptide; and a light chain variable region (V L ) sequence that comprises complementary determining region V L CDRI, V CDR2, and V L CDR3 sequences selected from Table A1 or Table A3 and variants thereof which specifically bind to the human NRP2 polypeptide.
- V H heavy chain variable region
- V L light chain variable region
- the V H CDRI, V H CDR2, and V H CDR3 sequences comprise SEQ ID NOs: 1-3, respectively, and the V L CDRI, V L CDR2, and V L CDR3 sequences comprise SEQ ID NOs: 4-6, respectively, including variants thereof;
- the V H CDRI, V H CDR2, and V H CDR3 sequences comprise SEQ ID NOs: 7-9, respectively, and the V L CDRI, V L CDR2, and V L CDR3 sequences comprise SEQ ID NOs: 10-12, respectively, including variants thereof;
- the V H CDRI, V H CDR2, and V H CDR3 sequences comprise SEQ ID NOs: 13-15, respectively, and the V L CDRI, V L CDR2, and V L CDR3 sequences comprise SEQ ID NOs: 16-18, respectively, including variants thereof;
- the V H CDRI, V H CDR2, and V H CDR3 sequences comprise SEQ ID NOs: 19-21, respectively, and the V L CDRI, V L CDR2, and
- the VH sequence is at least 80, 85, 90, 95, 97, 98, 99, or 100% identical to a sequence selected from Table A2, optionally wherein the VH sequence has 1, 2, 3, 4, or 5 alterations in the framework regions.
- the VL sequence is at least 80, 85, 90, 95, 97, 98, 99, or 100% identical to a sequence selected from Table A2, optionally wherein the VL sequence has 1, 2, 3, 4, or 5 alterations in the framework regions.
- the VH sequence comprises a sequence at least 80, 85, 90, 95, 97, 98, 99, or 100% identical to SEQ ID NO: 43
- the VL sequence comprises a sequence at least 80, 85, 90, 95, 97, 98, 99, or 100% identical to SEQ ID NO: 44
- the VH sequence comprises a sequence at least 80, 85, 90, 95, 97, 98, 99, or 100% identical to SEQ ID NO: 45
- the V L sequence comprises a sequence at least 80, 85, 90, 95, 97, 98, 99, or 100% identical to SEQ ID NO: 46
- the V H sequence comprises a sequence at least 80, 85, 90, 95, 97, 98, 99, or 100% identical to SEQ ID NO: 47
- the VL sequence comprises a sequence at least 80, 85, 90, 95, 97, 98, 99, or 100% identical to SEQ ID NO: 48
- the VH sequence comprises a sequence at least 80, 85, 90, 95, 97, 98, 99,
- the at least one antibody or antigen-binding fragment thereof specifically binds to a full-length human NRP2 polypeptide or a human NRP2 polypeptide selected from Table Nl, optionally with an affinity of about 10 pM to about 500 pM or to about 50 nM, or about, at least about, or no more than about 10, 20, 30, 40, 50, 60, 70, 80, 90, 100, 110, 120, 130, 140, 150, 160, 170, 180, 190, 200, 300, 400, 500, 600, 700, 800, 900 pM, 1 nM, 10 nM, 25 nM, or 50 nM, or optionally with an affinity that ranges from about 10 pM to about 500 pM, about 10 pM to about 400 pM, about 10 pM to about 300 pM, about 10 pM to about 200 pM, about 10 pM to about 100 pM, about 10 pM to about 50 pM, or about 20 pM to
- the at least one antibody or antigen-binding fragment thereof that specifically binds to at least one epitope in a neuropilin domain selected from one or more of the neuropilin bl domain, neuropilin al domain, neuropilin a2 domain, neuropilin b2 domain, neuropilin c domain, neuropilin al/a2 combined domain, neuropilin bl/b2 combined domain, neuropilin a2/bl combined domain, neuropilin b2/c combined domain, neuropilin a2/bl/b2 combined domain, neuropilin a2/bl/b2/c combined domain, neuropilin al/a2/bl combined domain, neuropilin al/a2/bl/b2 combined domain, neuropilin al/a2/bl/b2 combined domain, neuropilin al/a2/bl/b2/c combined domain, and the neuropilin bl/b2/c combined domain, optionally with an affinity of about 10 pM to about 500 p
- the at least one antibody or antigen-binding fragment thereof specifically binds to at least one epitope in the neuropilin al domain, the neuropilin a2 domain, and/or the neuropilin ala2 combined domain, including adjacent linker regions, optionally at about residues;
- NRP2 precursor sequence 20-148, 30-141, 40-141, 50-141, 60-141, 70-141, 80-141, 90-141, 100-141, 110-141, 120-141, 130-141; 20-130, 20-120, 20-110, 20-100, 20-90, 20-80, 20-70, 20-60, 20-50, 20-40, or 20-30 as defined by a human NRP2 precursor sequence (see Table Nl);
- the at least one antibody or antigen-binding fragment thereof specifically binds to at least one epitope in the neuropilin bl domain, the neuropilin b2 domain, and/or the neuropilin bl/b2 combined domain, including adjacent linker regions, optionally at about residues;
- the at least one antibody or antigen-binding fragment thereof specifically binds to at least one epitope in the neuropilin a2/bl combined domain and/or the neuropilin b2c combined domain, including adjacent linker regions, optionally at about residues; (neuropilin a2bl combined domain) 149-437, 159-426, 169-426, 179-426, 189-426, 199-426, 209-426, 219-426, 229-426,239-426, 249-426, 259-426, 269-426, 279-426, 289-426, 299-426, 309- 426, 319-426, 329-426, 339-426, 349-426, 359-426, 369-426, 379-426, 389-426, 399-426, 409-426, 419-426, 149-436, 149-426, 149-416, 149-406, 149-396, 149-386, 149
- the at least one antibody or antigen-binding fragment thereof specifically binds to at least one epitope in the neuropilin c domain, including adjacent linker regions, optionally at about residues 591-794, 600-794, 610-794, 620-794, 630-794, 640-794, 650- 794, 660-794, 670-794, 680-794, 690-794, 700-794, 710-794, 720-794, 730-794, 740-794, 750-794, 760-794, 770-794, 780-794, 790-794, 591-790, 591-780, 591-770, 591-760, 591-750, 591-740, 591- 730, 591-720, 591-710, 591-700, 591-690, 591-680, 591-670, 591-660, 591-650, 591-640, 591-630, 591-620, 591-610, or 591-6
- the at least one antibody or antigen-binding fragment thereof specifically binds to at least one epitope in the neuropilin bl/b2/c combined domain, including adjacent linker regions, optionally at about residues 276-794, 286-794, 296-794, 306-794, 316-794, 326-794, 336-794, 346-794, 356-794, 366-794, 376-794, 387-794, 396-794, 406-794, 416-794, 426- 794, 436-794, 446-794, 456-794, 466-794, 476-794, 486-794, 496-794, 506-794, 516-794, 526-794, 536-794, 546-794, 556-794, 566-794, 576-794, 586-794, 596-794, 606-794, 616-794, 626-794, 636- 794, 646-794, 656-794, 666-794, 676-794, 686-794, 696-794, 706-794, 716-794, 726-794
- the at least one antibody or antigen-binding fragment thereof specifically binds to at least one epitope in the juxtamembrane domain (see Table Nl), optionally selected from one or more of the juxtamembrane domain of NRP2a (variant 1), the juxtamembrane domain of NRP2a (variant 2), the juxtamembrane domain of NRP2a (variant 3), the juxtamembrane domain of NRP2b (variant 4), and the juxtamembrane domain of NRP2b (variant 5), including combinations thereof.
- the at least one antibody or antigen-binding fragment thereof specifically binds to a conformational epitope composed of two or more discontinuous epitope regions, optionally a conformational epitope comprising or consisting of:
- the at least one antibody or antigen-binding fragment thereof modulates binding of the human NRP2 polypeptide to at least one NRP2 ligand (optionally an NRP2 ligand selected from Table N2 or Table N3 and/or a human histidyl-tRNA synthetase (HRS) polypeptide selected from Table HI, optionally a HRS splice variant selected from one or more of SV9 (HRS(l-60)), SV11 (HRS(l-60)+(399-509)) and SV14 (HRS(l-100)+(399-509)).
- NRP2 ligand optionally an NRP2 ligand selected from Table N2 or Table N3 and/or a human histidyl-tRNA synthetase (HRS) polypeptide selected from Table HI, optionally a HRS splice variant selected from one or more of SV9 (HRS(l-60)), SV11 (HRS(l-60)+(399
- the at least one antibody or antigen-binding fragment thereof is a blocking antibody which inhibits about or at least about 80-100% of the theoretical maximal binding between the human NRP2 polypeptide and the least one NRP2 ligand, after pre-incubation with the human NRP2 polypeptide in a stoichiometrically equivalent amount, optionally about or at least about 80, 85, 90, 95, or 100% of the theoretical maximal binding.
- the at least one antibody or antigen-binding fragment thereof is a partial blocking antibody which inhibits about or at least about 20-80% of the theoretical maximal binding between the human NRP2 polypeptide and the at least one NRP2 ligand, after pre-incubation with the human NRP2 polypeptide in a stoichiometrically equivalent amount, optionally about or at least about 20, 25, 30, 35, 40, 45, 50,
- the at least one antibody or antigen-binding fragment thereof specifically binds to an HRS polypeptide-interacting region of the NRP2 polypeptide, and mimics or agonizes one or more signaling activities of the HRS polypeptide binding to the NRP2 polypeptide.
- the at least one antibody or antigen-binding fragment thereof specifically binds to an HRS polypeptide-interacting region of the NRP2 polypeptide, and modulates binding/signaling activity between the NRP2 polypeptide and at least one NRP2 ligand.
- the at least one antibody or antigen-binding fragment thereof antagonizes the binding/signaling activity between the NRP2 polypeptide and the at least one NRP2 ligand.
- the at least one antibody or antigen-binding fragment thereof agonizes or enhances the binding/signaling activity between the NRP2 polypeptide and the at least one NRP2 ligand.
- the at least one NRP2 ligand is selected from: - a VEGF selected from one or more of VEGF-A145, VEGF-A165, VEGF-C, VEGF-D and PIGF-2;
- VEGF receptor selected from VEGFR2 and VEGFR3;
- semaphorin selected from one or more of SEMA3-A, SEMA-3B, SEMA-3C, SEMA-3D SEMA-3F, and SEMA-3G;
- FGF fibroblast growth factor
- FIGF hepatocyte growth factor
- PDGF platelet derived growth factor
- a growth factor receptor selected from one or more of a fibroblast growth factor receptor (FGFR), a hepatocyte growth factor receptor (FIGFR), and a platelet derived growth factor receptor (PDGF);
- FGFR fibroblast growth factor receptor
- FOGFR hepatocyte growth factor receptor
- PDGF platelet derived growth factor receptor
- transcription factor selected from FAC1 and bromoprotein PHD finger transcription factor
- an adaptor protein selected from one or more of GIPC1, GIPC2 and GIPC3;
- an integrin selected from Table N3 optionally one or more of a bi , a b , a b , a b 6, anbb , o ⁇ iand a 6 b 4 ;
- transforming growth factor beta selected from one or more of T ⁇ RbI, T ⁇ Rb2, T ⁇ Rb3, and their corresponding T ⁇ Rb receptors;
- an FIRS polypeptide selected from Table HI optionally an HRS splice variant selected from one or more of HisRS N1 , HisRS N2 , HisRS N3 , HisRS N4 (SV9), HisRS N5 , HisRS cl , HisRS C2 , HisRS C3 , HisRS C4 , HisRS C5 , HisRS ce , HisRS C7 , HisRS C8 (SVll), and HisRS C9 (SV14).
- the at least one antibody or antigen-binding fragment thereof antagonizes the binding/signaling activity between the NRP2 polypeptide and a plexin receptor and/or a semaphorin without substantially modulating the binding/signaling activity between the NRP2 polypeptide and VEGFR2 or VEGFR3 or VEGF-C. In some embodiments, the at least one antibody or antigen-binding fragment thereof antagonizes the binding/signaling activity between the NRP2 polypeptide and a plexin receptor and/or semaphorin without substantially modulating the binding/signaling activity between the NRP2 polypeptide and a HRS polypeptide.
- the at least one antibody or antigen-binding fragment thereof antagonizes the binding/signaling activity between the NRP2 polypeptide and a plexin receptor and/or a semaphorin without substantially modulating the binding/signaling activity between the NRP2 polypeptide and a HRS polypeptide, and without substantially modulating the binding /signaling activity between the NRP2 polypeptide and VEGFR2 or VEGFR3 or VEGF-C.
- the at least one antibody or antigen-binding fragment thereof antagonizes the binding/signaling activity between the NRP2 polypeptide and VEGFR3 without substantially modulating the binding/signaling activity between the NRP2 polypeptide and a plexin receptor and/or a semaphorin. In some embodiments, the at least one antibody or antigen-binding fragment thereof antagonizes the binding/signaling activity between the NRP2 polypeptide and VEGFR3 or VEGF-C without substantially modulating the binding/signaling activity between the NRP2 polypeptide and a different ligand, optionally an FIRS polypeptide.
- the at least one antibody or antigen-binding fragment thereof antagonizes the binding/signaling activity between the NRP2 polypeptide and a plexin receptor without substantially modulating the ligand binding of semaphorin 3 to NRP2.
- the plexin receptor is selected from plexin Al, A2, A3, A4, and Dl.
- the semaphorin is selected from semaphorin 3B, 3C, 3D, 3F, and 3G.
- the at least one antibody or antigen-binding fragment thereof specifically binds to an epitope of at least 5 contiguous amino acids within the human NRP2 a2 domain, wherein the at least one antibody or antigen-binding fragment thereof selectively inhibits receptor dimerization between NRP2 and plexin Al without substantially inhibiting dimerization between NRP2 and FLT4 (VEGFR3).
- the at least one antibody or antigen binding fragment thereof specifically binds to an epitope within amino acids 232-242 of a human NRP2 precursor (see Table Nl).
- the at least one antibody or antigen-binding fragment thereof specifically binds to a discontinuous epitope comprised within amino acids 299- 416 the human NRP2 bl domain, wherein the at least one antibody or antigen-binding fragment thereof selectively inhibits receptor dimerization between NRP2 and FLT4 (VEGFR3) and KDR (VEGFR2) without substantially inhibiting dimerization between NRP2 and plexin Al.
- the at least one antibody or antigen-binding fragment thereof specifically binds to an epitope of at least 5 contiguous amino acids within the human NRP2 b2 domain, wherein the at least one antibody or antigen-binding fragment thereof inhibits receptor dimerization between NRP2 and FLT4 (VEGFR3) and inhibits dimerization between NRP2 and plexin Al.
- the at least one antibody or antigen-binding fragment thereof specifically binds to an epitope of at least 5 contiguous amino acids within the human NRP2 c domain, wherein the at least one antibody or antigen-binding fragment thereof inhibits receptor dimerization between NRP2 and plexin Al and partially inhibits dimerization between NRP2 and FLT4 (VEGFR3).
- the at least one antibody or antigen-binding fragment thereof has an affinity (Kd or EC50) for each of (i) a human NRP2 polypeptide and (ii) the corresponding region of a cynomolgus monkey NRP2 polypeptide, wherein the affinity for (i) and (ii) is within the range of about 20 pM to about 200 pM, about 30 pM to about 300 pM, about 40 pM to about 400 pM, about 50 pM to about 500 pM, about 60 pM to about 600 pM, about 70 pM to about 700 pM, about 80 pM to about 800 pM, about 90 pM to about 900 pM, about 100 pM to about 1 nM, about 0.4 to about 1.2 nM, about 0.9 to about 5.5 nM, about 0.9 to about 5 nM, or about 1 nM to about 10 nM.
- affinity Kd or EC50
- the at least one antibody or antigen-binding fragment thereof has an affinity (Kd or EC50) for each of (i) a human NRP2 polypeptide and (ii) the corresponding region of a murine NRP2 polypeptide, wherein the affinity for (i) and (ii) is within the range of about 20 pM to about 200 pM, about 30 pM to about 300 pM, about 40 pM to about 400 pM, about 50 pM to about 500 pM, about 60 pM to about 600 pM, about 70 pM to about 700 pM, about 80 pM to about 800 pM, about 90 pM to about 900 pM, about 100 pM to about 1 nM, or about 1 nM to about 10 nM.
- affinity Kd or EC50
- the at least one antibody or antigen-binding fragment thereof binds selectively to the NRP2a isoform (optionally variants 1, 2, and/or 3 of Table Nl) of NRP2, and does not substantially bind to the NRP2b isoform (optionally variants 4 and/or 5 of Table Nl). In some embodiments, the at least one antibody or antigen-binding fragment thereof binds selectively to the NRP2b isoform (optionally variants 4 and/or 5 of Table Nl), and does not substantially bind to the NRP2a isoform (optionally variants 1, 2, and/or 3 of Table Nl).
- the at least one antibody or antigen-binding fragment thereof reduces the homo- or hetero-dimerization between NRP2 polypeptides, optionally by about or at least about 20-100% (e.g., about 20, 25, 30, 35, 40, 45, 50, 55, 60, 65, 70, 75, 80, 90, or 100%) after pre-incubation of the anti-NRP2 antibody with the NRP2 polypeptides in a substantially stoichiometrically equivalent amount, optionally in the presence of an NRP2 ligand.
- about 20-100% e.g., about 20, 25, 30, 35, 40, 45, 50, 55, 60, 65, 70, 75, 80, 90, or 100%
- the at least one antibody or antigen-binding fragment thereof enhances the homo- or hetero-dimerization between NRP2 polypeptides, optionally by about or at least about 20-100% (e.g., about 20, 25, 30, 35, 40, 45, 50, 55, 60, 65, 70, 75, 80, 90, or 100%) after pre-incubation of the anti-NRP2 antibody with the NRP2 polypeptides in a substantially stoichiometrically equivalent amount, optionally in the presence of an NRP2 ligand.
- about 20-100% e.g., about 20, 25, 30, 35, 40, 45, 50, 55, 60, 65, 70, 75, 80, 90, or 100%
- the at least one antibody or antigen-binding fragment thereof binds selectively to a human NRP2 polypeptide (see Table Nl) relative to a murine NRP2 polypeptide, optionally where its affinity for the human NRP2 polypeptide is significantly stronger than its affinity for the murine NRP2 polypeptide, optionally by about or at least about 2, 5, 10, 20, 30, 40, 50, 100, 500, or 1000-fold or more.
- the at least one antibody or antigen-binding fragment thereof binds to the human NRP2 polypeptide and does not substantially bind to the murine NRP2 polypeptide, optionally wherein the murine NRP2 polypeptide is a Mus musculus NRP2 polypeptide.
- the at least one antibody or antigen-binding fragment thereof binds to an epitope in the bl domain that comprises residues 299Y, 354N, and 416S, as defined by a human NRP2 precursor sequence (see Table Nl).
- the at least one antibody or antigen-binding fragment thereof comprises an IgA (including subclasses IgAl and lgA2), IgD, IgE, IgG (including subclasses IgGl, lgG2, lgG3, and lgG4), or IgM Fc domain, optionally a human Fc domain, or a hybrid and/or variant thereof.
- the at least one antibody or antigen-binding fragment thereof comprises an IgG Fc domain with high effector function in humans, optionally an IgGl or lgG3 Fc domain.
- the at least one antibody or antigen-binding fragment thereof comprises an IgG Fc domain with low effector function in humans, optionally an lgG2 or lgG4 Fc domain. In some embodiments, the at least one antibody or antigen-binding fragment thereof comprises an IgGl or lgG4 Fc domain, optionally selected from Table FI.
- the at least one antibody or antigen-binding fragment thereof comprises a modified IgGl or lgG4 Fc domain which has altered binding to FcRn, optionally wherein the modified IgGl or lgG4 Fc domain comprises any one or more of YD (M252Y/T256D), DQ (T256D/T307Q), DW (T256D/T307W), YTE (M252Y/S254T/T256E), AAA (T307A/E380A/N434A), LS (M428L/N434S), M252Y, T256D/E, K288D/N, T307Q/W, E380C, N434FY, and/or Y436FI/N/W mutations (EU numbering), including combinations thereof.
- YD M252Y/T256D
- DQ T256D/T307Q
- DW T256D/T307W
- YTE M252Y/
- the at least one antibody or antigen-binding fragment thereof is a monoclonal antibody. In some embodiments, the at least one antibody or antigen-binding fragment thereof is a humanized antibody. In some embodiments, the at least one antibody or antigen binding fragment thereof is an Fv fragment, a single chain Fv (scFv) polypeptide, an adnectin, an anticalin, an aptamer, an avimer, a camelid antibody, a designed ankyrin repeat protein (DARPin), a minibody, a nanobody, or a unibody.
- scFv single chain Fv
- the therapeutic composition has a purity of at least about 80%, 85%, 90%, 95%, 98%, or 99% on a protein basis with respect to the at least one antibody or antigen binding fragment, and is substantially aggregate-free. In some embodiments, the therapeutic composition is substantially endotoxin-free. In some embodiments, the therapeutic composition is a sterile, injectable solution, optionally suitable for intravenous, intramuscular, subcutaneous, or intraperitoneal administration.
- the therapeutic composition further comprises at least one additional agent selected from one or more of a cancer immunotherapy agent, a chemotherapeutic agent, a hormonal therapeutic agent, and a kinase inhibitor.
- the cancer immunotherapy agent is selected from one or more of an immune checkpoint modulatory agent, a cancer vaccine, an oncolytic virus, a cytokine, and a cell-based immunotherapies.
- the immune checkpoint modulatory agent is a polypeptide, optionally an antibody or antigen-binding fragment thereof or a ligand, or a small molecule.
- the immune checkpoint modulatory agent comprises
- the inhibitory immune checkpoint molecule is selected from one or more of Programmed Death-Ligand 1 (PD-L1), Programmed Death 1 (PD-1), Programmed Death- Ligand 2 (PD-L2), Cytotoxic T-Lymphocyte-Associated protein 4 (CTLA-4), Indoleamine 2,3- dioxygenase (IDO), tryptophan 2,3-dioxygenase (TDO), T-cell Immunoglobulin domain and Mucin domain 3 (TIM-3), Lymphocyte Activation Gene-3 (LAG-3), V-domain Ig suppressor of T cell activation (VISTA), B and T Lymphocyte Attenuator (BTLA), CD160, Herpes Virus Entry Mediator (HVEM), and T- cell immunoreceptor with Ig and ITIM domains (TIGIT).
- P-L1 Programmed Death-Ligand 1
- PD-1 Programmed Death 1
- PD-L2 Programmed Death- Ligand 2
- CTLA-4 Cytotoxic T-Lymphocyte-Associated
- the antagonist is a PD-L1 and/or PD-L2 antagonist optionally selected from one or more of an antibody or antigen-binding fragment or small molecule that specifically binds thereto, atezolizumab (MPDL3280A), avelumab (MSB0010718C), and durvalumab (MEDI4736);
- the antagonist is a PD-1 antagonist optionally selected from one or more of an antibody or antigen-binding fragment or small molecule that specifically binds thereto, nivolumab, pembrolizumab, MK-3475, AMP-224, AMP-514, PDR001, and pidilizumab;
- the antagonist is a CTLA-4 antagonist optionally selected from one or more of an antibody or antigen-binding fragment or small molecule that specifically binds thereto, ipilimumab, and tremelimumab;
- the antagonist is an IDO antagonist optionally selected from one or more of an antibody or antigen-binding
- the stimulatory immune checkpoint molecule is selected from one or more of 0X40, CD40, Glucocorticoid-Induced TNFR Family Related Gene (GITR), CD137 (4-1BB),
- HVEM Herpes Virus Entry Mediator
- the agonist is an 0X40 agonist optionally selected from one or more of an antibody or antigen-binding fragment or small molecule or ligand that specifically binds thereto, 0X86, Fc- 0X40 L, and GSK3174998;
- the agonist is a CD40 agonist optionally selected from one or more of an antibody or antigen-binding fragment or small molecule or ligand that specifically binds thereto, CP-870,893, dacetuzumab, Chi Lob 7/4, ADC-1013, and rhCD40L;
- the agonist is a GITR agonist optionally selected from one or more of an antibody or antigen binding fragment or small molecule or ligand that specifically binds thereto, INCAGN01876, DTA-1, and MEDI1873;
- the agonist is a CD137 agonist optionally selected from one or more of an antibody or antigen-binding fragment or small molecule or ligand that specifically binds thereto, utomil
- the cancer vaccine is selected from one or more of Oncophage, a human papillomavirus HPV vaccine optionally Gardasil or Cervarix, a hepatitis B vaccine optionally Engerix-B, Recombivax HB, or Twinrix, and sipuleucel-T (Provenge), or comprises a cancer antigen selected from one or more of human Her2/neu, Herl/EGF receptor (EGFR), Fler3, A33 antigen, B7FI3, CD5, CD19, CD20, CD22, CD23 (IgE Receptor), MAGE-3, C242 antigen, 5T4, IL-6, IL-13, vascular endothelial growth factor VEGF (e.g., VEGF-A) VEGFR-1, VEGFR-2, CD30, CD33, CD37, CD40, CD44, CD51, CD52, CD56, CD74, CD80, CD152, CD200, CD221, CCR4, HLA-DR, CTLA-4, NPC-1
- the oncolytic virus selected from one or more of talimogene laherparepvec (T-VEC), coxsackievirus A21 (CAVATAKTM), Oncorine (H101), pelareorep (REOLYSIN ® ), Seneca Valley virus (NTX-010), Senecavirus SVV-001, ColoAdl, SEPREHVIR (HSV-1716), CGTG-102 (Ad5/3-D24-GMCSF), GL-ONC1, MV-NIS, and DNX-2401.
- T-VEC talimogene laherparepvec
- CAVATAKTM coxsackievirus A21
- Oncorine H101
- pelareorep REOLYSIN ®
- Seneca Valley virus NTX-010
- Senecavirus SVV-001 Senecavirus SVV-001, ColoAdl
- SEPREHVIR HSV-1716
- CGTG-102
- the cytokine selected from one or more of interferon (IFN)-a, IL-2, IL- 12, IL-7, IL-21, and Granulocyte-macrophage colony-stimulating factor (GM-CSF).
- IFN interferon
- IL-2 IL-2
- IL- 12 IL- 12
- IL-7 IL-21
- GM-CSF Granulocyte-macrophage colony-stimulating factor
- the cell-based immunotherapy agent comprises cancer antigen- specific T-cells, optionally ex v/Vo-derived T-cells.
- the cancer antigen-specific T-cells are selected from one or more of chimeric antigen receptor (CAR)-modified T-cells, and T-cell Receptor (TCR)-modified T-cells, tumor infiltrating lymphocytes (TILs), and peptide-induced T-cells.
- CAR chimeric antigen receptor
- TCR T-cell Receptor
- the at least one chemotherapeutic agent is selected from one or more of an alkylating agent, an anti-metabolite, a cytotoxic antibiotic, a topoisomerase inhibitor (type 1 or type II), and an anti-microtubule agent.
- the alkylating agent is selected from one or more of nitrogen mustards (optionally mechlorethamine, cyclophosphamide, mustine, melphalan, chlorambucil, ifosfamide , and busulfan), nitrosoureas (optionally N-Nitroso-N-methylurea (MNU), carmustine (BCNU), lomustine (CCNU), semustine (MeCCNU), fotemustine, and streptozotocin), tetrazines (optionally dacarbazine, mitozolomide, and temozolomide), aziridines (optionally thiotepa, mytomycin, and diaziquone (AZQ)), cisplatins and derivatives thereof (optionally carboplatin and oxaliplatin), and non-classical alkylating agents (optionally procarbazine and hexamethylmelamine); the anti-metabolite is selected from one or more of anti-fo
- the at least one hormonal therapeutic agent is a hormonal agonist or a hormonal antagonist.
- the hormonal agonist is selected from one or more of a progestogen (progestin), a corticosteroid (optionally prednisolone, methylprednisolone, or dexamethasone), insulin like growth factors, VEGF derived angiogenic and lymphangiogenic factors (optionally VEGF-A, VEGF-A145, VEGF-A165, VEGF-C, VEGF-D, PIGF-2), fibroblast growth factor (FGF), galectin, hepatocyte growth factor (FIGF), platelet derived growth factor (PDGF), transforming growth factor (TGF)-beta, an androgen, an estrogen, and a somatostatin analog.
- progestogen progestin
- corticosteroid optionally prednisolone, methylprednisolone, or dexamethasone
- insulin like growth factors VEGF
- the hormonal antagonist is selected from one or more of a hormone synthesis inhibitor, optionally an aromatase inhibitor or a gonadotropin-releasing hormone (GnRFI) or an analog thereof, and a hormone receptor antagonist, optionally a selective estrogen receptor modulator (SERM) or an anti-androgen, or an antibody directed against a hormonal receptor, optionally cixutumumab, dalotuzumab, figitumumab, ganitumab, istiratumab, robatumumab, alacizumab pegol, bevacizumab, icrucumab, ramucirumab, fresolimumab, metelimumab, naxitamab, cetuximab, depatuxizumab mafodotin, futuximab, imgatuzumab, laprituximab emtansine, matuzumab, modotuximab, necitumuma
- the kinase inhibitor is selected from one or more of adavosertib, afanitib, aflibercept, axitinib, bevacizumab, bosutinib, cabozantinib, cetuximab, cobimetinib, crizotinib, dasatinib, entrectinib, erdafitinib, erlotinib, fostamitinib, gefitinib, ibrutinib, imatinib, lapatinib, lenvatinib, mubritinib, nilotinib, panitumumab, pazopanib, pegaptanib, ponatinib, ranibizumab, regorafenib, ruxolitinib, sorafenib, sunitinib, SU6656, tofacitinib
- a therapeutic composition comprising at least one antibody or antigen-binding fragment thereof that specifically binds to a human neuropilin-2 (NRP2) polypeptide, wherein the at least one antibody or antigen-binding fragment thereof modulates (e.g., interferes with) binding of the human NRP2 polypeptide to a human histidyl-tRNA synthetase (HRS) polypeptide, optionally as a therapeutic composition described
- the disease or condition is an NRP2-associated disease or condition.
- the disease or condition is selected from one or more of cancer and diseases and pathways associated with cancer, including cancer cell growth, initiation, migration, adhesion, invasion, chemoresistance, and/or metastasis; diseases associated with inflammation, autoimmunity, and related inflammatory diseases, including diseases associated with inappropriate immune cell activation or migration such as Graft versus host disease (GVHD); diseases associated with lymphatic development, lymphangioma, lymphangiogenesis, and lymphatic damage, including, for example, edema, lymphedema, secondary lymphedema, inappropriate fat absorption and deposition, excess fat deposition, and vascular permeability; diseases associated with infections, including latent infections; diseases associated with allergic disorders/diseases, allergic responses, including, for example, chronic obstructive pulmonary disorder (COPD), neutrophilic asthma, antineutrophil cytoplasmic antibody (ANCA)-associated systemic vasculitis, systemic lupus ery
- COPD chronic o
- the disease is a cancer, optionally wherein the cancer expresses or overexpresses NRP2, optionally wherein the cancer displays NRP2-dependent growth, NRP2- dependent adhesion, NRP2-dependent migration, and/or NRP2-dependent invasion.
- the cancer expresses or overexpresses NRP2 but does not substantially express neuropilin-1 (NRP1).
- NRP1 neuropilin-1
- Certain methods are directed to reducing or preventing re-emergence of a cancer in a subject in need thereof, wherein administration of the therapeutic composition enables generation of an immune memory to the cancer.
- the subject has lymphedema.
- Certain embodiments comprise administering to the subject at least one additional agent selected from one or more of a cancer immunotherapy agent, a chemotherapeutic agent, a hormonal therapeutic agent, and a kinase inhibitor.
- the at least one anti- NRP2 antibody or antigen-binding fragment thereof and the at least one agent are administered separately, as separate compositions.
- the at least one anti-NRP2 antibody and the at least one agent are administered together as part of the same therapeutic composition, optionally as a therapeutic composition described herein.
- the cancer immunotherapy agent is selected from one or more of an immune checkpoint modulatory agent, a cancer vaccine, an oncolytic virus, a cytokine, and a cell-based immunotherapies.
- the immune checkpoint modulatory agent is a polypeptide, optionally an antibody or antigen-binding fragment thereof or a ligand, or a small molecule. In some embodiments, the immune checkpoint modulatory agent comprises
- the inhibitory immune checkpoint molecule is selected from one or more of Programmed Death-Ligand 1 (PD-L1), Programmed Death 1 (PD-1), Programmed Death- Ligand 2 (PD-L2), Cytotoxic T-Lymphocyte-Associated protein 4 (CTLA-4), Indoleamine 2,3- dioxygenase (IDO), tryptophan 2,3-dioxygenase (TDO), T-cell Immunoglobulin domain and Mucin domain 3 (TIM-3), Lymphocyte Activation Gene-3 (LAG-3), V-domain Ig suppressor of T cell activation (VISTA), B and T Lymphocyte Attenuator (BTLA), CD160, Herpes Virus Entry Mediator (HVEM), and T- cell immunoreceptor with Ig and ITIM domains (TIGIT).
- P-L1 Programmed Death-Ligand 1
- PD-1 Programmed Death 1
- PD-L2 Programmed Death- Ligand 2
- CTLA-4 Cytotoxic T-Lymphocyte-Associated
- the antagonist is a PD-L1 and/or PD-L2 antagonist optionally selected from one or more of an antibody or antigen-binding fragment or small molecule that specifically binds thereto, atezolizumab (MPDL3280A), avelumab (MSB0010718C), and durvalumab (MEDI4736), optionally wherein the cancer is selected from one or more of colorectal cancer, melanoma, breast cancer, non-small-cell lung carcinoma, bladder cancer, and renal cell carcinoma; the antagonist is a PD-1 antagonist optionally selected from one or more of an antibody or antigen-binding fragment or small molecule that specifically binds thereto, nivolumab, pembrolizumab, MK-3475, AMP-224, AMP-514PDR001, and pidilizumab, optionally wherein the PD- 1 antagonist is nivolumab and the cancer is optionally selected from one or more of Hodgkin's lympho
- the stimulatory immune checkpoint molecule is selected from one or more of 0X40, CD40, Glucocorticoid-Induced TNFR Family Related Gene (GITR), CD137 (4-1BB),
- the agonist is an 0X40 agonist optionally selected from one or more of an antibody or antigen-binding fragment or small molecule or ligand that specifically binds thereto, 0X86, Fc- 0X40 L, and GSK3174998;
- the agonist is a CD40 agonist optionally selected from one or more of an antibody or antigen-binding fragment or small molecule or ligand that specifically binds thereto, CP-870,893, dacetuzumab, Chi Lob 7/4, ADC-1013, and rhCD40L, and wherein the cancer is optionally selected from one or more of melanoma, pancreatic carcinoma, mesothelioma, and hematological cancers optionally lymphoma such as Non-Hodgkin's lymphoma;
- the agonist is a GITR agonist optionally selected from one or more of an antibody or antigen
- the cancer vaccine is selected from one or more of Oncophage, a human papillomavirus HPV vaccine optionally Gardasil or Cervarix, a hepatitis B vaccine optionally Engerix-B, Recombivax HB, or Twinrix, and sipuleucel-T (Provenge), or comprises a cancer antigen selected from one or more of human Her2/neu, Herl/EGF receptor (EGFR), Her3, A33 antigen, B7H3, CD5, CD19, CD20, CD22, CD23 (IgE Receptor), MAGE-3, C242 antigen, 5T4, IL-6, IL-13, vascular endothelial growth factor VEGF (e.g., VEGF-A) VEGFR-1, VEGFR-2, CD30, CD33, CD37, CD40, CD44, CD51, CD52, CD56, CD74, CD80, CD152, CD200, CD221, CCR4, HLA-DR, CTLA-4, NPC-1C
- the oncolytic virus selected from one or more of talimogene laherparepvec (T-VEC), coxsackievirus A21 (CAVATAKTM), Oncorine (H101), pelareorep (REOLYSIN ® ), Seneca Valley virus (NTX-010), Senecavirus SVV-001, ColoAdl, SEPREHVIR (HSV-1716), CGTG-102 (Ad5/3-D24-GMCSF), GL-ONC1, MV-NIS, and DNX-2401.
- T-VEC talimogene laherparepvec
- CAVATAKTM coxsackievirus A21
- Oncorine H101
- pelareorep REOLYSIN ®
- Seneca Valley virus NTX-010
- Senecavirus SVV-001 Senecavirus SVV-001, ColoAdl
- SEPREHVIR HSV-1716
- CGTG-102
- the cytokine selected from one or more of interferon (IFN)-a, IL-2, IL- 12, IL-7, IL-21, and Granulocyte-macrophage colony-stimulating factor (GM-CSF).
- IFN interferon
- IL-2 IL-2
- IL- 12 IL- 12
- IL-7 IL-21
- GM-CSF Granulocyte-macrophage colony-stimulating factor
- the cell-based immunotherapy agent comprises cancer antigen- specific T-cells, optionally ex v/Vo-derived T-cells.
- the cancer antigen-specific T-cells are selected from one or more of chimeric antigen receptor (CAR)-modified T-cells, and T-cell Receptor (TCR)-modified T-cells, tumor infiltrating lymphocytes (TILs), and peptide-induced T-cells.
- CAR chimeric antigen receptor
- TCR T-cell Receptor
- the at least one chemotherapeutic agent is selected from one or more of an alkylating agent, an anti-metabolite, a cytotoxic antibiotic, a topoisomerase inhibitor (type 1 or type II), and an anti-microtubule agent.
- the alkylating agent is selected from one or more of nitrogen mustards (optionally mechlorethamine, cyclophosphamide, mustine, melphalan, chlorambucil, ifosfamide , and busulfan), nitrosoureas (optionally N-Nitroso-N-methylurea (MNU), carmustine (BCNU), lomustine (CCNU), semustine (MeCCNU), fotemustine, and streptozotocin), tetrazines (optionally dacarbazine, mitozolomide, and temozolomide), aziridines (optionally thiotepa, mytomycin, and diaziquone (AZQ)), cisplatins and derivatives thereof (optionally carboplatin and oxaliplatin), and non-classical alkylating agents (optionally procarbazine and hexamethylmelamine); the anti-metabolite is selected from one or more of anti-fo
- the at least one hormonal therapeutic agent is a hormonal agonist or a hormonal antagonist.
- the hormonal agonist is selected from one or more of a progestogen (progestin), a corticosteroid (optionally prednisolone, methylprednisolone, or dexamethasone), insulin like growth factors, VEGF derived angiogenic and lymphangiogenic factors (optionally VEGF-A, VEGF-A145, VEGF-A165, VEGF-C, VEGF-D, PIGF-2), fibroblast growth factor (FGF), galectin, hepatocyte growth factor (FIGF), platelet derived growth factor (PDGF), transforming growth factor (TGF)-beta, an androgen, an estrogen, and a somatostatin analog.
- progestogen progestin
- corticosteroid optionally prednisolone, methylprednisolone, or dexamethasone
- insulin like growth factors VEGF
- the hormonal antagonist is selected from one or more of a hormone synthesis inhibitor, optionally an aromatase inhibitor or a gonadotropin-releasing hormone (GnRFI) or an analog thereof, and a hormone receptor antagonist, optionally a selective estrogen receptor modulator (SERM) or an anti-androgen, or an antibody directed against a hormonal receptor, optionally cixutumumab, dalotuzumab, figitumumab, ganitumab, istiratumab, robatumumab, alacizumab pegol, bevacizumab, icrucumab, ramucirumab, fresolimumab, metelimumab, naxitamab, cetuximab, depatuxizumab mafodotin, futuximab, imgatuzumab, laprituximab emtansine, matuzumab, modotuximab, necitumuma
- the kinase inhibitor is selected from one or more of adavosertib, afanitib, aflibercept, axitinib, bevacizumab, bosutinib, cabozantinib, cetuximab, cobimetinib, crizotinib, dasatinib, entrectinib, erdafitinib, erlotinib, fostamitinib, gefitinib, ibrutinib, imatinib, lapatinib, lenvatinib, mubritinib, nilotinib, panitumumab, pazopanib, pegaptanib, ponatinib, ranibizumab, regorafenib, ruxolitinib, sorafenib, sunitinib, SU6656, tofacitinib
- the cancer is a primary cancer.
- the cancer is a metastatic cancer, optionally a metastatic cancer that expresses NRP2a and/or NRP2b.
- the cancer is selected from one or more of melanoma (e.g., metastatic melanoma), pancreatic cancer, bone cancer, prostate cancer, small cell lung cancer, non-small cell lung cancer (NSCLC), mesothelioma, leukemia (e.g., lymphocytic leukemia, chronic myelogenous leukemia, acute myeloid leukemia, relapsed acute myeloid leukemia), lymphoma, hepatoma (hepatocellular carcinoma), sarcoma, B-cell malignancy, breast cancer, ovarian cancer, colorectal cancer, glioma, glioblastoma multiforme, meningioma, pituitary adenoma, vestibular schwannoma, primary
- kidney cancer which has metastasized to the adrenal glands, bone, brain, liver, and/or lungs;
- a lung cancer which has metastasized to the adrenal glands, bone, brain, liver, and/or other lung sites;
- pancreatic cancer which has metastasized to the liver, lung, and/or peritoneum;
- the subject has, and/or is selected for treatment based on having, increased circulating or serum levels of at least one NRP2 ligand (optionally an NRP2 ligand from Table N2 or Table N3 and/or an HRS polypeptide from Table HI), either bound or free, relative to the levels of a healthy control or matched control standard or population of subject(s), optionally about or at least about 30, 40, 50, 60, 70, 80, 90, 100, 200, 300, 400, 500, 600, 700, 800, 900, 1000,
- the subject has, and/or is selected for treatment based on having, a disease associated with increased levels or expression of at least one NRP2 ligand (optionally an NRP2 ligand from Table N2 or Table N3 and/or an HRS polypeptide from Table HI) and/or a coding mRNA thereof relative to a healthy control or matched control standard or population of subject(s), optionally a cancer which has increased levels or expression of the at least one NRP2 ligand and/or a coding mRNA thereof relative to a non-cancerous control cell or tissue, optionally relative to a non- cancerous cell or tissue of the same type as the cancer, optionally wherein the HRS polypeptide is a splice variant selected from HisRS N1 , HisRS N2 , HisRS N3 , HisRS N4 , HisRS N5 , HisRS cl , HisRS C2 , HisRS C3 , HisRS C4 , HisRS C5 , HisRS ce ,
- the subject has, and/or is selected for treatment based on having, increased circulating or serum levels of a soluble neuropilin 2 (NRP2) polypeptide (optionally selected from Table Nl), either bound or free, relative to the levels of a healthy control or matched control standard or population of subject(s), optionally circulating or serum levels of about or at least about 10, 20, 30, 50, 100, 200, 300, 400, 500, 600, 700, 800, 900, 1000, 1100, 1200, 1300, 1400, 1500, 1600, 1700, 1800, 1900, 2000, 3000, 4000, 5000 pM of the soluble NRP2 polypeptide, or optionally circulating or serum levels about 30-50, 50-100, 100-2000, 200-2000, 300-2000, 400-2000, 500-2000, 600-2000, 700-2000, 800-2000, 900-2000, 1000-2000, 2000-3000, 3000-4000, 4000-5000 pM of the soluble NRP2 polypeptide.
- NRP2 soluble neuropilin 2
- the subject has, and/or is selected for treatment based on having, a disease associated with increased levels or expression of an NRP2 polypeptide (optionally selected from Table Nl) and/or a coding mRNA thereof relative to a healthy control or matched control standard or population of subject(s), optionally a cancer which has increased levels or expression of an NRP2 polypeptide (optionally selected from Table Nl) and/or a coding mRNA thereof relative to a non-cancerous control cell or tissue, optionally relative to a non-cancerous cell or tissue of the same type as the cancer.
- a disease associated with increased levels or expression of an NRP2 polypeptide optionally selected from Table Nl
- a coding mRNA thereof relative to a healthy control or matched control standard or population of subject(s)
- a cancer which has increased levels or expression of an NRP2 polypeptide (optionally selected from Table Nl) and/or a coding mRNA thereof relative to a non-cancerous control cell or tissue, optional
- the subject has, and/or is selected for treatment based on having, a disease associated with increased levels or expression of NRP2a and/or NRP2b, or an altered ratio of NRP2a:NRP2b expression, relative to a healthy control or matched control standard or population of subject(s).
- the levels of NRP2b are increased by about or at least about 10%, 20%, 30%, 40%, 50%, 100%, 200%, 300%, 400%, 500%, 600%, 700%, 800%, 900%, 1000% compared to a healthy control or matched control standard or population of subject(s).
- the healthy control or matched control standard or population of subject(s) comprises average ranges for age-matched samples of cancerous or non-cancerous cells or tissue of the same type as the cancer, which comprise specific characteristics such as drug resistance, metastatic potential, aggressiveness, genetic signature (optionally p53 mutation(s), PTEN deletion, IGFR expression), and/or expression patterns.
- the subject has, and/or is selected for treatment based on having, increased circulating levels of HRS:NRP2 complexes relative to a healthy or matched control standard or population of subject(s).
- Certain embodiments comprise administering the at least one anti-NRP2 antibody in an amount and at a frequency sufficient to achieve an average, sustained serum or circulating levels of a soluble NRP2 polypeptide of about or less than about 500 pM, 400 pM, 300 pM, 200 pM, lOOpM, 50pm, 40pM, 30 pM, 20 pM, or lOpM. Certain embodiments comprise administering the at least one anti-NRP2 antibody in an amount and at a frequency sufficient to achieve a reduction in the circulating levels of HRS:NRP2 complexes, optionally a reduction of about or at least about 5, 10, 15, 20, 25, 30, 35, 40, 45, 50, 60, 70, 80, 90, 95, 99, or 100%.
- the at least one anti-NRP2 antibody enhances the immune response to the cancer by about, or at least about, 5, 10, 15, 20, 25, 30, 35, 40, 45, 50, 60, 70, 80, 90, 100, 200, 300, 400, 500, 600, 700, 800, 900, 1000, 2000% or more, relative to a control. In some embodiments, the at least one anti-NRP2 antibody reduces the rate of in vitro growth of the cancer by about or at least about 5, 10, 15, 20, 25, 30, 35, 40, 45, 50, 60, 70, 80, 90, 100, 200, 300, 400, 500, 600, 700, 800, 900, 1000, 2000% or more relative to an untreated control.
- the at least one anti-NRP2 antibody reduces the in vitro adhesiveness of the cancer to a substrate by about or at least about, 5, 10, 15, 20, 25, 30, 35, 40, 45, 50, 60, 70, 80, 90, 100, 200, 300, 400, 500, 600, 700,
- the substrate comprises laminin.
- the at least one anti-NRP2 antibody reduces the invasiveness of the cancer by about or at least about 5, 10, 15, 20, 25, 30, 35, 40, 45, 50, 60, 70, 80, 90, 100, 200, 300, 400, 500, 600, 700, 800, 900, 1000, 2000% or more relative to an untreated control. In some embodiments, the at least one anti-NRP2 antibody inhibits the rate of migration or motility of the cancer by about or at least about 5, 10, 15, 20, 25, 30, 35, 40, 45, 50, 60, 70, 80, 90, 100, 200, 300, 400, 500, 600, 700, 800, 900, 1000, 2000% or more relative to an untreated control.
- the at least one anti-NRP2 antibody inhibits the rate of autophagy or endosome maturation (optionally endosome acidification) of the cancer or associated immune cells by about or at least about 5, 10, 15, 20, 25, 30, 35, 40, 45, 50, 60, 70, 80, 90, 100, 200, 300, 400, 500, 600, 700, 800, 900, 1000, 2000% or more relative to an untreated control.
- the at least one anti-NRP2 antibody enhances the susceptibility of the cancer to an additional agent selected from one or more of a chemotherapeutic agent, hormonal therapeutic agent, and kinase inhibitor by about or at least about 5, 10, 15, 20, 25, 30, 35, 40, 45, 50, 60, 70, 80, 90, 100, 200, 300, 400, 500, 600, 700, 800, 900, 1000, 2000% or more relative to the additional agent alone.
- the at least one anti-NRP2 antibody enhances an anti-tumor and/or immunostimulatory activity of the cancer immunotherapy agent by about, or at least about, 5, 10,
- Certain embodiments comprise administering the at least one anti-NRP2 antibody in an amount and at a frequency sufficient to achieve a steady state concentration, or average circulating concentration, of the at least one anti-NRP2 antibody of between about 1 nM and about 1 mM, between about 1 nM and about 100 nM, between about 1 nM and about 10 nM, or between about 1 nM and about 3 mM.
- patient care kits comprising:
- At least one additional agent selected from a cancer immunotherapy agent, a chemotherapeutic agent, a hormonal therapeutic agent, and a kinase inhibitor.
- (a) and (b) are in separate therapeutic compositions. In some embodiments, (a) and (b) are in the same therapeutic composition. In some embodiments, the at least one chemotherapeutic agent is selected from one or more of an alkylating agent, an anti metabolite, a cytotoxic antibiotic, a topoisomerase inhibitor (type 1 or type II), and an anti microtubule agent.
- the alkylating agent is selected from one or more of nitrogen mustards (optionally mechlorethamine, cyclophosphamide, mustine, melphalan, chlorambucil, ifosfamide , and busulfan), nitrosoureas (optionally N-Nitroso-N-methylurea (MNU), carmustine (BCNU), lomustine (CCNU), semustine (MeCCNU), fotemustine, and streptozotocin), tetrazines (optionally dacarbazine, mitozolomide, and temozolomide), aziridines (optionally thiotepa, mytomycin, and diaziquone (AZQ)), cisplatins and derivatives thereof (optionally carboplatin and oxaliplatin), and non-classical alkylating agents (optionally procarbazine and hexamethylmelamine); the anti-metabolite is selected from one or more of anti-fo
- the at least one hormonal therapeutic agent is a hormonal agonist or a hormonal antagonist.
- the hormonal agonist is selected from one or more of a progestogen (progestin), a corticosteroid (optionally prednisolone, methylprednisolone, or dexamethasone), insulin like growth factors, VEGF derived angiogenic and lymphangiogenic factors (optionally VEGF-A, VEGF-A145, VEGF-A165, VEGF-C, VEGF-D, PIGF-2), fibroblast growth factor (FGF), galectin, hepatocyte growth factor (FIGF), platelet derived growth factor (PDGF), transforming growth factor (TGF)-beta, an androgen, an estrogen, and a somatostatin analog.
- progestogen progestin
- corticosteroid optionally prednisolone, methylprednisolone, or dexamethasone
- insulin like growth factors VEGF
- the hormonal antagonist is selected from one or more of a hormone synthesis inhibitor, optionally an aromatase inhibitor or a gonadotropin-releasing hormone (GnRFI) or an analog thereof, and a hormone receptor antagonist, optionally a selective estrogen receptor modulator (SERM) or an anti-androgen, or an antibody directed against a hormonal receptor, optionally cixutumumab, dalotuzumab, figitumumab, ganitumab, istiratumab, robatumumab, alacizumab pegol, bevacizumab, icrucumab, ramucirumab, fresolimumab, metelimumab, naxitamab, cetuximab, depatuxizumab mafodotin, futuximab, imgatuzumab, laprituximab emtansine, matuzumab, modotuximab, necitumuma
- the kinase inhibitor is selected from one or more of adavosertib, afanitib, aflibercept, axitinib, bevacizumab, bosutinib, cabozantinib, cetuximab, cobimetinib, crizotinib, dasatinib, entrectinib, erdafitinib, erlotinib, fostamitinib, gefitinib, ibrutinib, imatinib, lapatinib, lenvatinib, mubritinib, nilotinib, panitumumab, pazopanib, pegaptanib, ponatinib, ranibizumab, regorafenib, ruxolitinib, sorafenib, sunitinib, SU6656, tofacitinib
- bioassay systems comprising a substantially pure anti-NRP2 antibody or antigen-binding fragment thereof, optionally as defined herein, and a host cell line that expresses a human NRP2 polypeptide on the cell surface.
- the NRP2 polypeptide is labeled with a detectable label.
- the anti-NRP2 antibody is labeled with a detectable label.
- the NRP2 polypeptide is functionally coupled to a readout or indicator, such as a fluorescent or luminescent indicator of biological activity of the NRP2 polypeptide.
- the NRP2 polypeptide is selected from Table Nl.
- Certain bioassay systems comprise at least one NRP2 ligand (optionally an NRP2 ligand selected from Table N2 or Table N3 and/or a human histidyl-tRNA synthetase (HRS) polypeptide selected from Table HI), optionally wherein the host cell expresses the at least one NRP2 ligand.
- NRP2 ligand optionally an NRP2 ligand selected from Table N2 or Table N3 and/or a human histidyl-tRNA synthetase (HRS) polypeptide selected from Table HI
- HRS human histidyl-tRNA synthetase
- the HRS polypeptide is selected from Table HI, optionally wherein the HRS polypeptide comprises a HRS splice variant, optionally selected from HisRS N1 , HisRS N2 , HisRS N3 , HisRS N4 , HisRS N5 , HisRS cl , HisRS C2 , HisRS C3 , HisRS C4 , HisRS C5 , HisRS ce , HisRS C7 , HisRS C8 , and HisRS C9 .
- the at least one NRP2 ligand is selected from Table N2 or Table N3.
- detection systems comprising a cell that expresses a human neuropilin 2 (NRP2) polypeptide, at least one NRP2 ligand (optionally a recombinant NRP2 ligand selected from Table N2 or Table N3 and/or a human histidyl-tRNA synthetase (HRS) polypeptide selected from Table HI), and a human or humanized anti-NRP2 antibody or antigen-binding fragment thereof, optionally as defined herein, which modulates the interaction between the NRP2 polypeptide and the at least one NRP2 ligand.
- the anti-NRP2 antibody is labeled with a detectable label.
- the NRP2 polypeptide is selected from Table Nl.
- the HRS polypeptide comprises a HRS splice variant selected from Table HI, optionally selected from HisRS N1 , HisRS N2 , HisRS N3 , HisRS N4 , HisRS N5 , HisRS cl , HisRS C2 , HisRS C3 , HisRS C4 , HisRS C5 , HisRS ce , HisRS C7 , HisRS C8 , and HisRS C9 .
- the at least one NRP2 ligand is selected from Table N2 or Table N3.
- the NRP2 polypeptide and/or the at least one NRP2 ligand is/are functionally coupled to a readout or indicator, such as a fluorescent or luminescent indicator of biological activity of the NRP2 polypeptide or the at least one NRP2 ligand.
- a readout or indicator such as a fluorescent or luminescent indicator of biological activity of the NRP2 polypeptide or the at least one NRP2 ligand.
- diagnostic systems comprising a cell that comprises a neuropilin 2 (NRP2) polypeptide, and at least one NRP2 ligand that specifically binds to the NRP2 polypeptide (optionally an NRP2 ligand selected from Table N2 or Table N3 and/or a human histidyl-tRNA synthetase (HRS) polypeptide selected from Table HI), wherein the cell comprises an indicator molecule that indicates a change in the levels or activity of the NRP2 polypeptide in response to interaction with the at least one NRP2 ligand.
- NRP2 neuropilin 2
- HRS human histidyl-tRNA synthetase
- compositions comprising an engineered population of cells in which at least one cell comprises one or more polynucleotides encoding a human or humanized anti- NRP2 antibody or antigen-binding fragment thereof, as defined herein, wherein the cells are capable of growing in a serum-free medium.
- cellular growth devices comprising a human or humanized anti-NRP2 antibody or antigen-binding fragment thereof, as defined herein, an engineered population of cells in which at least one cell comprises one or more polynucleotides encoding said anti-NRP2 antibody or antigen-binding fragment thereof, at least about 10 liters of a serum-free growth medium, and a sterile container.
- Figures 1A-1B illustrate the general domain structure of neuropilins (1A) and exemplary neuropilin co-receptor functions (IB).
- FIGS 2A-2B illustrate the domain structure of NRP2 isoforms and exemplary NRP2 ligand binding domains. All NRP2 isoforms are identical through the MAM domain, after this, is a short possible retained intron that codes for GENFK. There are then two possible splicing frames (forms a and b), these code different juxtamembrane domains, transmembrane helixes, and cytoplasmic domains. Within the first there is an alternative splice acceptor that removes 17 amino acids (variant 3, or form c). Each form has different spacing from the membrane, which may affect co-receptor specificity. The A/C and B forms, also have different transmembrane domains, where the A/C forms contain a dimerization motif (GXXXG).
- GXXXG dimerization motif
- Figure 3 shows the binding of anti-NRP2 antibodies to clonal Expi293 cells expressing human NRP2.
- the four anti-NRP2 antibodies, and isotype control antibody (human lgG4) were added to human NRP2 expressing cells at the concentrations shown, and cell binding determined by FACS analysis as described in the examples.
- Figure 4 shows the binding of anti-NRP2 antibodies to clonal Expi293 cells expressing cynomolgus monkey NRP2.
- the four anti-NRP2 antibodies, and isotype control antibody (human lgG4) were added to cynomologus monkey NRP2 expressing cells at the concentrations shown, and cell binding determined by FACS analysis as described in the examples.
- Figures 5A-5B show the effects of anti-NRP2 antibodies on NRP2 receptor dimerization with KDR in the presence and absence of VEGF-A.
- the indicated antibodies were assessed in a receptor dimerization assay as described in the examples.
- 5A shows normalized responses for each individual well were calculated to the time point prior to addition of ligand, then normalized to no- antibody/no-ligand (baseline signal). Replicates were then processed to give average response and standard deviation.
- 5B shows the net effect at 80 minutes
- Figures 6A-6B show the effects of anti-NRP2 antibodies on NRP2 receptor dimerization with FLT4 in the presence and absence of VEGF-C.
- the indicated antibodies were assessed in a receptor dimerization assay as described in the examples.
- 6A shows normalized responses for each individual well were calculated to the time point prior to addition of ligand, then normalized to no- antibody/no-ligand (baseline signal). Replicates were then processed to give average response and standard deviation. 6B shows the net effect at 80 minutes
- Figures 7A-7B show the effects of anti-NRP2 antibodies on NRP2 receptor dimerization with PLXNA1 in the presence and absence of SEMA 3F.
- the indicated antibodies were assessed in a receptor dimerization assay as described in the examples.
- 7A shows normalized responses for each individual well were calculated to the time point prior to addition of ligand, then normalized to no- antibody/no-ligand (baseline signal). Replicates were then processed to give average response and standard deviation.
- 7B shows the net effect at 80 minutes
- Figures 8A-8B show the effects of anti-NRP2 antibodies on NRP2 receptor dimerization with KDR in the presence and absence of VEGF-A.
- the indicated antibodies were assessed in a receptor dimerization assay as described in the examples.
- 8A shows normalized responses for each individual well were calculated to the time point prior to addition of ligand, then normalized to no- antibody/no-ligand (baseline signal). Replicates were then processed to give average response and standard deviation.
- 8B shows the net effect at 80 minutes.
- Figured 9A-9B show the effects of anti-NRP2 antibodies on NRP2 receptor dimerization with FLT4 in the presence and absence of VEGF-C.
- the indicated antibodies were assessed in a receptor dimerization assay as described in the examples.
- 9A shows normalized responses for each individual well were calculated to the time point prior to addition of ligand, then normalized to no- antibody/no-ligand (baseline signal). Replicates were then processed to give average response and standard deviation.
- 9B shows the net effect at 80 minutes.
- Figures 10A-10B show the effects of anti-NRP2 antibodies on NRP2 receptor dimerization with PLXN A1 in the presence and absence of SEMA 3F.
- the indicated antibodies were assessed in a receptor dimerization assay as described in the examples.
- 10A shows normalized responses for each individual well were calculated to the time point prior to addition of ligand, then normalized to no- antibody/no-ligand (baseline signal). Replicates were then processed to give average response and standard deviation.
- 10B shows the net effect at 80 minutes
- Figures 11A-11B show the measurement of antibody binding to Expi293 cells over expressing NRP2.
- 11A shows an example of MFI profiles stained with mouse/human reactive control antibody where untransfected cell histogram is shown in light grey, while cells over-expressing mouse NRP2 1383V variant are shown in dark grey. Gating for NRP2 over-expressing cells is shown.
- 11B shows a chart of MFI staining of aNRP2-10vl0 at lOnM of human and mouse wild type NRP2, and mouse NRP2 receptors containing individual mutations representing human residues.
- Figure 12 shows the structure of the human NRP2 bl domain from PBD file 2QQ.K.
- a ribbon diagram showing amino acids 280-426 is displayed. Side chains of residues 299Y, 354N, 416S, and 319T are highlighted in white. Distances between the alpha carbon of 299Y, 354N, and 416S in angstroms are shown alongside a dotted line.
- FIGS 13A-13B shows the inhibitory effect of the anti-NRP2 antibody on anchorage- independent growth and sensitivity to chemotherapeutic agents in triple negative breast cancer cells (TNBC) cells in 3D soft agar colony formation assays.
- the fluorescence readings of the colony formation assay are shown as dot plots with mean ⁇ SEM, for TNBC cells MDA-MB-231 (13A) or BT549 (13B) treated with a-NRP2-10vl0 vs the isotype control hlgG4 at lOOnM in combination with chemo drugs - Cisplatin or 5-FU.
- the statistical significance is indicated by asterisks (* ⁇ 0.05, ** ⁇ 0.01, **** ⁇ 0.0001 by Student's t test). In both cases, the anti-tumor effects of the anti-NRP2 antibody are significantly more pronounced in combination with cisplatin or 5-FU.
- Figure 14 shows the inhibitory effect of the anti-NRP2 antibody in combination with chemotherapeutic agents and a VEGF-A antibody drug (Bevacizumab) on anchorage-independent growth of TNBC MDA-MB-231 cells in 3D methylcellulose colony formation assays.
- the luminescence readings of the colony formation assay are shown as dot plots with mean ⁇ SEM, for TNBC cells MDA-MB-231 treated with aNRP2-10vl0 vs the isotype control hlgG4 at 100 nM in combination with chemo drugs - Cisplatin (at 2 doses) or Bevacizumab (at 100 nM).
- the statistical significance is indicated by asterisks (**p ⁇ 0.01, ***p ⁇ 0.001, ****p ⁇ 0.0001 by Student's t test).
- FIG. 15 shows the inhibition of human lymphatic endothelial cell (HLEC) migration toward vascular endothelial growth factor C (VEGF-C) by antibodies aNRP2-10vl0 and aNRP2-llv7.
- H LECs were inhibited by both NRP2 antibodies to levels consistent with positive control antibodies (aKDR or 3C5) directed against VEGFR2 or VEGFR3 respectively.
- Figure 16 shows that treatment of cells with the antibodies aNRP2-14vlO (NRP2_14) or aNRP2-llv7 (NRP2_11 ) blocked the reduction in phospho-Akt levels upon Semaphorin 3F treatment in U251 glioblastoma cells.
- Treatment of U251 cells with Sema3F results in an approximately 50% decrease in intracellular phospho-Akt levels that can be blocked by both NRP2_11 and NRP2_14, but is not blocked by VEGF-C blocking antibody aNRP2-10vl0 or by mlgGl and hlgG4 control antibodies.
- Figures 17 show a schematic of Sema3F signaling via NRP2. Treatment with Sema3F results in blocking PI3K activity and thereby reducing phospho-Akt levels.
- Figure 18 shows that antibodies aNRP2-14vlO and aNRP22-llv7, but not aNRP2-10vl0, block semaphorin 3F mediated inhibition of AKT phosphorylation.
- Treatment of U251 cells with Sema3F resulted in an approximately 50% decrease in intracellular phospho-Akt levels that can be blocked by both the semaphorin blocking antibodies aNRP2-llv7 and aNRP2-14vlO, but is not blocked by the VEGF-C blocking antibody aNRP2-10vl0 or with mlgGl and hlgG4 control antibodies.
- Figures 19A-19B show that the mouse surrogate VEGF Blocking antibody aNRP2-28 inhibits Tumor Growth in a Murine Melanoma Model (B16.F10). Animals bearing B16-F10 tumors and treated with three doses of the mouse surrogate antibody aNRP2-28, which recognizes mouse NRP2 (and is a functional surrogate for anti-human NRP2 antibody aNRP2-10vl0).
- Figure 19A shows that treatment with the mouse surrogate antibody aNRP2-28 (grey triangles), showed tumor growth inhibition compared to the IgG control group (black squares), and Bevacizumab (black triangles) reaching statistical significance (p ⁇ 0.05) on Day 14, 16, and 19.
- Figure 19B shows terminal tumor weights for each treatment group.
- Figure 20A-20B show the anti-metastatic effects of VEGF-blocker (aNRP2-28) in a model of spontaneous metastasis (4T1).
- Figure 20A shows that animals bearing 4T1 tumors and treated with mouse surrogate antibody aNRP2-28 showed a reduction in metastatic nodules in the lung at termination, reaching statistical significance (p ⁇ 0.05) compared to the IgG control (black bar graph).
- Figure 20B shows serum antibody concentration versus the lung of lung metastases, demonstrating a linear correlation between terminal antibody concentration and number of metastatic nodules
- Figure 21 shows the synergistic effect of VEGF-Blockers (aNRP2-10vl0 /aNRP2-28) in combination with cisplatin in the TNBC Xenograft Model (MDA-MB-231).
- aNRP2-10vl0 /aNRP2-28 VEGF-Blockers
- MDA-MB-231 TNBC Xenograft Model
- the addition of pooled anti-NRP2 antibodies (black symbols) to the cisplatin treatment regimen increased the tumor- inhibitory effect of cisplatin starting on day 40 post inoculation, reaching statistical significance on day 60 compared to the control animals (grey symbols).
- Figure 22 shows that the VEGF Blocker (aNRP2-10vl0) enhances activity of the chemotherapeutic drug 5-FU in the NSCLC Xenograft model (A549).
- the combination of 5-FU and aNRP2-10 performed better than 5-FU with control IgG (grey symbols), evidencing that targeting NRP2 increases the efficacy of the chemotherapeutic drug 5-FU in an art-accepted model of NSCLC. A statistically significant difference was reached on day 51 post cell inoculation
- Figures 23A-23B show that the VEGF Blocker (aNRP2-28) inhibits neo-lymphangiogenesis in an animal model of corneal injury.
- Figure 23A shows representative image scans of Lyve-1 (lymphangiogenic marker) stained corneas of the IgG control and aNRP2-28 group. Plotting the mean values of %Lye-l + area for each treatment group.
- Figure 23B shows a clear trend towards reduced sprouting of lymphatic vessels in the aNRP2-10 treatment groups as compared to the IgG control group.
- Standard techniques may be used for recombinant DNA, oligonucleotide synthesis, and tissue culture and transformation (e.g., electroporation, lipofection). Enzymatic reactions and purification techniques may be performed according to manufacturer's specifications or as commonly accomplished in the art or as described herein. These and related techniques and procedures may be generally performed according to conventional methods well known in the art and as described in various general and more specific references that are cited and discussed throughout the present specification. Unless specific definitions are provided, the nomenclature utilized in connection with, and the laboratory procedures and techniques of, molecular biology, analytical chemistry, synthetic organic chemistry, and medicinal and pharmaceutical chemistry described herein are those well-known and commonly used in the art. Standard techniques may be used for recombinant technology, molecular biological, microbiological, chemical syntheses, chemical analyses, pharmaceutical preparation, formulation, and delivery, and treatment of patients.
- an element includes “one element”, “one or more elements” and/or “at least one element”.
- antigen refers to a molecule or a portion of a molecule capable of being bound by a selective binding agent, such as an antibody, and additionally capable of being used in an animal to produce antibodies capable of binding to an epitope of that antigen.
- An antigen may have one or more epitopes.
- an antigen includes substances that are capable, under appropriate conditions, of inducing an immune response to the substance and of reacting with the products of the immune response.
- an antigen can be recognized by antibodies (humoral immune response) or sensitized T-lymphocytes (T helper or cell-mediated immune response), or both.
- Antigens can be soluble substances, such as toxins and foreign proteins, or particulates, such as bacteria and tissue cells; however, only the portion of the protein or polysaccharide molecule known as the antigenic determinant (epitopes) combines with the antibody or a specific receptor on a lymphocyte.
- the term "antigen” includes any substance to which an antibody binds, or for which antibodies are desired, regardless of whether the substance is immunogenic.
- antibodies can be identified by recombinant methods, independently of any immune response.
- an “antagonist” refers to biological structure or chemical agent that interferes with or otherwise reduces the physiological action of another agent or molecule. In some instances, the antagonist specifically binds to the other agent or molecule. Included are full and partial antagonists.
- an "agonist” refers to biological structure or chemical agent that increases or enhances the physiological action of another agent or molecule. In some instances, the agonist specifically binds to the other agent or molecule. Included are full and partial agonists.
- Anergy refers to the functional inactivation of a T-cell, or B-cell response to re stimulation by antigen.
- amino acid is intended to mean both naturally occurring and non-naturally occurring amino acids as well as amino acid analogs and mimetics.
- Naturally-occurring amino acids include the 20 (L)-amino acids utilized during protein biosynthesis as well as others such as 4-hydroxyproline, hydroxylysine, desmosine, isodesmosine, homocysteine, citrulline and ornithine, for example.
- Non-naturally occurring amino acids include, for example, (D)-amino acids, norleucine, norvaline, p-fluorophenylalanine, ethionine and the like, which are known to a person skilled in the art.
- Amino acid analogs include modified forms of naturally and non-naturally occurring amino acids.
- Such modifications can include, for example, substitution or replacement of chemical groups and moieties on the amino acid or by derivatization of the amino acid.
- Amino acid mimetics include, for example, organic structures which exhibit functionally similar properties such as charge and charge spacing characteristic of the reference amino acid. For example, an organic structure which mimics arginine (Arg or R) would have a positive charge moiety located in similar molecular space and having the same degree of mobility as the e-amino group of the side chain of the naturally occurring Arg amino acid.
- Mimetics also include constrained structures so as to maintain optimal spacing and charge interactions of the amino acid or of the amino acid functional groups. Those skilled in the art know or can determine what structures constitute functionally equivalent amino acid analogs and amino acid mimetics.
- antibody encompasses not only intact polyclonal or monoclonal antibodies, but also fragments thereof (such as dAb, Fab, Fab', F(ab')2, Fv), single chain (ScFv), synthetic variants thereof, naturally occurring variants, fusion proteins comprising an antibody portion with an antigen-binding fragment of the required specificity, humanized antibodies, chimeric antibodies, and any other modified configuration of the immunoglobulin molecule that comprises an antigen-binding site or fragment (epitope recognition site) of the required specificity. Certain features and characteristics of antibodies (and antigen-binding fragments thereof) are described in greater detail herein.
- an antibody or antigen-binding fragment can be of essentially any type.
- an antibody is an immunoglobulin molecule capable of specific binding to a target, such as an immune checkpoint molecule, through at least one epitope recognition site, located in the variable region of the immunoglobulin molecule.
- an antigen-binding fragment refers to a polypeptide fragment that contains at least one CDR of an immunoglobulin heavy and/or light chain that binds to the antigen of interest.
- an antigen-binding fragment of the herein described antibodies may comprise 1, 2, 3, 4, 5, or all 6 CDRs of a V H and V L sequence from antibodies that bind to a target molecule.
- an antibody or antigen-binding fragment thereof specifically binds to a target molecule, for example, an NRP2 polypeptide or an epitope or complex thereof, with an equilibrium dissociation constant that is about or ranges from about ⁇ 10 7 M to about 10 s M. In some embodiments, the equilibrium dissociation constant is about or ranges from about ⁇ 10 9 M to about ⁇ 10 10 M.
- an antibody or antigen-binding fragment thereof has an affinity (Kd or EC50) for a target molecule (to which it specifically binds) of about, at least about, or less than about, 0.01, 0.05, 0.1, 0.2, 0.3, 0.4, 0.5, 0.6, 0.7, 0.8, 0.9, 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 40, or 50 nM.
- a molecule such as a polypeptide or antibody is said to exhibit "specific binding” or “preferential binding” if it reacts or associates more frequently, more rapidly, with greater duration and/or with greater affinity with a particular cell, substance, or particular epitope than it does with alternative cells or substances, or epitopes.
- An antibody “specifically binds” or “preferentially binds” to a target molecule or epitope if it binds with greater affinity, avidity, more readily, and/or with greater duration than it binds to other substances or epitopes, for example, by a statistically significant amount.
- one member of the pair of molecules that exhibit specific binding has an area on its surface, or a cavity, which specifically binds to and is therefore complementary to a particular spatial and/or polar organization of the other member of the pair of molecules.
- the members of the pair have the property of binding specifically to each other.
- an antibody that specifically or preferentially binds to a specific epitope is an antibody that binds that specific epitope with greater affinity, avidity, more readily, and/or with greater duration than it binds to other epitopes. It is also understood by reading this definition that, for example, an antibody (or moiety or epitope) that specifically or preferentially binds to a first target may or may not specifically or preferentially bind to a second target.
- Immunological binding generally refers to the non-covalent interactions of the type which occur between an immunoglobulin molecule and an antigen for which the immunoglobulin is specific, for example by way of illustration and not limitation, as a result of electrostatic, ionic, hydrophilic and/or hydrophobic attractions or repulsion, steric forces, hydrogen bonding, van der Waals forces, and other interactions.
- the strength, or affinity of immunological binding interactions can be expressed in terms of the dissociation constant (Kd) of the interaction, wherein a smaller Kd represents a greater affinity.
- Immunological binding properties of selected polypeptides can be quantified using methods well known in the art. One such method entails measuring the rates of antigen-binding site/antigen complex formation and dissociation, wherein those rates depend on the concentrations of the complex partners, the affinity of the interaction, and on geometric parameters that equally influence the rate in both directions.
- both the "on rate constant” (Kon) and the "off rate constant” (Koff) can be determined by calculation of the concentrations and the actual rates of association and dissociation.
- affinity includes the equilibrium constant for the reversible binding of two agents and is expressed as Kd or EC50.
- Affinity of a binding protein to a ligand such as affinity of an antibody for an epitope can be, for example, from about 100 nanomolar (nM) to about 0.1 nM, from about 100 nM to about 1 picomolar (pM), or from about 100 nM to about 1 femtomolar (fM).
- pM nanomolar
- fM femtomolar
- fM femtomolar
- vidity refers to the resistance of a complex of two or more agents to dissociation after dilution.
- affinity is expressed in the terms of the half maximal effective concentration (ECso), which refers to the concentration of an agent, such as an antibody, or an anti- NRP2 antibody, as disclosed herein, which induces a response halfway between the baseline and maximum after a specified exposure time.
- ECso half maximal effective concentration
- the ECso is commonly used as a measure of an antibody's potency.
- Antibodies may be prepared by any of a variety of techniques known to those of ordinary skill in the art. See, e.g., Harlow and Lane, Antibodies: A Laboratory Manual, Cold Spring Harbor Laboratory, 1988. Monoclonal antibodies specific for a polypeptide of interest may be prepared, for example, using the technique of Kohler and Milstein, Eur. J. Immunol. 6:511-519, 1976, and improvements thereto. Also included are methods that utilize transgenic animals such as mice to express human antibodies.
- Antibodies can also be generated or identified by the use of phage display or yeast display libraries (see, e.g., U.S. Patent No. 7,244,592; Chao et al., Nature Protocols. 1:755-768, 2006).
- HuCAL Human Combinatorial Antibody Library
- human libraries designed with human-donor-sourced fragments encoding a light-chain variable region, a heavy-chain CDR-3, synthetic DNA encoding diversity in heavy-chain CDR-1, and synthetic DNA encoding diversity in heavy-chain CDR-2.
- Other libraries suitable for use will be apparent to persons skilled in the art.
- antibodies and antigen-binding fragments thereof as described herein include a heavy chain and a light chain CDR set, respectively interposed between a heavy chain and a light chain framework region (FR) set which provide support to the CDRs and define the spatial relationship of the CDRs relative to each other.
- CDR set refers to the three hypervariable regions of a heavy or light chain V region. Proceeding from the N-terminus of a heavy or light chain, these regions are denoted as "CDR1," "CDR2,” and “CDR3" respectively.
- An antigen-binding site therefore, includes six CDRs, comprising the CDR set from each of a heavy and a light chain V region.
- a polypeptide comprising a single CDR (e.g., a CDR1, CDR2 or CDR3) is referred to herein as a "molecular recognition unit.” Crystallographic analysis of a number of antigen- antibody complexes has demonstrated that the amino acid residues of CDRs form extensive contact with bound antigen, wherein the most extensive antigen contact is with the heavy chain CDR3. Thus, the molecular recognition units are primarily responsible for the specificity of an antigen-binding site.
- FR set refers to the four flanking amino acid sequences which frame the CDRs of a CDR set of a heavy or light chain V region. Some FR residues may contact bound antigen; however, FRs are primarily responsible for folding the V region into the antigen-binding site, particularly the FR residues directly adjacent to the CDRs. Within FRs, certain amino residues and certain structural features are very highly conserved. In this regard, all V region sequences contain an internal disulfide loop of around 90 amino acid residues. When the V regions fold into a binding- site, the CDRs are displayed as projecting loop motifs which form an antigen-binding surface.
- immunoglobulin variable domains may be determined by reference to Kabat, E. A. et al., Sequences of Proteins of Immunological Interest. 4th Edition. US Department of Health and Fluman Services. 1987, and updates thereof.
- Monoclonal antibodies refer to a homogeneous antibody population wherein the monoclonal antibody is comprised of amino acids (naturally occurring and non-naturally occurring) that are involved in the selective binding of an epitope.
- Monoclonal antibodies are highly specific, being directed against a single epitope.
- monoclonal antibody encompasses not only intact monoclonal antibodies and full-length monoclonal antibodies, but also fragments thereof (such as Fab, Fab', F(ab')2, Fv), single chain (ScFv), variants thereof, fusion proteins comprising an antigen-binding portion, humanized monoclonal antibodies, chimeric monoclonal antibodies, and any other modified configuration of the immunoglobulin molecule that comprises an antigen-binding fragment (epitope recognition site) of the required specificity and the ability to bind to an epitope.
- fragments thereof such as Fab, Fab', F(ab')2, Fv), single chain (ScFv)
- fusion proteins comprising an antigen-binding portion
- humanized monoclonal antibodies chimeric monoclonal antibodies
- any other modified configuration of the immunoglobulin molecule that comprises an antigen-binding fragment (epitope recognition site) of the required specificity and the ability to bind to an epitope.
- the term includes whole immunoglobulins as well as the fragments etc. described above under the definition of "antibody.”
- the proteolytic enzyme papain preferentially cleaves IgG molecules to yield several fragments, two of which (the F(ab) fragments) each comprise a covalent heterodimer that includes an intact antigen-binding site.
- the enzyme pepsin is able to cleave IgG molecules to provide several fragments, including the F(ab')2 fragment which comprises both antigen-binding sites.
- An Fv fragment for use according to certain embodiments can be produced by preferential proteolytic cleavage of an IgM, and on rare occasions of an IgG or IgA immunoglobulin molecule. Fv fragments are, however, more commonly derived using recombinant techniques known in the art.
- the Fv fragment includes a non-covalent VFI::VL heterodimer including an antigen-binding site which retains much of the antigen recognition and binding capabilities of the native antibody molecule. See Inbar et al., PNAS USA. 69:2659-2662, 1972; Hochman et al., Biochem. 15:2706-2710, 1976; and Ehrlich et al., Biochem. 19:4091-4096, 1980.
- single chain Fv (scFV) antibodies are contemplated.
- Kappa bodies III et al., Prot. Eng. 10:949-57, 1997
- minibodies Martin et al., EMBO J 13:5305-9, 1994
- diabodies Holliger et al., PNAS 90: 6444-8, 1993
- Janusins Traunecker et al., EMBO J 10: 3655-59, 1991; and Traunecker et al., Int. J. Cancer Suppl. 7:51-52, 1992
- a single chain Fv (scFv) polypeptide is a covalently linked VH::VL heterodimer which is expressed from a gene fusion including VH- and VL-encoding genes linked by a peptide-encoding linker. Fluston et al. (PNAS USA. 85(16):5879-5883, 1988).
- a number of methods have been described to discern chemical structures for converting the naturally aggregated— but chemically separated— light and heavy polypeptide chains from an antibody V region into an scFv molecule which will fold into a three dimensional structure substantially similar to the structure of an antigen binding site. See, e.g., U.S. Pat. Nos. 5,091,513 and 5,132,405, to Huston et al.; and U.S. Pat. No. 4,946,778, to Ladner et al.
- the antibodies or antigen-binding fragments described herein are in the form of a "diabody.”
- Diabodies are multimers of polypeptides, each polypeptide comprising a first domain comprising a binding region of an immunoglobulin light chain and a second domain comprising a binding region of an immunoglobulin heavy chain, the two domains being linked (e.g., by a peptide linker) but unable to associate with each other to form an antigen-binding site: antigen binding sites are formed by the association of the first domain of one polypeptide within the multimer with the second domain of another polypeptide within the multimer (WO94/13804).
- a dAb fragment of an antibody consists of a VH domain (Ward et al., Nature 341:544-546, 1989).
- Diabodies and other multivalent or multispecific fragments can be constructed, for example, by gene fusion (see WO94/13804; and Holliger et al., PNAS USA. 90:6444-6448, 1993)).
- Minibodies comprising a scFv joined to a CH3 domain are also included (see Hu et al., Cancer Res. 56:3055-3061, 1996). See also Ward et al., Nature. 341:544-546, 1989; Bird et al., Science. 242:423-426, 1988; Huston et al., PNAS USA. 85:5879-5883, 1988); PCT/US92/09965; WO94/13804; and Reiter et al., Nature Biotech. 14:1239-1245, 1996.
- bispecific antibodies may be conventional bispecific antibodies, which can be manufactured in a variety of ways (Holliger and Winter, Current Opinion Biotechnol. 4:446-449, 1993), e.g., prepared chemically or from hybrid hybridomas, or may be any of the bispecific antibody fragments mentioned above.
- Diabodies and scFv can be constructed without an Fc region, using only variable domains, potentially reducing the effects of anti-idiotypic reaction.
- Bispecific diabodies as opposed to bispecific whole antibodies, may also be particularly useful because they can be readily constructed and expressed in E. coli.
- Diabodies (and many other polypeptides such as antibody fragments) of appropriate binding specificities can be readily selected using phage display (WO94/13804) from libraries. If one arm of the diabody is to be kept constant, for instance, with a specificity directed against antigen X, then a library can be made where the other arm is varied and an antibody of appropriate specificity selected.
- Bispecific whole antibodies may be made by knobs-into-holes engineering (Ridgeway et al., Protein Eng., 9:616-621, 1996).
- the antibodies or antigen-binding fragments described herein are in the form of a UniBody ® .
- a UniBody ® is an lgG4 antibody with the hinge region removed (see GenMab Utrecht, The Netherlands; see also, e.g., US20090226421). This antibody technology creates a stable, smaller antibody format with an anticipated longer therapeutic window than current small antibody formats. lgG4 antibodies are considered inert and thus do not interact with the immune system. Fully human lgG4 antibodies may be modified by eliminating the hinge region of the antibody to obtain half-molecule fragments having distinct stability properties relative to the corresponding intact lgG4 (GenMab, Utrecht).
- the antibodies and antigen-binding fragments described herein are in the form of a nanobody.
- Minibodies are encoded by single genes and are efficiently produced in almost all prokaryotic and eukaryotic hosts, for example, E. coli (see U.S. Pat. No. 6,765,087), molds (for example Aspergillus orTrichoderma) and yeast (for example Saccharomyces, Kluyvermyces, Hansenula or Pichia (see U.S. Pat. No. 6,838,254).
- the production process is scalable and multi kilogram quantities of nanobodies have been produced.
- Nanobodies may be formulated as a ready- to-use solution having a long shelf life.
- the Nanoclone method (see WO 06/079372) is a proprietary method for generating Nanobodies against a desired target, based on automated high-throughput selection of B-cells.
- the antibodies or antigen-binding fragments described herein are in the form of an aptamer (see, e.g., Ellington et al., Nature. 346, 818-22, 1990; and Tuerk et al., Science. 249, 505-10, 1990, incorporated by reference).
- aptamers included nucleic acid aptamers (e.g., DNA aptamers, RNA aptamers) and peptide aptamers.
- Nucleic acid aptamers refer generally to nucleic acid species that have been engineered through repeated rounds of in vitro selection or equivalent method, such as SELEX (systematic evolution of ligands by exponential enrichment), to bind to various molecular targets such as small molecules, proteins, nucleic acids, and even cells, tissues and organisms. See, e.g., U.S. Patent Nos. 6,376,190; and 6,387,620, incorporated by reference.
- Peptide aptamers typically include a variable peptide loop attached at both ends to a protein scaffold, a double structural constraint that typically increases the binding affinity of the peptide aptamer to levels comparable to that of an antibody's (e.g., in the nanomolar range).
- the variable loop length may be composed of about 10-20 amino acids (including all integers in between), and the scaffold may include any protein that has good solubility and compacity properties.
- Certain exemplary embodiments utilize the bacterial protein Thioredoxin-A as a scaffold protein, the variable loop being inserted within the reducing active site (-Cys-Gly-Pro-Cys- loop in the wild protein), with the two cysteines lateral chains being able to form a disulfide bridge.
- Methods for identifying peptide aptamers are described, for example, in U.S. Application No. 2003/0108532, incorporated by reference.
- Peptide aptamer selection can be performed using different systems known in the art, including the yeast two-hybrid system.
- the antibodies or antigen-binding fragments described herein are in the form of an avimer.
- Avimers refer to multimeric binding proteins or peptides engineered using in vitro exon shuffling and phage display. Multiple binding domains are linked, resulting in greater affinity and specificity compared to single epitope immunoglobulin domains. See, e.g., Silverman et al., Nature Biotechnology. 23:1556-1561, 2005; U.S. Patent No. 7,166,697; and U.S. Application Nos. 2004/0175756, 2005/0048512, 2005/0053973, 2005/0089932 and 2005/0221384, incorporated by reference.
- the antibodies or antigen-binding fragments described herein are in the form of an adnectin.
- Adnectins refer to a class of targeted biologies derived from human fibronectin, an abundant extracellular protein that naturally binds to other proteins. See, e.g., U.S. Application Nos. 2007/0082365; 2008/0139791; and 2008/0220049, incorporated by reference.
- Adnectins typically consists of a natural fibronectin backbone, as well as the multiple targeting domains of a specific portion of human fibronectin. The targeting domains can be engineered to enable an adnectin to specifically recognize an NRP2 polypeptide or an epitope thereof.
- the antibodies or antigen-binding fragments described herein are in the form of an anticalin.
- Anticalins refer to a class of antibody mimetics that are typically synthesized from human lipocalins, a family of binding proteins with a hypervariable loop region supported by a structurally rigid framework. See, e.g., U.S. Application No. 2006/0058510.
- Anticalins typically have a size of about 20 kDa.
- Anticalins can be characterized by a barrel structure formed by eight antiparallel b-strands (a stable b-barrel scaffold) that are pairwise connected by four peptide loops and an attached a-helix. In certain aspects, conformational deviations to achieve specific binding are made in the hypervariable loop region(s). See, e.g., Skerra, FEBS J. 275:2677-83, 2008, incorporated by reference.
- the antibodies or antigen-binding fragments described herein are in the form of a designed ankyrin repeat protein (DARPin).
- DARPins include a class of non immunoglobulin proteins that can offer advantages over antibodies for target binding in drug discovery and drug development.
- DARPins are ideally suited for in vivo imaging or delivery of toxins or other therapeutic payloads because of their favorable molecular properties, including small size and high stability. The low-cost production in bacteria and the rapid generation of many target-specific DARPins make the DARPin approach useful for drug discovery.
- DARPins can be easily generated in multispecific formats, offering the potential to target an effector DARPin to a specific organ or to target multiple receptors with one molecule composed of several DARPins. See, e.g., Stumpp et al., Curr Opin Drug Discov Devel. 10:153-159, 2007; U.S. Application No. 2009/0082274; and PCT/EP2001/10454, incorporated by reference.
- heavy chain dimers such as antibodies from camelids and sharks.
- Camelid and shark antibodies comprise a homodimeric pair of two chains of V-like and C-like domains (neither has a light chain). Since the VH region of a heavy chain dimer IgG in a camelid does not have to make hydrophobic interactions with a light chain, the region in the heavy chain that normally contacts a light chain is changed to hydrophilic amino acid residues in a camelid. VH domains of heavy-chain dimer IgGs are called VHH domains.
- Shark Ig-NARs comprise a homodimer of one variable domain (termed a V-NAR domain) and five C-like constant domains (C-NAR domains).
- camelids the diversity of antibody repertoire is determined by the complementary determining regions (CDR) 1, 2, and 3 in the VH or VHH regions.
- the CDR3 in the camel VHH region is characterized by its relatively long length averaging 16 amino acids (Muyldermans et al., 1994, Protein Engineering 7(9): 1129). This is in contrast to CDR3 regions of antibodies of many other species.
- the CDR3 of mouse VH has an average of 9 amino acids.
- the antibodies or antigen-binding fragments thereof are humanized. These embodiments refer to a chimeric molecule, generally prepared using recombinant techniques, having an antigen-binding site derived from an immunoglobulin from a non-human species and the remaining immunoglobulin structure of the molecule based upon the structure and/or sequence of a human immunoglobulin.
- the antigen-binding site may comprise either complete variable domains fused onto constant domains or only the CDRs grafted onto appropriate framework regions in the variable domains.
- Epitope binding sites may be wild type or modified by one or more amino acid substitutions.
- variable regions of both heavy and light chains contain three complementarity determining regions (CDRs) which vary in response to the epitopes in question and determine binding capability, flanked by four framework regions (FRs) which are relatively conserved in a given species and which putatively provide a scaffolding for the CDRs.
- CDRs complementarity determining regions
- FRs framework regions
- humanized antibodies preserve all CDR sequences (for example, a humanized mouse antibody which contains all six CDRs from the mouse antibodies).
- humanized antibodies have one or more CDRs (one, two, three, four, five, six) which are altered with respect to the original antibody, which are also termed one or more CDRs "derived from" one or more CDRs from the original antibody.
- the antibodies are "chimeric" antibodies.
- a chimeric antibody is comprised of an antigen-binding fragment of an antibody operably linked or otherwise fused to a heterologous Fc portion of a different antibody.
- the Fc domain or heterologous Fc domain is of human origin.
- the Fc domain or heterologous Fc domain is of mouse origin.
- the heterologous Fc domain may be from a different Ig class from the parent antibody, including IgA (including subclasses IgAl and lgA2), IgD, IgE, IgG (including subclasses IgGl, lgG2, lgG3, and lgG4), and IgM.
- the heterologous Fc domain may be comprised of CH2 and CH3 domains from one or more of the different Ig classes.
- the antigen-binding fragment of a chimeric antibody may comprise only one or more of the CDRs of the antibodies described herein (e.g., 1, 2, 3, 4, 5, or 6 CDRs of the antibodies described herein), or may comprise an entire variable domain (VL, VH or both).
- a subject “at risk” of developing a disease, or adverse reaction may or may not have detectable disease, or symptoms of disease, and may or may not have displayed detectable disease or symptoms of disease prior to the treatment methods described herein.
- “At risk” denotes that a subject has one or more risk factors, which are measurable parameters that correlate with development of a disease, as described herein and known in the art. A subject having one or more of these risk factors has a higher probability of developing disease, or an adverse reaction than a subject without one or more of these risk factor(s).
- Biocompatible refers to materials or compounds which are generally not injurious to biological functions of a cell or subject and which will not result in any degree of unacceptable toxicity, including allergenic and disease states.
- binding refers to a direct association between two molecules, due to, for example, covalent, electrostatic, hydrophobic, and ionic and/or hydrogen-bond interactions, including interactions such as salt bridges and water bridges.
- chemoresistance refers to the change in therapeutic sensitivity of a cancer cell population over time following exposure to chemotherapy, including resistance to at least one of a cancer immunotherapy agent, a chemotherapeutic agent, a hormonal therapeutic agent, and/or a kinase inhibitor.
- chemoresistance leads to the relapse and/or metastasis, of the cancer, and challenges the improvement of clinical outcome for the cancer patients. It remains the main obstacle to long term successful cancer therapy. For example, approximately 30 percent of women diagnosed with early-stage breast cancer ultimately develop resistance and eventually progress to metastatic breast cancer.
- chemoresistance include the induction of transporter pumps, oncogenes, tumor suppressor genes, mitochondrial alteration, DNA repair, autophagy, epithelial-mesenchymal transition (EMT), cancer sternness, and exosome production.
- EMT epithelial-mesenchymal transition
- exosome production processes may operate via distinct mechanisms, alone or in combination with each other, but ultimately coordinate to prevent cell death in response to a specific targeted chemotherapeutic agent.
- EMT epithelial-mesenchymal transition
- coding sequence is meant any nucleic acid sequence that contributes to the code for the polypeptide product of a gene.
- non-coding sequence refers to any nucleic acid sequence that does not directly contribute to the code for the polypeptide product of a gene.
- effector function in the context of antibodies refers to the ability of that antibody to engage with other arms of the immune system, including for example, the activation of the classical complement pathway, or through engagement of Fc receptors.
- Complement dependent pathways are primarily driven by the interaction of Clq with the Cl complex with clustered antibody Fc domains.
- Antibody dependent cellular cytotoxicity is primarily driven by the interaction of Fc receptors (FcRs) on the surface of effector cells (natural killer cells, macrophages, monocytes and eosinophils) which bind to the Fc region of an IgG which itself is bound to a target cell.
- Fc receptors are key immune regulatory receptors connecting the antibody mediated (humoral) immune response to cellular effector functions. Receptors for all classes of immunoglobulins have been identified, including FcyR (IgG), FceRI (IgE), FcaRI (IgA), FcpR (IgM) and Fc6R (IgD). There are at least three classes of receptors for human IgG found on leukocytes: CD64 (FcyRI), CD32 (FcyRIla, FcyRIIb and FcyRIIc) and CD16 (FcyRIIIa and FcyRIIIb).
- FcyR I is classed as a high affinity receptor (nanomolar range KD) while FcyRII and FcyRIII are low to intermediate affinity (micromolar range KD).
- Fc binding Upon Fc binding a signaling pathway is triggered which results in the secretion of various substances, such as lytic enzymes, perforin, granzymes and tumour necrosis factor, which mediate in the destruction of the target cell.
- the level of ADCC effector function various for human IgG subtypes. Although this is dependent on the allotype and specific FcvR, in simple terms ADCC effector function is "high" for human IgGl and lgG3, and “low” for lgG2 and lgG4.
- endotoxin free or “substantially endotoxin free” relates generally to compositions, solvents, and/or vessels that contain at most trace amounts (e.g., amounts having no clinically adverse physiological effects to a subject) of endotoxin, and preferably undetectable amounts of endotoxin.
- Endotoxins are toxins associated with certain micro-organisms, such as bacteria, typically gram-negative bacteria, although endotoxins may be found in gram-positive bacteria, such as Listeria monocytogenes.
- LPS lipopolysaccharides
- LOS lipo-oligo-saccharides
- a depyrogenation oven may be used for this purpose, as temperatures in excess of 300°C are typically required to break down most endotoxins. For instance, based on primary packaging material such as syringes or vials, the combination of a glass temperature of 250°C and a holding time of 30 minutes is often sufficient to achieve a 3 log reduction in endotoxin levels.
- Other methods of removing endotoxins are contemplated, including, for example, chromatography and filtration methods, as described herein and known in the art. Endotoxins can be detected using routine techniques known in the art.
- the Limulus Amoebocyte Lysate assay which utilizes blood from the horseshoe crab, is a very sensitive assay for detecting presence of endotoxin.
- very low levels of LPS can cause detectable coagulation of the limulus lysate due a powerful enzymatic cascade that amplifies this reaction.
- Endotoxins can also be quantitated by enzyme-linked immunosorbent assay (ELISA).
- endotoxin levels may be less than about 0.001, 0.005, 0.01, 0.02, 0.03, 0.04, 0.05, 0.06, 0.08, 0.09, 0.1, 0.5, 1.0, 1.5, 2, 2.5, 3, 4, 5, 6, 7, 8, 9, or 10 EU/mg of active compound.
- 1 ng lipopolysaccharide (LPS) corresponds to about 1-10 EU.
- epitope includes any determinant, preferably a polypeptide determinant, capable of specific binding to an immunoglobulin or T-cell receptor.
- An epitope includes a region of an antigen that is bound by an antibody.
- epitope determinants include chemically active surface groupings of molecules such as amino acids, sugar side chains, phosphoryl or sulfonyl, and may in certain embodiments have specific three-dimensional structural characteristics, and/or specific charge characteristics. Epitopes can be contiguous or non-contiguous in relation to the primary structure of the antigen, for example, an NRP2 polypeptide.
- an epitope comprises, consists, or consists essentially of about, at least about, or no more than about 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, or 20 contiguous amino acids (i.e., a linear epitope) or non-contiguous amino acids (i.e., conformational epitope) of a reference sequence (see, e.g., Table Nl) or target molecule described herein.
- An “epitope” includes that portion of an antigen or other macromolecule capable of forming a binding interaction that interacts with the variable region binding pocket of a binding protein. Such binding interaction can be manifested as an intermolecular contact with one or more amino acid residues of a CDR.
- Antigen binding can involve a CDR3 or a CDR3 pair.
- An epitope can be a linear peptide sequence (i.e., “continuous") or can be composed of noncontiguous amino acid sequences (i.e., "conformational” or “discontinuous”).
- a binding protein can recognize one or more amino acid sequences; therefore an epitope can define more than one distinct amino acid sequence.
- Epitopes recognized by binding protein can be determined by peptide mapping and sequence analysis techniques well known to one of skill in the art.
- a "cryptic epitope” or a “cryptic binding site” is an epitope or binding site of a protein sequence that is not exposed or substantially protected from recognition within an unmodified polypeptide, but is capable of being recognized by a binding protein of a denatured or proteolyzed polypeptide. Amino acid sequences that are not exposed, or are only partially exposed, in the unmodified polypeptide structure are potential cryptic epitopes. If an epitope is not exposed, or only partially exposed, then it is likely that it is buried within the interior of the polypeptide.
- Candidate cryptic epitopes can be identified, for example, by examining the three-dimensional structure of an unmodified polypeptide.
- EC50 half maximal effective concentration
- concentration of an agent e.g., antibody
- the EC50 of a graded dose response curve therefore represents the concentration of a compound at which 50% of its maximal effect is observed.
- EC50 also represents the plasma concentration required for obtaining 50% of a maximum effect in vivo.
- EC90 refers to the concentration of an agent or composition at which 90% of its maximal effect is observed. The “EC90” can be calculated from the “EC50” and the Hill slope, or it can be determined from the data directly, using routine knowledge in the art.
- the EC50 of an agent is less than about 0.01, 0.05, 0.1, 0.2, 0.3, 0.4, 0.5, 0.6, 0.7, 0.8, 0.9, 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 25, 30, 40, 50,
- an agent will have an EC 5 0 value of about InM or less.
- Immuno response means any immunological response originating from immune system, including responses from the cellular and humeral, innate and adaptive immune systems.
- exemplary cellular immune cells include for example, lymphocytes, macrophages, T cells, B cells, NK cells, neutrophils, eosinophils, dendritic cells, mast cells, monocytes, and all subsets thereof.
- Cellular responses include for example, effector function, cytokine release, phagocytosis, efferocytosis, translocation, trafficking, proliferation, differentiation, activation, repression, cell-cell interactions, apoptosis, etc.
- Humeral responses include for example IgG, IgM, IgA, IgE, responses and their corresponding effector functions.
- half-life of an agent such as an antibody can refer to the time it takes for the agent to lose half of its pharmacologic, physiologic, or other activity, relative to such activity at the time of administration into the serum or tissue of an organism, or relative to any other defined time-point.
- “Half-life” can also refer to the time it takes for the amount or concentration of an agent to be reduced by half of a starting amount administered into the serum or tissue of an organism, relative to such amount or concentration at the time of administration into the serum or tissue of an organism, or relative to any other defined time-point.
- the half-life can be measured in serum and/or any one or more selected tissues.
- modulating and “altering” include “increasing,” “enhancing” or “stimulating,” as well as “decreasing” or “reducing,” typically in a statistically significant or a physiologically significant amount or degree relative to a control.
- An “increased,” “stimulated” or “enhanced” amount is typically a “statistically significant” amount, and may include an increase that is 1.1, 1.2, 1.5, 2, 3, 4, 5, 6, 7, 8, 9, 10, 15, 20, 30, 40, 50, 60, 70, 80, 90, 100 or more times (e.g., 500, 1000 times) (including all integers and ranges in between e.g., 1.5, 1.6, 1.7.
- a "decreased” or “reduced” amount is typically a "statistically significant” amount, and may include a 1%, 2%, 3%, 4%, 5%, 6%, 7%, 8%, 9%, 10%, 11%, 12%, 13%, 14%, 15%, 16%, 17%, 18% , 19%, 20%, 25%, 30%, 35%, 40%, 45%, 50%, 55%, 60%, 65%, 70%, 75%, 80%, 85%, 90%, 95%, or 100% decrease (including all integers and ranges in between) in the amount produced by no composition (e.g., the absence of an agent) or a control composition. Examples of comparisons and "statistically significant" amounts are described herein.
- migratory cells refers to cells that are capable of movement from one place to another in response to a stimulus.
- exemplary migratory cells include immune cells such as monocytes, Natural Killer (NK) cells, dendritic cells (immature or mature), subsets of dendritic cells including myeloid, plasmacytoid (also called lymphoid) and Langerhans cells, macrophages such as histiocytes, tissue resident macrophages such as Kupffer's cells, microglia cells in the CNS, alveolar macrophages, and peritoneal macrophages, macrophage subtypes such as M0, Ml, Mox,M2a, M2b, and M2c macrophages, neutrophils, eosinophils, mast cells, basophils, B cells including plasma B cells, memory B cells, B-l cells, and B-2 cells, CD45RO (naive T) cells, CD45RA (memory T) cells, CD4 Helper T Cell
- migratory cells include fibroblasts, fibrocytes, tumor cells, and stem cells.
- cell migration refers to the movement of migratory cells
- modulation of cell migration refers to the modulation of the movement of any such migratory cells.
- polypeptide protein
- peptide a polymer of amino acids not limited to any particular length.
- enzyme includes polypeptide or protein catalysts. The terms include modifications such as myristoylation, sulfation, glycosylation, phosphorylation and addition or deletion of signal sequences.
- polypeptide or protein means one or more chains of amino acids, wherein each chain comprises amino acids covalently linked by peptide bonds, and wherein said polypeptide or protein can comprise a plurality of chains non-covalently and/or covalently linked together by peptide bonds, having the sequence of native proteins, that is, proteins produced by naturally-occurring and specifically non-recombinant cells, or genetically-engineered or recombinant cells, and comprise molecules having the amino acid sequence of the native protein, or molecules having deletions from, additions to, and/or substitutions of one or more amino acids of the native sequence.
- the polypeptide is a "recombinant" polypeptide, produced by recombinant cell that comprises one or more recombinant DNA molecules, which are typically made of heterologous polynucleotide sequences or combinations of polynucleotide sequences that would not otherwise be found in the cell.
- polynucleotide and “nucleic acid” includes mRNA, RNA, cRNA, cDNA, and DNA.
- the term typically refers to polymeric form of nucleotides of at least 10 bases in length, either ribonucleotides or deoxynucleotides or a modified form of either type of nucleotide.
- the term includes single and double stranded forms of DNA.
- isolated DNA and isolated polynucleotide and “isolated nucleic acid” refer to a molecule that has been isolated free of total genomic DNA of a particular species.
- an isolated DNA segment encoding a polypeptide refers to a DNA segment that contains one or more coding sequences yet is substantially isolated away from, or purified free from, total genomic DNA of the species from which the DNA segment is obtained. Also included are non-coding polynucleotides (e.g., primers, probes, oligonucleotides), which do not encode a polypeptide. Also included are recombinant vectors, including, for example, expression vectors, viral vectors, plasmids, cosmids, phagemids, phage, viruses, and the like.
- Additional coding or non-coding sequences may, but need not, be present within a polynucleotide described herein, and a polynucleotide may, but need not, be linked to other molecules and/or support materials.
- a polynucleotide or expressible polynucleotides regardless of the length of the coding sequence itself, may be combined with other sequences, for example, expression control sequences.
- “Expression control sequences” include regulatory sequences of nucleic acids, or the corresponding amino acids, such as promoters, leaders, enhancers, introns, recognition motifs for RNA, or DNA binding proteins, polyadenylation signals, terminators, internal ribosome entry sites (IRES), secretion signals, subcellular localization signals, and the like, which have the ability to affect the transcription or translation, or subcellular, or cellular location of a coding sequence in a host cell. Exemplary expression control sequences are described in Goeddel; Gene Expression Technology: Methods in Enzymology 185, Academic Press, San Diego, Calif. (1990).
- a “promoter” is a DNA regulatory region capable of binding RNA polymerase in a cell and initiating transcription of a downstream (3' direction) coding sequence.
- the promoter sequence is bounded at its 3' terminus by the transcription initiation site and extends upstream (5' direction) to include the minimum number of bases or elements necessary to initiate transcription at levels detectable above background.
- a transcription initiation site (conveniently defined by mapping with nuclease SI) can be found within a promoter sequence, as well as protein binding domains (consensus sequences) responsible for the binding of RNA polymerase.
- Eukaryotic promoters can often, but not always, contain "TATA" boxes and "CAT” boxes.
- Prokaryotic promoters contain Shine- Dalgarno sequences in addition to the -10 and -35 consensus sequences.
- promoters including constitutive, inducible and repressible promoters, from a variety of different sources are well known in the art.
- Representative sources include for example, viral, mammalian, insect, plant, yeast, and bacterial cell types), and suitable promoters from these sources are readily available, or can be made synthetically, based on sequences publicly available on line or, for example, from depositories such as the ATCC as well as other commercial or individual sources.
- Promoters can be unidirectional (i.e., initiate transcription in one direction) or bi directional (i.e., initiate transcription in either a 3' or 5' direction).
- Non-limiting examples of promoters include, for example, the T7 bacterial expression system, pBAD (araA) bacterial expression system, the cytomegalovirus (CMV) promoter, the SV40 promoter, the RSV promoter.
- Inducible promoters include the Tet system, (US Patents 5,464,758 and 5,814,618), the Ecdysone inducible system (No et al., Proc. Natl. Acad. Sci.
- an "expressible polynucleotide” includes a cDNA, RNA, mRNA or other polynucleotide that comprises at least one coding sequence and optionally at least one expression control sequence, for example, a transcriptional and/or translational regulatory element, and which can express an encoded polypeptide upon introduction into a cell, for example, a cell in a subject.
- adenoviral vectors that can be utilized to deliver an expressible polynucleotide
- retroviral vectors include adenoviral vectors, herpes virus vectors, vaccinia virus vectors, adeno-associated virus (AAV) vectors, and retroviral vectors.
- the retroviral vector is a derivative of a murine or avian retrovirus, or is a lentiviral vector.
- retroviral vectors in which a single foreign gene can be inserted include, but are not limited to: Moloney murine leukemia virus (MoMuLV), Harvey murine sarcoma virus (HaMuSV), murine mammary tumor virus (MuMTV), SIV, BIV, HIV and Rous Sarcoma Virus (RSV).
- MoMuLV Moloney murine leukemia virus
- HaMuSV Harvey murine sarcoma virus
- MuMTV murine mammary tumor virus
- SIV BIV
- HIV Rous Sar
- retroviral vectors can incorporate multiple genes. All of these vectors can transfer or incorporate a gene for a selectable marker so that transduced cells can be identified and generated.
- the vector By inserting a polypeptide sequence of interest into the viral vector, along with another gene that encodes the ligand for a receptor on a specific target cell, for example, the vector may be made target specific.
- Retroviral vectors can be made target specific by inserting, for example, a polynucleotide encoding a protein. Illustrative targeting may be accomplished by using an antibody to target the retroviral vector. Those of skill in the art will know of, or can readily ascertain without undue experimentation, specific polynucleotide sequences which can be inserted into the retroviral genome to allow target specific delivery of the retroviral vector.
- the expressible polynucleotide is a modified RNA or modified mRNA polynucleotide, for example, a non-naturally occurring RNA analog.
- the modified RNA or mRNA polypeptide comprises one or more modified or non-natural bases, for example, a nucleotide base other than adenine (A), guanine (G), cytosine (C), thymine (T), and/or uracil (U).
- the modified mRNA comprises one or more modified or non natural internucleotide linkages.
- RNA polynucleotides for delivering an encoded therapeutic polypeptide are described, for example, in Kormann et al., Nat Biotechnol. 29:154-7, 2011; and U.S. Application Nos. 2015/0111248; 2014/0243399; 2014/0147454; and 2013/0245104, which are incorporated by reference in their entireties.
- isolated polypeptide or protein referred to herein means that a subject protein (1) is free of at least some other proteins with which it would typically be found in nature, (2) is essentially free of other proteins from the same source, e.g., from the same species, (3) is expressed by a cell from a different species, (4) has been separated from at least about 50 percent of polynucleotides, lipids, carbohydrates, or other materials with which it is associated in nature, (5) is not associated (by covalent or non-covalent interaction) with portions of a protein with which the "isolated protein" is associated in nature, (6) is operably associated (by covalent or non-covalent interaction) with a polypeptide with which it is not associated in nature, or (7) does not occur in nature.
- Such an isolated protein can be encoded by genomic DNA, cDNA, mRNA or other RNA, of may be of synthetic origin, or any combination thereof.
- the isolated protein is substantially free from proteins or polypeptides or other contaminants that are found in its natural environment that would interfere with its use (therapeutic, diagnostic, prophylactic, research or otherwise).
- the "purity" of any given agent (e.g., polypeptide such as an antibody) in a composition may be defined.
- certain compositions may comprise an agent such as a polypeptide agent that is at least 80%, 85%, 90%, 91%, 92%, 93%, 94%, 95%, 96%, 97%, 98%, 99%, or 100% pure on a protein basis or a weight-weight basis, including all decimals and ranges in between, as measured, for example and by no means limiting, by high performance liquid chromatography (HPLC), a well-known form of column chromatography used frequently in biochemistry and analytical chemistry to separate, identify, and quantify compounds.
- HPLC high performance liquid chromatography
- a “lipid nanoparticle” or “solid lipid nanoparticle” refers to one or more spherical nanoparticles with an average diameter of between about 10 to about 1000 nanometers, and which comprise a solid lipid core matrix that can solubilize lipophilic molecules.
- the lipid core is stabilized by surfactants (e.g., emulsifiers), and can comprise one or more of triglycerides (e.g., tristearin), diglycerides (e.g., glycerol bahenate), monoglycerides (e.g., glycerol monostearate), fatty acids (e.g., stearic acid), steroids (e.g., cholesterol), and waxes (e.g., cetyl palmitate), including combinations thereof.
- surfactants e.g., emulsifiers
- emulsifiers can comprise one or more of triglycerides (e.g., tristearin), diglycerides (e.g., glycerol bahenate), monoglycerides (e.g., glycerol monostearate), fatty acids (e.g., stearic acid), steroids (e.g., cholesterol), and waxes (e.g.,
- compositions described herein are formulated with one or more lipid nanoparticles.
- Neuron 2-associated disease refers to diseases and conditions in which NRP2 activity, expression, and/or spatial distribution plays a role in the pathophysiology of that disease or condition.
- NRP2 associated diseases are modulated by the anti-NRP2 antibodies of the present disclosure by altering the interaction of NRP2 with at least one NRP2 ligand to impact NRP2 activity, signaling, expression, and/or spatial distribution.
- Exemplary NRP2-associated diseases and conditions include without limitation, cancer and diseases or pathologies associated with cancer including cancer cell growth, cancer initiation, cancer migration, cancer cell adhesion, invasion, chemoresistance, and metastasis.
- diseases associated with inflammation and autoimmunity and related inflammatory diseases, including disease associated with inappropriate immune cell activation or migration such as graft versus host disease (GVHD).
- diseases associated with lymphatic development, lymphangiogenesis, and lymphatic damage including edema, lymphedema, secondary lymphedema, inappropriate fat absorption and deposition, excess fat deposition, and vascular permeability.
- COPD chronic obstructive pulmonary disorder
- ANCA antineutrophil cytoplasmic antibody
- ANCA antineutrophil cytoplasmic antibody-associated systemic vasculitis
- systemic lupus erythematosus rheumatoid arthritis
- inflammasome-related disease(s) ryoderma gangrenosum
- skin-related neutrophil-mediated disease(s) such as pyoderma gangrenosum.
- Additional examples include diseases associated with granulomatous inflammatory diseases including sarcoidosis and granulomas, and fibrotic diseases including endometriosis, fibrosis, endothelial to mesenchymal transition (EMT), and wound healing, among others. Also included are diseases associated with inappropriate smooth muscle contractility, smooth muscle compensation and decompensation, vascular smooth muscle cell migration and/or adhesion, and diseases associated with inappropriate autophagy, phagocytosis, and efferocytosis. Also included are diseases associated with inappropriate migratory cell movement, as described herein. Additional examples include neuronal diseases, including diseases associated with peripheral nervous system remodeling and pain perception. Also included are diseases associated with bone development and/or bone remodeling. Typically, the term "inappropriate” refers to an activity or characteristic that associates with or causes a pathology or disease state.
- reference sequence refers generally to a nucleic acid coding sequence, or amino acid sequence, to which another sequence is being compared. All polypeptide and polynucleotide sequences described herein are included as references sequences, including those described by name and those described in the Tables and the Sequence Listing.
- Certain embodiments include biologically active "variants” and “fragments” of the polypeptides (e.g., antibodies) described herein, and the polynucleotides that encode the same. "Variants” contain one or more substitutions, additions, deletions, and/or insertions relative to a reference polypeptide or polynucleotide (see, e.g., the Tables and the Sequence Listing).
- a variant polypeptide or polynucleotide comprises an amino acid or nucleotide sequence with at least about 50%, 55%, 60%, 65%, 70%, 75%, 80%, 85%, 90%, 91%, 92%, 93%, 94%, 95%, 96%, 97%, 98% , 99% or more sequence identity or similarity or homology to a reference sequence, as described herein, and substantially retains the activity of that reference sequence. Also included are sequences that consist of or differ from a reference sequences by the addition, deletion, insertion, or substitution of 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 30, 40, 50, 60,70, 80, 90, 100, 110,
- additions or deletions include C-terminal and/or N-terminal additions and/or deletions.
- sequence identity or, for example, comprising a “sequence 50% identical to,” as used herein, refer to the extent that sequences are identical on a nucleotide-by-nucleotide basis or an amino acid-by-amino acid basis over a window of comparison.
- a "percentage of sequence identity” may be calculated by comparing two optimally aligned sequences over the window of comparison, determining the number of positions at which the identical nucleic acid base (e.g., A, T, C, G, I) or the identical amino acid residue (e.g., Ala, Pro, Ser, Thr, Gly, Val, Leu, lie, Phe, Tyr, Trp, Lys, Arg, His, Asp, Glu, Asn, Gin, Cys and Met) occurs in both sequences to yield the number of matched positions, dividing the number of matched positions by the total number of positions in the window of comparison (i.e., the window size), and multiplying the result by 100 to yield the percentage of sequence identity.
- the identical nucleic acid base e.g., A, T, C, G, I
- the identical amino acid residue e.g., Ala, Pro, Ser, Thr, Gly, Val, Leu, lie, Phe, Tyr, Trp, Lys, Arg,
- Optimal alignment of sequences for aligning a comparison window may be conducted by computerized implementations of algorithms (GAP, BESTFIT, FAST A, and TFASTA in the Wisconsin Genetics Software Package Release 7.0, Genetics Computer Group, 575 Science Drive Madison, Wis., USA) or by inspection and the best alignment (i.e., resulting in the highest percentage homology over the comparison window) generated by any of the various methods selected.
- GAP Garnier et al., Nucl. Acids Res. 25:3389, 1997.
- solubility refers to the property of an agent (e.g., antibody) provided herein to dissolve in a liquid solvent and form a homogeneous solution. Solubility is typically expressed as a concentration, either by mass of solute per unit volume of solvent (g of solute per kg of solvent, g per dL (100 mL), mg/ml, etc.), molarity, molality, mole fraction or other similar descriptions of concentration.
- the maximum equilibrium amount of solute that can dissolve per amount of solvent is the solubility of that solute in that solvent under the specified conditions, including temperature, pressure, pH, and the nature of the solvent.
- solubility is measured at physiological pH, or other pH, for example, at pH 5.0, pH 6.0, pH 7.0, pH 7.4, pH 7.6, pH 7.8, or pH 8.0 (e.g., about pH 5-8).
- solubility is measured in water or a physiological buffer such as PBS or NaCI (with or without NaPC ).
- solubility is measured at relatively lower pH (e.g., pH 6.0) and relatively higher salt (e.g., 500mM NaCI and lOmM NaP0 4 ).
- solubility is measured in a biological fluid (solvent) such as blood or serum.
- a biological fluid such as blood or serum.
- the temperature can be about room temperature (e.g., about 20, 21, 22,
- an agent has a solubility of at least about 0.1, 0.2, 0.3, 0.4, 0.5, 0.6, 0.7, 0.8, 0.9, 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 25, 30, 40, 50, 60, 70, 80, 90 or 100 mg/ml at room temperature or at 37°C.
- a "subject” or a “subject in need thereof” or a “patient” or a “patient in need thereof” includes a mammalian subject such as a human subject.
- substantially or “essentially” means nearly totally or completely, for instance, 95%, 96%, 97%, 98%, 99% or greater of some given quantity.
- Statistical significance it is meant that the result was unlikely to have occurred by chance.
- Statistical significance can be determined by any method known in the art. Commonly used measures of significance include the p-value, which is the frequency or probability with which the observed event would occur, if the null hypothesis were true. If the obtained p-value is smaller than the significance level, then the null hypothesis is rejected. In simple cases, the significance level is defined at a p-value of 0.05 or less.
- “Therapeutic response” refers to improvement of symptoms (whether or not sustained) based on administration of one or more therapeutic agents.
- the terms “therapeutically effective amount”, “therapeutic dose,” “prophylactically effective amount,” or “diagnostically effective amount” is the amount of an agent (e.g., anti-NRP2 antibody, immunotherapy agent) needed to elicit the desired biological response following administration.
- treatment of a subject (e.g., a mammal, such as a human) or a cell is any type of intervention used in an attempt to alter the natural course of the individual or cell. Treatment includes, but is not limited to, administration of a pharmaceutical composition, and may be performed either prophylactically or subsequent to the initiation of a pathologic event or contact with an etiologic agent.
- prophylactic treatments which can be directed to reducing the rate of progression of the disease or condition being treated, delaying the onset of that disease or condition, or reducing the severity of its onset.
- Treatment or “prophylaxis” does not necessarily indicate complete eradication, cure, or prevention of the disease or condition, or associated symptoms thereof.
- wild-type refers to a gene or gene product (e.g., a polypeptide) that is most frequently observed in a population and is thus arbitrarily designed the "normal” or “wild-type” form of the gene.
- Certain embodiments include antibodies, and antigen-binding fragments thereof, which specifically bind to a human neuropilin 2 (NRP2) polypeptide.
- the at least one antibody or antigen-binding fragment thereof modulates (e.g., interferes with) binding of the human NRP2 polypeptide to at least one NRP2 ligand, such as a human histidyl-tRNA synthetase (HRS) polypeptide or other NRP2 ligand.
- NRP2 human neuropilin 2
- the at least one antibody or antigen-binding fragment thereof modulates (e.g., interferes with) binding of the human NRP2 polypeptide to at least one NRP2 ligand, such as a human histidyl-tRNA synthetase (HRS) polypeptide or other NRP2 ligand.
- HRS human histidyl-tRNA synthetase
- an antibody or antigen-binding fragment thereof is characterized by or comprises a heavy chain variable region (VH) sequence that comprises complementary determining region VHCDRI, VHCDR2, and VHCDR3 sequences, and a light chain variable region (VL) sequence that comprises complementary determining region VLCDRI, V CDR2, and V CDR3 sequences.
- VH heavy chain variable region
- VL light chain variable region
- Exemplary V H , V H CDR1, V H CDR2, V H CDR3, V L , V L CDR1, V L CDR2, and V L CDR3 sequences are provided in Table Al, Table A2, and Table A3 below.
- an antibody or antigen-binding fragment thereof comprises a heavy chain variable region (V H ) sequence that comprises complementary determining region V H CDR1, V H CDR2, and V H CDR3 sequences selected from Table A1 and variants thereof which specifically bind to a human NRP2 polypeptide (selected, for example, from Table Nl); and a light chain variable region (V L ) sequence that comprises complementary determining region V L CDRI, V L CDR2, and V L CDR3 sequences selected from Table A1 and variants thereof which specifically bind to the human NRP2 polypeptide (selected, for example, from Table Nl).
- V H heavy chain variable region
- V L light chain variable region
- the CDR sequences are as follows: the V H CDRI, V H CDR2, and V H CDR3 sequences comprise SEQ ID NOs: 1-3, respectively, and the V L CDRI, V L CDR2, and V L CDR3 sequences comprise SEQ ID NOs: 4-6, respectively, including variants thereof; the V H CDRI, V H CDR2, and V H CDR3 sequences comprise SEQ ID NOs: 7-9, respectively, and the V L CDRI, V L CDR2, and V L CDR3 sequences comprise SEQ ID NOs: 10-12, respectively, including variants thereof; the V H CDR1, V H CDR2, and V H CDR3 sequences comprise SEQ ID NOs: 13-15, respectively, and the V L CDR1, V L CDR2, and V L CDR3 sequences comprise SEQ ID NOs: 16-18, respectively, including variants thereof; the V H CDRI, V H CDR2, and V H CDR3 sequences comprise SEQ ID NOs: 19-21, respectively, and the V L CDRI
- variants thereof including affinity matured variants, which bind to human NRP2, for example, variants having 1, 2, 3, 4, 5, or 6 alterations in one or more of the CDR regions, for example, one or more the V H CDRI, V H CDR2, V H CDR3, V L CDRI, V L CDR2, and/or V L CDR3 sequences described herein.
- alterations include amino acid substitutions, additions, and deletions.
- the V H sequence is at least 80, 85, 90, 95, 97, 98, 99, or 100% identical to a sequence selected from Table A2, including, for example, wherein the V H sequence has 1, 2, 3, 4, or 5 alterations in one or more framework regions.
- the V L sequence is at least 80, 85, 90, 95, 97, 98, 99, or 100% identical to a sequence selected from Table A2, including, for example, wherein the V L sequence has 1, 2, 3, 4, or 5 alterations in one or more framework regions.
- the V H and V L sequences of an antibody or antigen-binding fragment are as follows: the V H sequence comprises SEQ ID NO: 43, and the V L sequence comprises SEQ ID NO: 44; the V H sequence comprises SEQ ID NO: 45, and the V L sequence comprises SEQ ID NO: 46; the V H sequence comprises SEQ ID NO: 47, and the V L sequence comprises SEQ ID NO: 48; the V H sequence comprises SEQ ID NO: 49, and the V L sequence comprises SEQ ID NO: 50; the V H sequence comprises SEQ ID NO: 51, and the V L sequence comprises SEQ ID NO: 52; the V H sequence comprises SEQ ID NO: 53, and the V L sequence comprises SEQ ID NO: 54; the V H sequence comprises SEQ ID NO: 55, and the V L sequence comprises SEQ ID NO: 56; the V H sequence comprises SEQ ID NO: 69, and the V L sequence comprises SEQ ID NO: 70; the V H sequence comprises SEQ ID NO: 71, and the V L sequence comprises SEQ ID NO: 72; or
- variants thereof for example, variants having 1, 2, 3, 4, or 5 alterations in one or more framework regions.
- exemplary "alterations” include amino acid substitutions, additions, and deletions.
- Table A3 summarizes exemplary redundant antibody CDRs, including exemplary consensus CDR sequences, and provides amino acid code for the same.
- the at least one anti-NRP2 antibody or antigen-binding fragment thereof comprises a CDR sequence, for example, a CDR1 consensus sequence, from Table A3.
- Neuropilin-2 is a cell surface receptor protein that modulates a broad range of cellular functions through its roles as an essential cell surface receptor and co-receptor for a variety of ligands (see, e.g., Guo and Vander Kooi, J. Cell. Biol. 290 No 49: 29120-29126, 2015).
- EMT epithelial to mesenchymal transition
- Neuropilin-2 expression promotes lymphangiogenesis (see, e.g., Doci et al., Cancer Res. 75:2937-2948, 2015) single nucleotide polymorphisms (SNPs) in NRP2 are associated with lymphedema (see, e.g., Miaskowski et al., PLoS ONE 8(4) e60164, 2013).
- NRP2 also regulates smooth muscle contractility (see, e.g., Bielenberg et al., Amer. J. Path. 181:548-559, 2012), regulates autophagy, for example, in cancer (see, e.g., Stanton et al., Cancer Res.
- Neuropilins are also multifunctional co-receptors involved in tumor initiation, growth, metastasis and immunity (see, e.g., Prud'homme et al., Oncotarget 3:921-939, 2012).
- Neuropilin-2 is expressed in various cells of the immune system, including lymphoid cells such as B and T cells, and myeloid cells such as basophils, eosinophil, monocytes, dendritic cells, neutrophils, and macrophages, including tissue-specific macrophages, for example, alveolar macrophages. It is also expressed in endothelial and epithelial cells in the lung and other tissues, and in muscle cells [see, e.g., Bielenberg et al., Amer. J. Path. 181:548-559, 2012; Aung, et al., PLoS ONE 11(2) e0147358, 2016; Schellenburg et al., Mol. Imm 90:239-244, 2017; and Wild et al., Int. J. Exp. Path. 93:81-103, 2012).
- lymphoid cells such as B and T cells
- myeloid cells such as basophils, eosinophil,
- Neuropilin-2 also plays a key role in endosome development, for example, by regulating late endosomal maturation, an important aspect of phagocytosis and efferocytosis, which respectively contribute to clearance of infections and apoptotic cells (See, e.g., Diaz-Vera et al., J. Cell. Sci. 130:697-711, 2017; Dutta et al., Cancer Res. 76:418-428, 2016).
- Neuropilin-2 is known to be a key player in the pathophysiology of many diseases (e.g., "NRP2-associated diseases") and interacts with a broad array of soluble ligands including semaphorin 3F, VEGF-C and D, and TGF-beta (see, for example, Table N2 and Table N3), and an array of cellular receptors and co-factors (see, for example, Figures 1A-1B and Figure 2).
- NRP2 is also polysialated on dendritic cells, and actively interacts with the chemokine CCL21 to mediate immune cell migration, and for which single nucleotide polymorphisms associated with ILD and RA have been described (see, e.g., Rey-Gallardo et al., Glycobiology 20:1139-1146, 2010; Stahl et al., Nat. Genet. 42:508-514, 2013; and Miller et al., Arthritis Rheum. 65:3239-3247).
- NRP2 soluble, circulating forms of NRP-2 are known (see, e.g., Parker et al., Structure 23(4) 677-687, 2015), and internal studies have confirmed the existence of circulating complexes of FIRS polypeptides and NRP-2 polypeptides in circulation. Accordingly, given the central role played by NRP2 in pathophysiology in a broad range of diseases, it is evident that interactions between NRP2 and NRP2 ligand(s) (for example, NRP2 ligands from Table N2 and Table N3), and the modulation of those interactions with antibodies against NRP2 to selectively change the corresponding biological activities, provides broad potential for the treatment of diseases, including NRP2 associated diseases.
- NRP2 ligand(s) for example, NRP2 ligands from Table N2 and Table N3
- NRP2 is a single transmembrane receptor with a predominant extracellular region containing two CUB domains (al/a2 combined domain), two Factor V/VIII homology domains (bl/b2 combined domain), a MAM domain (c domain) (see Figures 1A-1B), and a short juxtamembrane region that connects the c domain to the transmembrane domain (which traverses the plasm membrane).
- the ala2 combined domain interacts with sema region of the semaphorins, and the bl domain interacts with the semaphorin PSI and Ig-like domains.
- NRP2 has a higher affinity for SEMA3F and 3G; in contrast, SEMAs 3A, 3B and 3E preferentially interact with NRP1. Both NRP1 and NRP2 have similar affinity for SEMA 3C.
- the blb2 combined domain interacts with several growth factors containing heparin-binding domains, including VEGF C & D, placenta growth factor (PIGF)-2, fibroblast growth factor (FGF), galectin, hepatocyte growth factor (FIGF), platelet derived growth factor (PDGF), and transforming growth factor (TGF)-beta (see, for example, Prud'homme et al., Oncotarget. 3:921-939, 2012).
- PIGF placenta growth factor
- FGF fibroblast growth factor
- FIGF hepatocyte growth factor
- PDGF platelet derived growth factor
- TGF transforming growth factor
- NRP2 also interacts with various growth factor-specific receptors, and interactions with these receptors occur independently of binding to SEMAs.
- integrins and growth factor receptors like VEGF receptor, TGF-beta receptor, c-Met, EGFR, FGFR, PDGFR, have been shown to interact with NRPs and in general appear to increase the affinity of each ligand for its receptor and to modulate down stream signaling.
- the c domain (Mam) domain does not appear to be directly required for ligand binding, but may impact ligand specificity, receptor signaling, and NRP2 dimerization.
- the juxtamembrane region differs significantly between the NRP2a and NRP2b isoforms, and may also impact ligand specificity, dimerization, and signaling. Accordingly, anti-NRP2 antibodies and antigen-binding fragments thereof that bind to the al and/or a2 domains of NRP2 have the potential to selectively modulate semaphorin binding.
- anti-NRP2 antibodies and antigen-binding fragments thereof that bind to the bl domain have the potential to modulating both semaphorin and VEGF and growth factor binding
- anti- NRP2 antibodies that bind to the b2 domain have the potential to selectively modulate VEGF and growth factor binding
- Antibodies and antigen-binding fragments thereof that bind to the c domain might not directly impact NRP2 ligand binding, but have the potential to modulate NRP2 downstream signaling, for example, by modulating (e.g., promoting or enhancing) NRP2 receptor dimerization.
- Anti-NRP2 antibodies and antigen binding fragments thereof that promote NRP2 receptor homodimerization could modulate NRP2 receptor activity, and provide agonistic or antagonistic antibodies depending on the nature of the binding site. Such antibodies and antigen binding fragments thereof could modulate (e.g., enhance) the activities of NRP2 ligands, even if they do not directly modulate ligand binding. Additional diversity in the functional effects of specific anti-NRP2 antibodies may be expected based on their binding mode, and as a result of steric effects, which may indirectly impact ligand binding.
- NRP2 can form homodimers as well as heterodimers, and is heavily glycosylated. NRP2 has different splice variants which are between about 551 and 926 amino acids long. Two major variants for NRP2 are categorized as NRP2a and NRP2b. These differ in their intracellular C terminal part ( Figures 1A-1B) in which for NRP2a, the c-terminal domain comprises 42 amino acids and a PDZ- binding domain with the C-terminal SEA amino acid sequence. By contrast, NRP2b comprises a 46 amino acid C terminal domain which shares about 11% sequence homolog with the intracellular, juxtamembrane, and transmembrane sequences of NRP2a.
- NRP2a 5 additional amino acids
- NRP2b 5 additional amino acids
- NRP2b 5 additional amino acids
- NRP2a(17) or variant 1
- NRP2a(22) or variant 2
- NRP2b(0) or variant 4
- NRP2b(5) or variant 5
- sNRP2b or variant 6
- Exemplary NRP2 polypeptide sequences are provided in Table N1 below, including the mature (after cleavage of the N-terminal signal peptide) and precursor forms of the various isoforms of NRP2.
- the at least one antibody or antigen-binding fragment thereof specifically binds to a full-length human NRP2 polypeptide or a human NRP2 polypeptide selected from Table Nl.
- the antibody or antigen-binding fragment thereof binds to the human NRP2 polypeptide with an affinity of about 10 pM to about 500 pM or to about 50 nM, or about, at least about, or no more than about 10, 20, 30, 40, 50, 60, 70, 80, 90, 100, 110, 120, 130, 140, 150, 160, 170, 180, 190, 200, 300, 400, 500, 600, 700, 800, 900 pM, 1 nM, 10 nM, 25 nM, or 50 nM, or optionally with an affinity that ranges from about 10 pM to about 500 pM, about 10 pM to about 400 pM, about 10 pM to about 300 pM, about 10 pM to about 200 pM, about 10 pM to
- the at least one antibody or antigen-binding fragment thereof that specifically binds to at least one epitope in at least one neuropilin domain include one or more of the neuropilin al domain, neuropilin a2 domain, neuropilin bl domain, neuropilin b2 domain, neuropilin c domain, neuropilin al/a2 combined domain, neuropilin bl/b2 combined domain, neuropilin a2/bl combined domain, neuropilin b2/c combined domain, neuropilin a2/bl/b2 combined domain, neuropilin a2/bl/b2/c combined domain, neuropilin al/a2/bl combined domain, neuropilin al/a2/bl/b2 combined domain, neuropilin al/a2/bl/b2 combined domain, neuropilin al/a2/bl/b2/c combined domain, al/a2/bl/b2/c/juxtamembrane combined domain, and the neuropilin bl/
- the at least one antibody or antigen-binding fragment thereof specifically binds to at least one epitope in the neuropilin bl domain, the neuropilin b2 domain, and/or the neuropilin bl/b2 combined domain (see Table Nl).
- the antibody or antigen-binding fragment thereof binds to the at least one domain (or at least one epitope therein) with an affinity of about 10 pM to about 500 pM or to about 50 nM, or about, at least about, or no more than about 10, 20, 30, 40, 50, 60, 70, 80, 90, 100, 110, 120, 130, 140, 150, 160, 170, 180, 190, 200, 300, 400, 500, 600, 700, 800, 900 pM, 1 nM, 10 nM, 25 nM, or 50 nM, or optionally with an affinity that ranges from about 10 pM to about 500 pM, about 10 pM to about 400 pM, about 10 pM to about 300 pM, about 10 pM to about 200 pM, about 10 pM to about 100 pM, about 10 pM to about 50 pM, or about 20 pM to about 500 pM, about 20 pM to about 400 pM,
- the at least one antibody or antigen-binding fragment thereof specifically binds to at least one epitope in the neuropilin al domain, the neuropilin a2 domain, and/or the neuropilin ala2 combined domain, including adjacent linker regions, for example, at about residues (neuropilin al domain) 20-148, 30-141, 40-141, 50-141, 60-141, 70-141, 80-141, 90- 141, 100-141, 110-141, 120-141, 130-141; 20-130, 20-120, 20-110, 20-100, 20-90, 20-80, 20-70, 20- 60, 20-50, 20-40, or 20-30 as defined by a human NRP2 precursor sequence (see Table Nl); or, for example, at about residues (neuropilin a2 domain) 142-280, 150-265, 160-265, 170-265, 180-265, 190-265, 200-265, 210-265, 220-265, 230-265, 240
- the at least one antibody or antigen-binding fragment thereof specifically binds to at least one epitope in the neuropilin bl domain, the neuropilin b2 domain, and/or the neuropilin bl/b2 combined domain, including adjacent linker regions, for example, at about residues (neuropilin bl domain) 266-426, 280-426, 290-426, 299-420, 300-426, 310-426, 320- 426, 330-426, 340-426, 350-426, 360-426, 370-426, 380-426, 390-426, 400-426, 410-426, 420-426, 280-420, 280-410, 280-400, 280-390, 280-380, 280-370, 280-360, 280-350, 280-340, 280-330, 280- 320, 280-310, 280-300, or 280-290 as defined by a human NRP2 precursor sequence (see
- the at least one antibody or antigen-binding fragment thereof specifically binds to at least one epitope in the neuropilin a2/bl combined domain and/or the neuropilin b2c combined domain, including adjacent linker regions, for example, at about residues (neuropilin a2bl combined domain) 149-437, 159-426, 169-426, 179-426, 189-426, 199-426, 209- 426, 219-426, 229-426,239-426, 249-426, 259-426, 269-426, 279-426, 289-426, 299-426, 309-426, 319-426, 329-426, 339-426, 349-426, 359-426, 369-426, 379-426, 389-426, 399-426, 409-426, 419- 426, 149-436, 149-426, 149-416, 149-406, 149-396, 149-386,
- the at least one antibody or antigen-binding fragment thereof specifically binds to at least one epitope in the neuropilin c domain, including adjacent linker regions, for example, at about residues 591-794, 600-794, 610-794, 620-794, 630-794, 640-794, 650- 794, 660-794, 670-794, 680-794, 690-794, 700-794, 710-794, 720-794, 730-794, 740-794, 750-794, 760-794, 770-794, 780-794, 790-794, 591-790, 591-780, 591-770, 591-760, 591-750, 591-740, 591- 730, 591-720, 591-710, 591-700, 591-690, 591-680, 591-670, 591-660, 591-650, 591-640, 591-630, 591-620, 591-610, or 59
- the at least one antibody or antigen-binding fragment thereof specifically binds to at least one epitope in the neuropilin bl/b2/c combined domain, including adjacent linker regions, for example, at about residues 276-794, 286-794, 296-794, 306-794, 316- 794, 326-794, 336-794, 346-794, 356-794, 366-794, 376-794, 387-794, 396-794, 406-794, 416-794, 426-794, 436-794, 446-794, 456-794, 466-794, 476-794, 486-794, 496-794, 506-794, 516-794, 526- 794, 536-794, 546-794, 556-794, 566-794, 576-794, 586-794, 596-794, 606-794, 616-794, 626-794, 636-794, 646-794, 656-794, 666-794, 676-794, 686-794, 696-794, 706-794, 716-794, 72
- the at least one antibody or antigen-binding fragment thereof specifically binds to at least one epitope in the neuropilin C/juxtamembrane combined domain.
- the at least one antibody or antigen-binding fragment thereof specifically binds to at least one epitope in the neuropilin juxtamembrane domain of NRP2a (variant 1). In some embodiments, the at least one antibody or antigen-binding fragment thereof specifically binds to at least one epitope in the neuropilin juxtamembrane domain of NRP2a (variant 2). In some embodiments, the at least one antibody or antigen-binding fragment thereof specifically binds to at least one epitope in the neuropilin juxtamembrane domain of NRP2a (variant 3).
- the at least one antibody or antigen-binding fragment thereof specifically binds to at least one epitope in the neuropilin juxtamembrane domain of NRP2b (variant 4). In some embodiments, the at least one antibody or antigen-binding fragment thereof specifically binds to at least one epitope in the neuropilin juxtamembrane domain of NRP2b (variant 5).
- the at least one antibody or antigen-binding fragment thereof specifically binds to a conformational epitope composed of two or more discontinuous epitope regions. In some embodiments, the at least one antibody or antigen-binding fragment thereof specifically binds to a conformational epitope comprising or consisting of:
- the antibody or antigen-binding fragment thereof specifically binds to at least one epitope within a region of a human NRP2 polypeptide that binds to or interacts with at least one "NRP2 ligand", including any molecule that interacts with or binds reversibly to human NRP2, including any one or more variants of human NRP2.
- "NRP2 ligands” include polypeptides such as HRS polypeptides, soluble ligands, receptors (e.g., cell surface receptors), including growth factors, growth factor receptors, and others, and specific examples of NRP2 ligands are detailed herein.
- the at least one antibody or antigen binding fragment thereof modulates (e.g., antagonizes, interferes with, agonizes, enhances) binding of the human NRP2 polypeptide to at least one "NRP2 ligand".
- the at least one NRP2 ligand is an HRS polypeptide.
- an antibody or antigen-binding fragment thereof specifically binds to at least one epitope within a region of a human NRP2 polypeptide that binds to or interacts with at least one human HRS polypeptide, and thereby modulates binding of the human NRP2 polypeptide to the human HRS polypeptide.
- Exemplary HRS polypeptides are provided in Table HI below.
- the at least one NRP2 ligand is selected from Table HI
- the anti-NRP2 antibody or antigen-binding fragment thereof modulates (e.g., interferes with) binding of a human NRP2 polypeptide (for example, a human NRP2 polypeptide selected from Table Nl) to a human HRS polypeptide selected from Table HI.
- the anti-NRP2 antibody or antigen-binding fragment specifically binds to an HRS polypeptide-interacting region of the NRP2 polypeptide, and in some instances mimics one or more signaling activities of the HRS polypeptide binding to the NRP2 polypeptide, for example, as an agonist antibody.
- HRS polypeptide-interacting region includes a region or domain of a human NRP2 polypeptide that interacts with a region or domain of human HRS polypeptide, for example, at a ligand binding site for a different NRP2 ligand (examples of which are provided herein), a dimerization domain, a protein- protein interaction domain, or at a site which is allosterically sensitive within a NRP2 polypeptide to modulate the activity of the NRP2 polypeptide.
- an antibody or antigen-binding fragment thereof is a "blocking antibody", which fully or substantially inhibits the binding between a human NRP2 polypeptide (selected, for example, from Table Nl) and an NRP2 ligand such as a human HRS polypeptide (selected, for example, from Table HI) or other NRP2 ligand (for example, selected from Table N2 or Table N3).
- a "blocking antibody” inhibits about or at least about 80-100% (e.g., 80, 85, 90, 95, or 100%) of the theoretical maximal binding between the NRP2 polypeptide and the NRP2 ligand (for example, HRS polypeptide) after pre-incubation of the "blocking antibody” with the NRP2 polypeptide in a substantially stoichiometrically equivalent amount.
- a "stoichiometrically equivalent amount” refers to a situation where the number of moles of one substance (e.g., anti-NRP2 antibody) is equivalent or substantially equivalent to the number of moles at least one other substance (e.g., NRP2 polypeptide) in a given equation or reaction.
- an antibody or antigen-binding fragment thereof is a "partial- blocking antibody", which at least partially but not fully inhibits the binding between a human NRP2 polypeptide (selected, for example, from Table Nl) and an NRP2 ligand such as a human HRS polypeptide (selected, for example, from Table HI) or other NRP2 ligand (for example, selected from Table N2 or Table N3).
- a human NRP2 polypeptide selected, for example, from Table Nl
- an NRP2 ligand such as a human HRS polypeptide (selected, for example, from Table HI) or other NRP2 ligand (for example, selected from Table N2 or Table N3).
- a "partial-blocking antibody” inhibits about or at least about 20-80% (e.g., 20, 25, 30, 35, 40, 45, 50, 55, 60, 65, 70, 75, or 80%) of the theoretical maximal binding between the NRP2 polypeptide and the NRP2 ligand (for example, HRS polypeptide) after pre-incubation of the "partial-blocking antibody" with the NRP2 polypeptide in a stoichiometric amount.
- the NRP2 polypeptide for example, HRS polypeptide
- the at least one antibody or antigen-binding fragment thereof specifically inhibits or otherwise reduces the binding between a human NRP2 polypeptide and a HRS polypeptide splice variant selected from Table HI, for example, a HRS splice variant selected from one or more of HisRS N1 , HisRS N2 , HisRS N3 , HisRS N4 (SV9), HisRS N5 , HisRS cl , HisRS C2 , HisRS C3 , HisRS C4 , HisRS C5 , HisRS ce , HisRS C7 , HisRS C8 (SVll), and HisRS C9 (SV14).
- NRP2 interacts with multiple NRP2 ligands other than HRS, which mediate downstream signaling events. Additional examples of NRP2 ligands are provided in Table N2 and Table N3 below.
- the at least one NRP2 ligand is selected from Table N2 and/or Table N3.
- the at least one NRP2 ligand is a VEGF (vascular endothelial growth factor) ligand selected from VEGF-A145, VEGF-A165, VEGF-C, VEGF-D, and PIGF-2.
- VEGF- VEGFR2/3-NRP2 interactions are associated with promoting cell migration, cell growth, cell survival, and cell attachment, and also with lymphangiogenesis, increasing vascular permeability, activating integrin signaling, promoting vesicular trafficking and internalization, and slowing cellular differentiation.
- anti-NRP2 antibodies which modulate VEGF related NRP2 ligands would be expected find utility in modulating one or more of these pathways.
- the at least one NRP2 ligand is a semaphorin selected from one or more of SEMA-3B, SEMA-3C, SEMA-3D, SEMA-3F, and SEMA-3B, or a plexin receptor selected from one or more of plexins Al, A2, A3, A4, and Dl.
- SEMAs typically antagonize the effects of VEGF-C, through there is a close dynamic interplay between VEGF and Serna signaling pathways.
- SEMAs typically function in the immune system to control cell movement, cell migration, cell-cell communication, and cell activation.
- SEMA Plexin-NRP2 interactions are associated with inhibiting cell migration, inhibiting cell growth, promoting apoptosis, inhibiting cell attachment, inhibiting integrin signaling, promoting cellular differentiation, inhibiting lymphangiogenesis, reducing vascular permeability, promoting microtubule destabilization, mediating the collapse of actin cytoskeleton & cell contraction including growth cone collapse and actomyosin contraction, and preventing neuronal cell spreading and inhibiting axon outgrowth.
- anti-NRP2 antibodies which modulate SEMA-related NRP2 ligands would be expected find utility in modulating one or more of these pathways.
- the at least one NRP2 ligand is an integrin selected from one or more of a ⁇ /b1, anb3, anb5, a ⁇ /b6, a ⁇ /b8, abb ⁇ and a6b4.
- I ntegrin-N RP2 interactions are generally associated with increased cell adhesion, cell growth, cancer growth and invasiveness. Accordingly anti-NRP2 antibodies which modulate integrin related NRP2 ligands would be expected find utility in modulating one or more of these pathways.
- the at least one NRP2 ligand is selected from T ⁇ RbI, T ⁇ Rb2, T ⁇ Rb , and their corresponding T ⁇ Rb receptors.
- TGF-b signaling is strongly involved in the regulation of EMT in cancer, and also in fibrosis development (see, for example, Gemmill et al., Sci. Signal. 10 eaag0528, 2017).
- NRP2b expression is preferentially upregulated by TGF-b signaling in abnormal lungs, and shows little or no expression in normal lung. NRP2b expression enhances migration, invasion, metastasis, chemoresistance, and tumorsphere formation, and also enhances acquired EGFR inhibitor resistance associated with EMT in cancer cells.
- anti-NRP2 antibodies which modulate TGF-b related NRP2 ligands would be expected find utility in modulating one or more of these pathways, and find utility in the treatment of cancer chemoresistance.
- an anti-NRP2 antibody or antigen-binding fragment thereof modulates binding/signaling activity between an NRP2 polypeptide and at least one of the NRP2 ligands from Table N2 and/or Table N3, for example, by specifically binding to an NRP2 ligand-interacting region of the NRP2 polypeptide.
- the at least one antibody or antigen-binding fragment thereof binds selectively to the NRP2a isoform (e.g., variants 1, 2, and/or 3 of Table Nl) of NRP2, and does not substantially bind to the NRP2b isoform (e.g., variants 4 and/or 5 of Table Nl) of NRP2. In some embodiments, the at least one antibody or antigen-binding fragment thereof binds selectively to the NRP2b isoform (e.g., variants 4 and/or 5 of Table Nl), and does not substantially bind to the NRP2a isoform (e.g., variants 1, 2, and/or 3 of Table Nl) of NRP2.
- the at least one antibody or antigen-binding fragment thereof antagonizes the binding/signaling activity between the NRP2 polypeptide and the at least one NRP2 ligand.
- the anti-NRP2 antibody antagonizes or reduces the theoretical maximal binding/signaling between the NRP2 polypeptide and the NRP2 ligand by about or at least about 20-100% (e.g., about 20, 25, 30, 35, 40, 45, 50, 55, 60, 65, 70, 75, 80, 90, or 100%) after pre-incubation of the anti-NRP2 antibody with the NRP2 polypeptide/ligand in a substantially stoichiometrically equivalent amount.
- the at least one antibody or antigen-binding fragment thereof reduces or inhibits the dimerization between two NRP2 polypeptides.
- the anti-NRP2 antibody antagonizes or reduces the theoretical maximal dimerization between two NRP2 polypeptides by about or at least about 20-100% (e.g., about 20, 25, 30, 35, 40, 45, 50, 55, 60, 65,
- the at least one antibody or antigen-binding fragment thereof agonizes or enhances the dimerization between two NRP2 polypeptides.
- the anti-NRP2 antibody agonizes or enhances the basal dimerization state of two NRP2 polypeptides by about or at least about 20%-500% (e.g., about 20, 30, 40, 50, 60, 70, 80, 90, 100, 200, 300, 400 or 500%) after pre-incubation of the anti-NRP2 antibody with the NRP2 polypeptides in a substantially stoichiometrically equivalent amount.
- the at least one antibody or antigen-binding fragment thereof agonizes or enhances the binding/signaling activity between the NRP2 polypeptide and the at least one NRP2 ligand.
- the anti-NRP2 antibody agonizes or enhances the theoretical maximal binding/signaling activity between the NRP2 polypeptide and the at least one NRP2 ligand by about or at least about 20%-500% (e.g., about 20, 30, 40, 50, 60, 70, 80, 90, 100, 200, 300, 400 or 500%) after pre-incubation of the anti-NRP2 antibody with the NRP2 polypeptide in a substantially stoichiometrically equivalent amount.
- the at least one antibody or antigen-binding fragment thereof selectively modulates the binding and/or signaling of semaphorins to, or via, the NRP2 polypeptide.
- such antibodies do not substantially block the interaction of VEGF-C or related NRP2 ligands.
- such antibodies are agonistic antibodies with respect to semaphorin signaling.
- such antibodies are antagonistic antibodies with respect to semaphorin signaling.
- the at least one antibody or antigen-binding fragment thereof selectively modulates the binding and/or signaling of VEGF-C or related NRP2 ligands to, or via, the NRP2 polypeptide.
- such antibodies do not substantially block the interaction of semaphorins.
- such antibodies selectively modulate both the binding of VEGF- C or related NRP2 ligands and semaphorins to the NRP2 polypeptide.
- such antibodies are agonistic antibodies with respect to VEGF-C signaling.
- such antibodies are antagonistic antibodies with respect to VEGF-C signaling.
- the at least one antibody or antigen-binding fragment thereof selectively modulates the binding and/or signaling of integrins or related NRP2 ligands to the NRP2 polypeptide. In some embodiments, the at least one antibody or antigen-binding fragment thereof selectively modulates the binding and/or signaling of TGF 1, TGF 2, TGF 3, or their corresponding TGF receptors to the NRP2 polypeptide.
- the at least one antibody or antigen-binding fragment thereof selectively modulates the binding and/or signaling of fibroblast growth factor (FGF), galectin, hepatocyte growth factor (FIGF), platelet derived growth factor, and/or their corresponding receptors to the NRP2 polypeptide.
- FGF fibroblast growth factor
- FIGF hepatocyte growth factor
- NRP2 polypeptide fibroblast growth factor
- the at least one antibody or antigen-binding fragment thereof antagonizes the binding/signaling activity between the NRP2 polypeptide and a plexin receptor and/or a semaphorin without substantially modulating the binding/signaling activity between the NRP2 polypeptide and VEGFR2, VEGFR3, and/or VEGF-C.
- the at least one antibody or antigen-binding fragment thereof antagonizes the binding/signaling activity between the NRP2 polypeptide and a plexin receptor and/or semaphorin without substantially modulating the binding/signaling activity between the NRP2 polypeptide and a FIRS polypeptide.
- the at least one antibody or antigen-binding fragment thereof antagonizes the binding/signaling activity between the NRP2 polypeptide and a plexin receptor and/or a semaphorin without substantially modulating the binding/signaling activity between the NRP2 polypeptide and a FIRS polypeptide, and without substantially modulating the binding/signaling activity between the NRP2 polypeptide and VEGFR2, VEGFR3, and/or VEGF-C.
- the at least one antibody or antigen-binding fragment thereof antagonizes the binding/signaling activity between the NRP2 polypeptide and VEGFR2 and/or VEGFR3 without substantially modulating the binding/signaling activity between the NRP2 polypeptide and a plexin receptor and/or a semaphorin.
- the at least one antibody or antigen-binding fragment thereof antagonizes the binding/signaling activity between the NRP2 polypeptide and VEGFR2, VEGFR3, and/or VEGF-C without substantially modulating the binding/signaling activity between the NRP2 polypeptide and a FIRS polypeptide.
- the at least one antibody or antigen-binding fragment thereof antagonizes the binding/signaling activity between the NRP2 polypeptide and a plexin receptor without substantially modulating the ligand binding of semaphorin 3 to NRP2.
- the plexin receptor is selected from plexin Al, A2, A3, A4, and Dl.
- the semaphorin is selected from semaphorin 3B, 3C, 3D, 3F, and 3G.
- the at least one antibody or antigen-binding fragment thereof specifically binds to an epitope of at least 5 amino acids within the human NRP2 a2 domain, wherein the at least one antibody or antigen-binding fragment thereof selectively inhibits receptor dimerization between NRP2 and plexin A1 without substantially inhibiting dimerization between NRP2 and FLT4 (VEGFR3).
- the at least one antibody or antigen-binding fragment thereof specifically binds to an epitope within amino acids 232-242 of a human NRP2 precursor (see Table Nl).
- the at least one antibody or antigen-binding fragment thereof specifically binds to an epitope of at least 5 amino acids within the human NRP2 bl domain, wherein the at least one antibody or antigen-binding fragment thereof selectively inhibits receptor dimerization between NRP2 and FLT4 (VEGFR3) without substantially inhibiting dimerization between NRP2 and plexin Al.
- the at least one antibody or antigen-binding fragment thereof specifically binds to an epitope of at least 5 amino acids within the human NRP2 b2 domain, wherein the at least one antibody or antigen-binding fragment thereof inhibits receptor dimerization between NRP2 and FLT4 (VEGFR3) and inhibits dimerization between NRP2 and plexin Al.
- the at least one antibody or antigen-binding fragment thereof specifically binds to an epitope of at least 5 amino acids within the human NRP2 c domain, wherein the at least one antibody or antigen-binding fragment thereof inhibits receptor dimerization between NRP2 and plexin Al and partially inhibits dimerization between NRP2 and FLT4 (VEGFR3).
- the at least one antibody or antigen-binding fragment thereof has an affinity (Kd or EC50) for each of (i) a human NRP2 polypeptide and (ii) the corresponding region of a cynomolgus monkey NRP2 polypeptide (see, for example, UniProt G7PL91), wherein the affinity for (i) and (ii) is within the range of about 20 pM to about 200 pM, about 30 pM to about 300 pM, about 40 pM to about 400 pM, about 50 pM to about 500 pM, about 60 pM to about 600 pM, about 70 pM to about 700 pM, about 80 pM to about 800 pM, about 90 pM to about 900 pM, about 100 pM to about 1 nM, about 0.4 to about 1.2 nM, about 0.9 to about 5.5 nM, about 0.9 to about 5 nM, or about 1 nM to about 10 n
- the at least one antibody or antigen-binding fragment thereof has an affinity (Kd or EC50) for each of (i) a human NRP2 polypeptide and (ii) the corresponding region of a murine NRP2 polypeptide, wherein the affinity for (i) and (ii) is within the range of about 20 pM to about 200 pM, about 30 pM to about 300 pM, about 40 pM to about 400 pM, about 50 pM to about 500 pM, about 60 pM to about 600 pM, about 70 pM to about 700 pM, about 80 pM to about 800 pM, about 90 pM to about 900 pM, about 100 pM to about 1 nM, or about 1 nM to about 10 nM.
- affinity Kd or EC50
- the at least one antibody or antigen-binding fragment thereof binds selectively to a human NRP2 polypeptide (see Table Nl) relative to a murine NRP2 polypeptide, for instance, where its affinity for a human NRP2 polypeptide is significantly stronger than its affinity for a murine NRP2 polypeptide, for example, by about or at least about 2, 5, 10, 20, 30, 40, 50, 100, 500, or 1000-fold or more.
- the at least one antibody or antigen-binding fragment thereof binds selectively to a human NRP2 polypeptide and does not substantially bind to a murine NRP2 polypeptide.
- Certain exemplary murine NRP2 polypeptides include the Mus musculus NRP2 polypeptide (see, for example, UniProt 035375).
- the binding interactions between a human NRP2 polypeptide and an NRP2 ligand can be detected and quantified using a variety of routine methods, including biacore assays (for example, with appropriately tagged soluble reagents, bound to a sensor chip), FACS analyses with cells expressing a NRP2 polypeptide on the cell surface (either native, or recombinant), immunoassays, fluorescence staining assays, ELISA assays, and microcalorimetry approaches such as ITC (Isothermal Titration Calorimetry).
- biacore assays for example, with appropriately tagged reagents, bound to a sensor chip
- FACS analyses with cells expressing a NRP2 polypeptide on the cell surface either native, or recombinant
- immunoassays fluorescence staining assays
- ELISA assays ELISA assays
- microcalorimetry approaches such as ITC (Isothermal Titration Calorimetry).
- an antibody or antigen-binding fragment thereof comprises variant or otherwise modified Fc region(s), including those having altered properties or biological activities relative to wild-type Fc region(s).
- modified Fc regions include those having mutated sequences, for instance, by substitution, insertion, deletion, or truncation of one or more amino acids relative to a wild-type sequence, hybrid Fc polypeptides composed of domains from different immunoglobulin classes/subclasses, Fc polypeptides having altered glycosylation/sialylation patterns, and Fc polypeptides that are modified or derivatized, for example, by biotinylation (see, e.g., US Application No.
- FcRs e.g., FcyRI, FcyRIla, FcyRIIb, FcyRIIc, FcyRIIIa, FcyRIIIb, FcRn
- pharmacokinetic properties e.g., stability or half-life, bioavailability, tissue distribution, volume of distribution, concentration, elimination rate constant, elimination rate, area under the curve (AUC), clearance, C max , t max , C min , fluctuation
- Fc region e.g., FcyRI, FcyRIla, FcyRIIb, FcyRIIc, FcyRIIIa, FcyRIIIb, FcRn
- pharmacokinetic properties e.g., stability or half-life, bioavailability, tissue distribution, volume of distribution, concentration, elimination rate constant, elimination rate, area under the curve (AUC), clearance, C max , t max , C min , fluctuation
- its immunogenicity e.g., its complement fixation or
- antibodies or antigen-binding fragments thereof that comprise hybrid Fc regions, for example, Fc regions that comprise a combination of Fc domains (e.g., hinge, CH2, CFI3, CH4) from immunoglobulins of different species (e.g., human, mouse), different Ig classes, and/or different Ig subclasses.
- Fc regions that comprise a combination of Fc domains (e.g., hinge, CH2, CFI3, CH4) from immunoglobulins of different species (e.g., human, mouse), different Ig classes, and/or different Ig subclasses.
- hybrid Fc regions that comprise, consist of, or consist essentially of the following combination of CH 2 /CH 3 domains: IgAl/lgAl, lgAl/lgA2, IgAl/lgD, IgAl/lgE, IgAl/lgGl, lgAl/lgG2, lgAl/lgG3, lgAl/lgG4, IgAl/lgM, lgA2/lgAl, lgA2/lgA2, lgA2/lgD, lgA2/lgE, lgA2/lgGl, lgA2/lgG2, lgA2/lgG3, lgA2/lgG4, lgA2/lgM, IgD/lgAl, lgD/lgA2, IgD/lgD, IgD/lgE, IgD/lgGl, lgD/lgG2, lgD
- hybrid Fc regions that comprise, consist of, or consist essentially of the following combination of CH 2 /CH 4 domains: IgAl/lgE, lgA2/lgE, IgD/lgE, IgE/lgE, IgGl/lgE, lgG2/lgE, lgG3/lgE, lgG4/lgE, IgM/lgE, IgAl/lgM, lgA2/lgM, IgD/lgM, IgE/lgM, IgGl/lgM, lgG2/lgM, lgG3/lgM, lgG4/lgM, IgM/lgM (or fragments or variants thereof), and optionally include a hinge from one or more of IgAl, lgA2, IgD, IgGl, lgG2, lgG3, lgG4, and/or a CH 3 domain from one or more
- hybrid Fc regions that comprise, consist of, or consist essentially of the following combination of CH 3 /CH 4 domains: IgAl/lgE, lgA2/lgE, IgD/lgE, IgE/lgE, IgGl/lgE, lgG2/lgE, lgG3/lgE, lgG4/lgE, IgM/lgE, IgAl/lgM, lgA2/lgM, IgD/lgM, IgE/lgM, IgGl/lgM, lgG2/lgM, lgG3/lgM, lgG4/lgM, IgM/lgM (or fragments or variants thereof), and optionally include a hinge from one or more of IgAl, lgA2, IgD, IgGl, lgG2, lgG3, lgG4, and/or a CH 2 domain from one or more
- hybrid Fc regions that comprise, consist of, or consist essentially of the following combination of hinge/CFI 2 domains: IgAl/lgAl, lgAl/lgA2, IgAl/lgD, IgAl/lgE, IgAl/lgGl, lgAl/lgG2, lgAl/lgG3, lgAl/lgG4, IgAl/lgM, lgA2/lgAl, lgA2/lgA2, lgA2/lgD, lgA2/lgE, lgA2/lgGl, lgA2/lgG2, lgA2/lgG3, lgA2/lgG4, lgA2/lgM, IgD/lgAl, lgD/lgA2, IgD/lgD, IgD/lgE,
- IgD/lgGl IgD/lgGl, lgD/lgG2, lgD/lgG3, lgD/lgG4, IgD/lgM, IgGl/lgAl, lgGl/lgA2, IgGl/lgD, IgGl/lgE, IgGl/lgGl, lgGl/lgG2, lgGl/lgG3, lgGl/lgG4, IgGl/lgM, lgG2/lgAl, lgG2/lgA2, lgG2/lgD, lgG2/lgE, lgG2/lgGl, lgG2/lgG2, lgG2/lgG3, lgG2/lgG4, lgG2/lgM, lgG3/lgAl, lgG3/lgA2, lgG3/lgD, lgG
- hybrid Fc regions that comprise, consist of, or consist essentially of the following combination of hinge/CH3 domains: IgAl/lgAl, lgAl/lgA2, IgAl/lgD, IgAl/lgE, IgAl/lgGl, lgAl/lgG2, lgAl/lgG3, lgAl/lgG4, IgAl/lgM, lgA2/lgAl, lgA2/lgA2, lgA2/lgD, lgA2/lgE, lgA2/lgGl, lgA2/lgG2, lgA2/lgG3, lgA2/lgG4, lgA2/lgM, IgD/lgAl, lgD/lgA2, IgD/lgD, IgD/lgE,
- IgD/lgGl IgD/lgGl, lgD/lgG2, lgD/lgG3, lgD/lgG4, IgD/lgM, IgGl/lgAl, lgGl/lgA2, IgGl/lgD, IgGl/lgE, IgGl/lgGl, lgGl/lgG2, lgGl/lgG3, lgGl/lgG4, IgGl/lgM, lgG2/lgAl, lgG2/lgA2, lgG2/lgD, lgG2/lgE, lgG2/lgGl, lgG2/lgG2, lgG2/lgG3, lgG2/lgG4, lgG2/lgM, lgG3/lgAl, lgG3/lgA2, lgG3/lgD, lgG
- hybrid Fc regions that comprise, consist of, or consist essentially of the following combination of hinge/CFU domains: IgAl/lgE, IgAl/lgM, lgA2/lgE, lgA2/lgM, IgD/lgE, IgD/lgM, IgGl/lgE, IgGl/lgM, lgG2/lgE, lgG2/lgM, lgG3/lgE, lgG3/lgM, lgG4/lgE, lgG4/lgM (or fragments or variants thereof), and optionally include a CH2 domain from one or more of IgAl, lgA2, IgD, IgE, IgGl, lgG2, lgG3, lgG4, or IgM, and/or a CH3 domain from one or more of IgAl, lgA2, IgD,
- IgE IgGl, lgG2, lgG3, lgG4, or IgM.
- hybrid Fc regions can be found, for example, in WO 2008/147143, which are derived from combinations of IgG subclasses or combinations of human IgD and IgG.
- the Fc region may be modified by phosphorylation, sulfation, acrylation, glycosylation, methylation, farnesylation, acetylation, amidation, and the like, for instance, relative to a wild-type or naturally-occurring Fc region.
- the Fc region may comprise wild-type or native glycosylation patterns, or alternatively, it may comprise increased glycosylation relative to a native form, decreased glycosylation relative to a native form, or it may be entirely deglycosylated.
- a modified Fc glycoform decreased glycosylation of an Fc region reduces binding to the Clq region of the first complement component Cl, a decrease in ADCC-related activity, and/or a decrease in CDC- related activity.
- Certain embodiments thus employ a deglycosylated or aglycosylated Fc region. See, e.g., WO 2005/047337 for the production of exemplary aglycosylated Fc regions.
- Another example of an Fc region glycoform can be generated by substituting the Q295 position with a cysteine residue (see, e.g., U.S. Application No. 2010/0080794), according to the Kabat et al. numbering system.
- Certain embodiments may include Fc regions where about 80-100% of the glycoprotein in Fc region comprises a mature core carbohydrate structure that lacks fructose (see, e.g., U.S. Application No. 2010/0255013). Some embodiments may include Fc regions that are optimized by substitution or deletion to reduce the level of fucosylation, for instance, to increase affinity for FcyRI, FcyRIa, or FcyRIIIa, and/or to improve phagocytosis by FcyRIIa-expressing cells (see U.S. Application Nos. 2010/0249382 and 2007/0148170).
- an Fc region of an antibody or antigen binding fragment thereof may comprise oligomannose-type N-glycans, and optionally have one or more of the following: increased ADCC effector activity, increased binding affinity for FcyRIIIA (and certain other FcRs), similar or increased binding specificity for the target of the NRP2 polypeptide, similar or higher binding affinity for the target of the NRP2 polypeptide, and/or similar or lower binding affinity for mannose receptor, relative to a corresponding Fc region that contains complex- type N-glycans (see, e.g., U.S. Application No. 2007/0092521 and U.S. Patent No. 7,700,321).
- enhanced affinity of Fc regions for FcyRs has been achieved using engineered glycoforms generated by expression of antibodies in engineered or variant cell lines (see, e.g.,
- Certain Fc region glycoforms comprise an increased proportion of N-glycoside bond type complex sugar chains, which do not have the 1- position of fucose bound to the 6-position of N-acetylglucosamine at the reducing end of the sugar chain (see, e.g., U.S.
- Particular embodiments may include IgG Fc region that is glycosylated with at least one galactose moiety connected to a respective terminal sialic acid moiety by an a-2,6 linkage, optionally where the Fc region has a higher anti-inflammatory activity relative to a corresponding, wild-type Fc region (see U.S. Application No. 2008/0206246).
- Certain of these and related altered glycosylation approaches have generated substantial enhancements of the capacity of Fc regions to selectively bind FcRs such as FcyRIII, to mediate ADCC, and to alter other properties of Fc regions, as described herein.
- Certain variant, fragment, hybrid, or otherwise modified Fc regions of an antibody or antigen-binding fragment thereof may have altered binding to one or more FcRs, and/or corresponding changes to effector function, relative to a corresponding, wild-type Fc sequence (e.g., same species, same Ig class, same Ig subclass). For instance, such Fc regions may have increased binding to one or more of Fey receptors, Fca receptors, Fee receptors, and/or the neonatal Fc receptor, relative to a corresponding, wild-type Fc sequence.
- variant, fragment, hybrid, or modified Fc regions may have decreased binding to one or more of Fey receptors, Fca receptors, Fee receptors, and/or the neonatal Fc receptor, relative to a corresponding, wild-type Fc sequence.
- Fey receptors Fca receptors
- Fee receptors and/or the neonatal Fc receptor, relative to a corresponding, wild-type Fc sequence.
- Specific FcRs are described elsewhere herein.
- an antibody comprises an Fc domain, comprising one or more mutations to increase binding to one or more of Fey receptors, Fca receptors, Fee receptors, and/or the neonatal Fc receptor, relative to a corresponding, wild-type Fc sequence.
- an antibody comprises an IgGl or lgG3 Fc domain, comprising one or more mutations to increase binding to one or more of Fey receptors, Fca receptors, Fee receptors, and/or the neonatal Fc receptor, relative to a corresponding, wild-type Fc sequence.
- an antibody comprises an Fc domain, comprising one or more mutations to increase effector function.
- the at least one antibody comprises an Fc domain selected from a human IgGl and lgG3, comprising one or more mutations to increase effector function.
- an antibody is blocking antibody that comprises an Fc domain with high effector activity.
- the blocking antibody comprises an Fc domain selected from a human IgGl and lgG3, comprising one or more mutations to increase effector function.
- an antibody is a partial-blocking antibody that comprises an Fc domain with high effector activity.
- the a partial-blocking antibody comprises an Fc domain selected from a human IgGl and lgG3, comprising one or more mutations to increase effector function.
- an antibody is a non-blocking antibody that comprises an Fc domain with high effector activity.
- the non-blocking antibody comprises an Fc domain selected from a human IgGl or lgG3, comprising one or more mutations to increase effector function.
- an antibody comprises an Fc domain, comprising one or more mutations to decrease binding to one or more of Fey receptors, Fca receptors, Fee receptors, and/or the neonatal Fc receptor, relative to a corresponding, wild-type Fc sequence.
- an antibody comprises an IgGl or lgG3 Fc domain, comprising one or more mutations to decrease binding to one or more of Fey receptors, Fca receptors, Fee receptors, and/or the neonatal Fc receptor, relative to a corresponding, wild-type Fc sequence.
- an antibody comprises an Fc domain, comprising one or more mutations to decrease effector function.
- an antibody comprises an Fc domain selected from a human lgG2 and lgG4, comprising one or more mutations to decrease effector function.
- an antibody is a blocking antibody comprising an Fc domain with low effector activity.
- the blocking antibody comprises an Fc domain selected from a human lgG2 and lgG4, comprising one or more mutations to decrease effector function.
- an antibody is a partial-blocking antibody comprising an Fc domain with low effector activity.
- the partial-blocking antibody comprises an Fc domain selected from a human lgG2 and lgG4, comprising one or more mutations to decrease effector function.
- an antibody is a non-blocking antibody comprising an Fc domain with low effector activity.
- the non-blocking antibody comprises an Fc domain selected from a human lgG2 and lgG4, comprising one or more mutations to decrease effector function.
- Fc variants having altered (e.g., increased, decreased) effector function/FcR binding can be found, for example, in U.S. Pat. Nos. 5,624,821 and 7,425,619; U.S. Application Nos. 2009/0017023, 2009/0010921, and 2010/0203046; and WO 2000/42072 and WO 2004/016750.
- Certain examples include human Fc regions having a one or more substitutions at position 298, 333, and/or 334, for example, S298A, E333A, and/or K334A (based on the numbering of the EU index of Kabat et al.), which have been shown to increase binding to the activating receptor FcyRIIIa and reduce binding to the inhibitory receptor FcyRIlb. These mutations can be combined to obtain double and triple mutation variants that have further improvements in binding to FcRs.
- Certain embodiments include a S298A/E333A/K334A triple mutant, which has increased binding to FcyRIIIa, decreased binding to FcyRIlb, and increased ADCC (see, e.g., Shields et al., J Biol Chem. 276:6591-6604, 2001; and Presta et al., Biochem Soc Trans. 30:487-490, 2002). See also engineered Fc glycoforms that have increased binding to FcRs, as disclosed in Umana et al., supra; and U.S. Patent No. 7,662,925.
- Some embodiments include Fc regions that comprise one or more substitutions selected from 434S, 252Y/428L, 252Y/434S, and 428L/434S (see U.S. Application Nos. 2009/0163699 and 20060173170), based on the EU index of Kabat et al.
- Certain variant, fragment, hybrid, or modified Fc regions may have altered effector functions, relative to a corresponding, wild-type Fc sequence.
- such Fc regions may have increased complement fixation or activation, increased Clq binding affinity, increased CDC-related activity, increased ADCC-related activity, and/or increased ADCP-related activity, relative to a corresponding, wild-type Fc sequence.
- such Fc regions may have decreased complement fixation or activation, decreased Clq binding affinity, decreased CDC-related activity, decreased ADCC-related activity, and/or decreased ADCP-related activity, relative to a corresponding, wild-type Fc sequence.
- an Fc region may comprise a deletion or substitution in a complement-binding site, such as a Clq-binding site, and/or a deletion or substitution in an ADCC site. Examples of such deletions/substitutions are described, for example, in U.S. Patent No. 7,030,226.
- Many Fc effector functions, such as ADCC can be assayed according to routine techniques in the art. (see, e.g., Zuckerman et al., CRC Crit Rev Microbiol. 7:1- 26, 1978).
- Useful effector cells for such assays includes, but are not limited to, natural killer (NK) cells, macrophages, and other peripheral blood mononuclear cells (PBMC).
- NK natural killer
- PBMC peripheral blood mononuclear cells
- certain Fc effector functions may be assessed in vivo, for example, by employing an animal model described in Clynes et al. PNAS. 95:652-656, 1998.
- variant hybrid, or modified Fc regions may have altered stability or half-life relative to a corresponding, wild-type Fc sequence. In certain embodiments, such Fc regions may have increased half-life relative to a corresponding, wild-type Fc sequence. In other embodiments, variant hybrid, or modified Fc regions may have decreased half-life relative to a corresponding, wild-type Fc sequence. Half-life can be measured in vitro (e.g., under physiological conditions) or in vivo, according to routine techniques in the art, such as radiolabeling, ELISA, or other methods.
- In vivo measurements of stability or half-life can be measured in one or more bodily fluids, including blood, serum, plasma, urine, or cerebrospinal fluid, or a given tissue, such as the liver, kidneys, muscle, central nervous system tissues, bone, etc.
- bodily fluids including blood, serum, plasma, urine, or cerebrospinal fluid, or a given tissue, such as the liver, kidneys, muscle, central nervous system tissues, bone, etc.
- a modified Fc domain for example, a modified IgGl or lgG4 Fc domain, comprises at least one mutation to alter FcRn binding as described, for example, by Zalevsky et al. (Nature Biotechnology. 28(2): 157-159, 2010) or Mackness et al. (mAbs. 11(7): 1276-1288, 2019).
- a modified IgGl or lgG3 Fc domain comprises any one or more of YD (M252Y/T256D), DQ (T256D/T307Q), DW (T256D/T307W), YTE (M252Y/S254T/T256E), AAA (T307A/E380A/N434A), LS (M428L/N434S), M252Y, T256D/E, K288D/N, T307Q/W, E380C, N434FY, or Y436FI/N/W mutations (EU numbering), including combinations thereof.
- a modified IgGl or lgG3 Fc domain comprises any one or more of M252Y, T256D/E, T307Q/W, and/or N434F/Y mutations (EU numbering), including combinations thereof.
- Assays for measuring the in vivo pharmacokinetic properties e.g., in vivo mean elimination half-life
- Fc modifications that alter its binding to the FcRn are described, for example, in U.S. Pat. Nos. 7,217,797 and 7,732,570; and U.S. Application Nos. US 2010/0143254 and 2010/0143254.
- modifications to alter stability or half-life include substitutions/deletions at one or more of amino acid residues selected from 251-256, 285-290, and 308-314 in the CH2 domain, and 385-389 and 428-436 in the CH3 domain, according to the numbering system of Kabat et al. See U.S. Application No. 2003/0190311.
- variant hybrid, or modified Fc regions may have altered solubility relative to a corresponding, wild-type Fc sequence. In certain embodiments, such Fc regions may have increased solubility relative to a corresponding, wild-type Fc sequence. In other embodiments, variant hybrid, or modified Fc regions may have decreased solubility relative to a corresponding, wild-type Fc sequence. Solubility can be measured, for example, in vitro (e.g., under physiological conditions) according to routine techniques in the art. Exemplary solubility measurements are described elsewhere herein.
- variants include IgG Fc regions having conservative or non conservative substitutions (as described elsewhere herein) at one or more of positions 250, 314, or 428 of the heavy chain, or in any combination thereof, such as at positions 250 and 428, or at positions 250 and 314, or at positions 314 and 428, or at positions 250, 314, and 428 (see, e.g., U.S. Application No. 2011/0183412).
- the residue at position 250 is substituted with glutamic acid or glutamine, and/or the residue at position 428 is substituted with leucine or phenylalanine.
- any one or more of the amino acid residues at positions 214 to 238, 297 to 299, 318 to 322, and/or 327 to 331 may be used as a suitable target for modification (e.g., conservative or non-conservative substitution, deletion).
- the IgG Fc variant CF domain contains amino acid substitutions at positions 228, 234, 235, and/or 331 (e.g., human lgG4 with Ser228Pro and Leu235Ala mutations) to attenuate the effector functions of the Fc region (see U.S. Patent No. 7,030,226).
- variant Fc regions that comprise one or more amino acid substitutions at positions 279, 341, 343 or 373 of a wild-type Fc region, or any combination thereof (see, e.g., U.S. Application No. 2007/0224188).
- the wild-type amino acid residues at these positions for human IgG are valine (279), glycine (341), proline (343) and tyrosine (373).
- the substation(s) can be conservative or non-conservative, or can include non-naturally occurring amino acids or mimetics, as described herein.
- certain embodiments may also employ a variant Fc region that comprises at least 1, 2, 3, 4, 5, 6, 7, 8, 9, 10 or more amino acid substitutions selected from the following: 235G, 235R, 236F, 236R, 236Y, 237K, 237N, 237R, 238E, 238G, 238H, 2381, 238L, 238V, 238W, 238Y, 244L, 245R, 247A, 247D, 247E, 247F, 247M, 247N, 247Q, 247R, 247S, 247T, 247W, 247Y, 248F, 248P, 248Q, 248W, 249L, 249M, 249N,
- variant Fc regions typically confer an altered effector function or altered serum half-life upon the antibody to which the variant Fc region is operably attached.
- the altered effector function is an increase in ADCC, a decrease in ADCC, an increase in CDC, a decrease in CDC, an increase in Clq binding affinity, a decrease in Clq binding affinity, an increase in FcR (preferably FcRn) binding affinity or a decrease in FcR (preferably FcRn) binding affinity as compared to a corresponding Fc region that lacks such amino acid substitution(s).
- variant Fc regions that comprise an amino acid substitution at one or more of position(s) 221, 222, 224, 227, 228, 230, 231, 223, 233, 234, 235, 236, 237, 238, 239, 240, 241, 243, 244, 245, 246, 247, 249, 250, 258, 262, 263, 264, 265, 266, 267, 268, 269, 270, 271,
- the variant Fc region comprises at least one amino acid substitution selected from the group consisting of: P230A, E233D, L234E, L234Y, L234I, L235D, L235S, L235Y, L235I, S239D, S239E, S239N, S239Q, S239T, V240I, V240M, F243L, V264I, V264T, V264Y, V266I, E272Y, K274T, K274E, K274R, K274L, K274Y, F275W, N276L, Y278T, V302I, E318R, S324D, S324I, S324V, N325T, K326I, K326T, L328M, L328I, L328Q, L328D, L328V, L328
- the variant Fc region comprises at least one amino acid substitution selected from the group consisting of: V264I, F243L/V264I, L328M, I332E, L328M/I332E, V264I/I332E, S298A/I332E, S239E/I332E, S239Q/I332E, S239E, A330Y, I332D, L328I/I332E, L328Q/I332E, V264T, V240I, V266I, S239D, S239D/I332D, S239D/I332E, S239D/I332N, S239D/I332Q, S239E/I332D, S239E/I332N, S239E/I332a S239N/I332D, S239N/I332E, S239Q/I332D, A330Y/I332E, V264I, F243L
- the variant Fc region comprises an amino acid substitution at position 332 (using the numbering of the EU index, Kabat et al., supra).
- substitutions include 332A, 332D, 332E, 332F, 332G, 332H, 332K, 332 L, 332M, 332N, 332P, 332Q, 332R, 332S, 332T, 332V, 332W and 332Y.
- the numbering of the residues in the Fc region is that of the EU index of Kabat et al.
- such variant Fc regions may have increased affinity for an FcyR, increased stability, and/or increased solubility, relative to a corresponding, wild-type Fc region.
- variant Fc regions that comprise one or more of the following amino acid substitutions: 224N/Y, 225A, 228L, 230S, 239P, 240A, 241L, 243S/L/G/H/I, 244L, 246E, 247L/A, 252T, 254T/P, 258K, 261Y, 265V, 266A, 267G/N, 268N, 269K/G, 273A, 276D, 278H, 279M, 280N, 283G, 285R, 288R, 289A, 290E, 291L, 292Q, 297D, 299A, 300H, 301C, 304G, 305A, 3061/F, 311R, 312N, 315D/K/S, 320R, 322E, 323A, 324T, 325S, 326E/R, 332T, 333D/G, 3351, 338R, 339
- variant Fc regions that comprise or consist of the following sets of substitutions: (1) N276D, R292Q, V305A, 1377V, T394A, V412A and K439E; (2) P244L, K246E, D399G and K409R; (3) S304G, K320R, S324T, K326E and M358T; (4) F243S, P247L, D265V, V266A, S383N and T411I; (5) H224N, F243L, T393A and H433P; (6) V240A, S267G, G341E and E356G; (7) M252T, P291L, P352A, R355W, N390D, S408G, S426F and A431S; (8) P228L, T289A, L365Q, N389S and 5440G; (9) F241L, V273A,
- Variant Fc regions can also have one or more mutated hinge regions, as described, for example, in U.S. Application No. 2003/0118592.
- one or more cysteines in a hinge region can be deleted or substituted with a different amino acid.
- the mutated hinge region can comprise no cysteine residues, or it can comprise 1, 2, or 3 fewer cysteine residues than a corresponding, wild-type hinge region.
- an Fc region having a mutated hinge region of this type exhibits a reduced ability to dimerize, relative to a wild-type Ig hinge region.
- the Fc region comprises, consists, or consists essentially of the Fc from human IgGl or lgG4 (see, e.g., Allberse and Schuurman, Immunology. 105:9-19, 2002), or a fragment or variant thereof.
- Table FI below provides exemplary sequences (CFI1, hinge (underlined), CFI2, and CH3 regions) from human IgGl and lgG4. Examples of variant lgG4 sequences that can be employed are described, for example, in Peters et al., JBC. 287:24525-24533, 2012, and include substitutions at C227, C230, C127 (e.g., C127S), and C131 (e.g., C131S).
- variants that can be used include a L445P substitution in lgG4 (denoted as lgG4-2) or a D356E and L358M substitution in IgGl, (denoted as IgGlm(zf)).
- antibodies having altered Fc regions typically have altered ( e.g improved, increased, decreased) pharmacokinetic properties relative to corresponding wild-type Fc region.
- pharmacokinetic properties include stability or half-life, bioavailability (the fraction of a drug that is absorbed), tissue distribution, volume of distribution (apparent volume in which a drug is distributed immediately after it has been injected intravenously and equilibrated between plasma and the surrounding tissues), concentration (initial or steady-state concentration of drug in plasma), elimination rate constant (rate at which drugs are removed from the body), elimination rate (rate of infusion required to balance elimination), area under the curve (AUC or exposure; integral of the concentration-time curve, after a single dose or in steady state), clearance (volume of plasma cleared of the drug per unit time), C max (peak plasma concentration of a drug after oral administration), t max (time to reach C max ), C mm (lowest concentration that a drug reaches before the next dose is administered), and fluctuation (peak trough fluctuation within one dosing interval at steady
- an antibody or antigen-binding fragment thereof has a biological half life at about pH 7.4, at about a physiological pH, at about 25 Q C or room temperature, and/or at about 37°C or human body temperature (e.g., in vivo, in serum, in a given tissue, in a given species such as rat, mouse, monkey, or human), of about or at least about 30 minutes, about 1 hour, about 2 hour, about 3 hours, about 4 hours, about 5 hours, about 6 hours, about 12 hours, about 18 hours, about 20 hours, about 24 hours, about 30 hours, about 36 hours, about 40 hours, about 48 hours, about 50 hours, about 60 hours, about 70 hours, about 72 hours, about 80 hours, about 84 hours, about 90 hours, about 96 hours, about 120 hours, or about 144 hours or more, or about 1 week, or about 2 weeks, or about 3 weeks, or about 4 weeks, or about 5 weeks, or about 6 weeks or more, or any intervening half-life, including all ranges in between.
- a biological half life at about pH
- an antibody or antigen-binding fragment thereof has a T m of about or at least about 60, 62, 64, 66, 68, 70, 72, 74, or 75°C. In some embodiments, an antibody or antigen binding fragment thereof has a T m of about 60 °C or greater.
- an antibody or antigen-binding fragment thereof conjugated to one or more cytotoxic or chemotherapeutic agents conjugated to one or more cytotoxic or chemotherapeutic agents.
- cytotoxic or chemotherapeutic agents include, without limitation, alkylating agents, anti-metabolites, anthracyclines, anti-tumor antibiotics, platinums, type I topoisomerase inhibitors, type II topoisomerase inhibitors, vinca alkaloids, and taxanes.
- cytotoxic or chemotherapeutic agents include, without limitation, cyclophosphamide, cilengitide, lomustine (CCNU), melphalan, procarbazine, carmustine (BCNU), enzastaurin, busulfan, daunorubicin, doxorubicin, gefitinib, erlotinib idarubicin, temozolomide, epirubicin, mitoxantrone, bleomycin, cisplatin, carboplatin, oxaliplatin, camptothecins, irinotecan, topotecan, amsacrine, etoposide, etoposide phosphate, teniposide, temsirolimus, everolimus, vincristine, vinblastine, vinorelbine, vindesine, CT52923, paclitaxel, imatinib, dasatinib, sorafenib, pazopan
- cytotoxic or chemotherapeutic agents include alkylating agents such as thiotepa, cyclophosphamide (CYTOXANTM); alkyl sulfonates such as busulfan, improsulfan and piposulfan; aziridines such as benzodopa, carboquone, meturedopa, and uredopa; ethylenimines and methylamelamines including altretamine, triethylenemelamine, trietylenephosphoramide, triethylenethiophosphaoramide and trimethylolomelamine; nitrogen mustards such as chlorambucil, chlornaphazine, cholophosphamide, estramustine, ifosfamide, mechlorethamine, mechlorethamine oxide hydrochloride, melphalan, novembichin, phenesterine, prednimustine, trofosfamide, uracil mustard; nitrosureas such as car
- the antibodies or antigen-binding fragments thereof can be used in any of the compositions, methods, and/or kits described herein, and combined with one or more of the immunotherapy agents described herein.
- an immunotherapy agent modulates the immune response of a subject, for example, to increase or maintain a cancer-related or cancer-specific immune response, and thereby results in increased immune cell inhibition or reduction of cancer cells.
- exemplary immunotherapy agents include polypeptides, for example, antibodies and antigen-binding fragments thereof, ligands, and small peptides, and mixtures thereof.
- immunotherapy agents are small molecules, cells (e.g., immune cells such as T-cells), various cancer vaccines, gene therapy or other polynucleotide-based agents, including viral agents such as oncolytic viruses, and others known in the art.
- the cancer immunotherapy agent is selected from one or more of immune checkpoint modulatory agents, cancer vaccines, oncolytic viruses, cytokines, and a cell-based immunotherapies.
- the cancer immunotherapy agent is an immune checkpoint modulatory agent.
- immune checkpoint molecules are components of the immune system that either turn up a signal (co-stimulatory molecules) or turn down a signal, the targeting of which has therapeutic potential in cancer because cancer cells can perturb the natural function of immune checkpoint molecules (see, e.g., Sharma and Allison, Science. 348:56-61, 2015; Topalian et al., Cancer Cell. 27:450-461, 2015; Pardoll, Nature Reviews Cancer. 12:252-264, 2012).
- the immune checkpoint modulatory agent e.g., antagonist, agonist
- the immune checkpoint modulatory agent "binds" or “specifically binds” to the one or more immune checkpoint molecules, as described herein.
- the immune checkpoint modulatory agent is a polypeptide or peptide.
- the terms “peptide” and “polypeptide” are used interchangeably herein, however, in certain instances, the term “peptide” can refer to shorter polypeptides, for example, polypeptides that consist of about 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 25, 30, 35, 40, 45, or 50 amino acids, including all integers and ranges (e.g., 5-10, 8-12, 10-15) in between.
- Polypeptides and peptides can be composed of naturally-occurring amino acids and/or non-naturally occurring amino acids, as described herein
- the immune checkpoint modulatory polypeptide agent is an antibody or "antigen-binding fragment thereof", as described elsewhere herein.
- the agent is or comprises a "ligand,” for example, a natural ligand, of the immune checkpoint molecule.
- a “ligand” refers generally to a substance or molecule that forms a complex with a target molecule (e.g., biomolecule) to serve a biological purpose, and includes a “protein ligand,” which generally produces a signal by binding to a site on a target molecule or target protein.
- a target molecule e.g., biomolecule
- protein ligand which generally produces a signal by binding to a site on a target molecule or target protein.
- proteins which generally produces a signal by binding to a site on a target molecule or target protein.
- modified ligands for example, protein ligands that are fused to a pharmacokinetic modifier, for example, an Fc region derived from an immunoglobulin.
- a polypeptide specifically binds to a target molecule, for example, an immune checkpoint molecule or an epitope thereof, with an equilibrium dissociation constant that is about or ranges from about ⁇ 10-7 to about 10-8 M. In some embodiments, the equilibrium dissociation constant is about or ranges from about ⁇ 10-9 M to about ⁇ 10-10 M.
- the polypeptide has an affinity (Kd or EC50) for a target described herein (to which it specifically binds) of about, at least about, or less than about, 0.01, 0.05, 0.1, 0.2, 0.3, 0.4, 0.5, 0.6, 0.7, 0.8, 0.9, 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13,
- the agent is a "small molecule,” which refers to an organic compound that is of synthetic or biological origin (biomolecule), but is typically not a polymer.
- Organic compounds refer to a large class of chemical compounds whose molecules contain carbon, typically excluding those that contain only carbonates, simple oxides of carbon, or cyanides.
- a "biomolecule” refers generally to an organic molecule that is produced by a living organism, including large polymeric molecules (biopolymers) such as peptides, polysaccharides, and nucleic acids as well, and small molecules such as primary secondary metabolites, lipids, phospholipids, glycolipids, sterols, glycerolipids, vitamins, and hormones.
- a "polymer” refers generally to a large molecule or macromolecule composed of repeating structural units, which are typically connected by covalent chemical bond.
- a small molecule has a molecular weight of about or less than about 1000-2000 Daltons, typically between about 300 and 700 Daltons, and including about or less than about 50, 100, 150, 200, 250, 300, 350, 400, 450, 500, 550, 500, 650, 600, 750, 700, 850, 800, 950, 1000 or 2000 Daltons.
- a small molecule specifically binds to a target, for example, an immune checkpoint molecule, with a binding affinity (Kd or EC50) of about, at least about, or less than about, 0.01, 0.05, 0.1, 0.2, 0.3, 0.4, 0.5, 0.6, 0.7, 0.8, 0.9, 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 40, or 50 nM.
- Kd or EC50 binding affinity
- the immune checkpoint modulatory agent is an antagonist or inhibitor of one or more inhibitory immune checkpoint molecules.
- inhibitory immune checkpoint molecules include Programmed Death-Ligand 1 (PD-L1), Programmed Death-Ligand 2 (PD-L2), Programmed Death 1 (PD-1), Cytotoxic T-Lymphocyte-Associated protein 4 (CTLA-4), Indoleamine 2,3-dioxygenase (IDO), tryptophan 2,3-dioxygenase (TDO), T-cell Immunoglobulin domain and Mucin domain 3 (TIM-3), Lymphocyte Activation Gene-3 (LAG-3), V-domain Ig suppressor of T cell activation (VISTA), B and T Lymphocyte Attenuator (BTLA), CD160, and T-cell immunoreceptor with Ig and ITIM domains (TIGIT).
- P-L1 Programmed Death-Ligand 1
- PD-L2 Programmed Death-Ligand 2
- PD-1 Programmed Death 1
- CTL-4 Cytotoxic T
- the agent is a PD-1 (receptor) antagonist or inhibitor, the targeting of which has been shown to restore immune function in the tumor environment (see, e.g., Phillips et al., Int Immunol. 27:39-46, 2015).
- PD-1 is a cell surface receptor that belongs to the immunoglobulin superfamily and is expressed on T cells and pro-B cells.
- PD-1 interacts with two ligands, PD-L1 and PD-L2.
- PD-1 functions as an inhibitory immune checkpoint molecule, for example, by reducing or preventing the activation of T-cells, which in turn reduces autoimmunity and promotes self tolerance.
- the inhibitory effect of PD-1 is accomplished at least in part through a dual mechanism of promoting apoptosis in antigen specific T-cells in lymph nodes while also reducing apoptosis in regulatory T cells (suppressor T cells).
- Some examples of PD-1 antagonists or inhibitors include an antibody or antigen-binding fragment or small molecule that specifically binds to PD-1 and reduces one or more of its immune-suppressive activities, for example, its downstream signaling or its interaction with PD-L1.
- PD-1 antagonists or inhibitors include the antibodies nivolumab, pembrolizumab, PDR001, MK-3475, AMP-224, AMP-514, and pidilizumab, and antigen binding fragments thereof (see, e.g., U.S. Patent Nos. 8,008,449; 8,993,731; 9,073,994; 9,084,776; 9,102,727; 9,102,728; 9,181,342; 9,217,034; 9,387,247; 9,492,539; 9,492,540; and U.S. Application Nos. 2012/0039906; 2015/0203579).
- the agent is a PD-L1 antagonist or inhibitor.
- PD-L1 is one of the natural ligands for the PD-1 receptor.
- General examples of PD-L1 antagonists or inhibitors include an antibody or antigen-binding fragment or small molecule that specifically binds to PD-L1 and reduces one or more of its immune-suppressive activities, for example, its binding to the PD-1 receptor.
- Specific examples of PD-L1 antagonists include the antibodies atezolizumab (MPDL3280A), avelumab (MSB0010718C), and durvalumab (MEDI4736), and antigen-binding fragments thereof (see, e.g., U.S. Patent Nos. 9,102,725; 9,393,301; 9,402,899; 9,439,962).
- the agent is a PD-L2 antagonist or inhibitor.
- PD-L2 is one of the natural ligands for the PD-1 receptor.
- General examples of PD-L2 antagonists or inhibitors include an antibody or antigen-binding fragment or small molecule that specifically binds to PD-L2 and reduces one or more of its immune-suppressive activities, for example, its binding to the PD-1 receptor.
- the agent is a CTLA-4 antagonist or inhibitor.
- CTLA4 or CTLA-4 cytotoxic T-lymphocyte-associated protein 4
- CD152 cluster of differentiation 152
- CTLA-4 antagonists or inhibitors include an antibody or antigen binding fragment or small molecule that specifically binds to CTLA-4.
- Particular examples include the antibodies ipilimumab and tremelimumab, and antigen-binding fragments thereof. At least some of the activity of ipilimumab is believed to be mediated by antibody-dependent cell-mediated cytotoxicity (ADCC) killing of suppressor Tregs that express CTLA-4.
- ADCC antibody-dependent cell-mediated cytotoxicity
- the agent is an IDO antagonist or inhibitor, or a TDO antagonist or inhibitor.
- IDO and TDO are tryptophan catabolic enzymes with immune-inhibitory properties.
- IDO is known to suppress T-cells and NK cells, generate and activate Tregs and myeloid- derived suppressor cells, and promote tumor angiogenesis.
- General examples of IDO and TDO antagonists or inhibitors include an antibody or antigen-binding fragment or small molecule that specifically binds to IDO or TDO (see, e.g., Platten et al., Front Immunol. 5: 673, 2014) and reduces or inhibits one or more immune-suppressive activities.
- IDO antagonists or inhibitors include indoximod (NLG-8189), 1-methyl-tryptophan (1MT), b-Carboline (norharmane; 9H- pyrido[3,4-b]indole), rosmarinic acid, and epacadostat (see, e.g., Sheridan, Nature Biotechnology. 33:321-322, 2015).
- TDO antagonists or inhibitors include 680C91 and LM10 (see, e.g., Pilotte et al., PNAS USA. 109:2497-2502, 2012).
- the agent is a TIM-3 antagonist or inhibitor.
- T-cell Immunoglobulin domain and Mucin domain 3 (TIM-3) is expressed on activated human CD4+ T-cells and regulates Thl and Thl7 cytokines.
- TIM-3 also acts as a negative regulator of Thl/Tcl function by triggering cell death upon interaction with its ligand, galectin-9.
- TIM-3 contributes to the suppressive tumor microenvironment and its overexpression is associated with poor prognosis in a variety of cancers (see, e.g., Li et al., Acta Oncol. 54:1706-13, 2015).
- General examples of TIM-3 antagonists or inhibitors include an antibody or antigen-binding fragment or small molecule that specifically binds to TIM-3 and reduces or inhibits one or more of its immune-suppressive activities.
- the agent is a LAG-3 antagonist or inhibitor.
- Lymphocyte Activation Gene-3 (LAG-3) is expressed on activated T-cells, natural killer cells, B-cells and plasmacytoid dendritic cells. It negatively regulates cellular proliferation, activation, and homeostasis of T-cells, in a similar fashion to CTLA-4 and PD-1 (see, e.g., Workman and Vignali. European Journal of Immun. 33: 970-9, 2003; and Workman et al., Journal of Immun. 172: 5450-5, 2004), and has been reported to play a role in Treg suppressive function (see, e.g., Huang et al., Immunity. 21: 503-13, 2004).
- LAG3 also maintains CD8+ T-cells in a tolerogenic state and combines with PD-1 to maintain CD8 T-cell exhaustion.
- LAG-3 antagonists or inhibitors include an antibody or antigen binding fragment or small molecule that specifically binds to LAG-3 and inhibits one or more of its immune-suppressive activities. Specific examples include the antibody BMS-986016, and antigen binding fragments thereof.
- the agent is a VISTA antagonist or inhibitor.
- V-domain Ig suppressor of T cell activation VISTA is primarily expressed on hematopoietic cells and is an inhibitory immune checkpoint regulator that suppresses T-cell activation, induces Foxp3 expression, and is highly expressed within the tumor microenvironment where it suppresses anti-tumor T cell responses (see, e.g., Lines et al., Cancer Res. 74:1924-32, 2014).
- VISTA antagonists or inhibitors include an antibody or antigen-binding fragment or small molecule that specifically binds to VISTA and reduces one or more of its immune-suppressive activities.
- the agent is a BTLA antagonist or inhibitor.
- B- and T-lymphocyte attenuator (BTLA; CD272) expression is induced during activation of T-cells, and it inhibits T-cells via interaction with tumor necrosis family receptors (TNF-R) and B7 family of cell surface receptors.
- TNF-R tumor necrosis family receptors
- BTLA is a ligand for tumor necrosis factor (receptor) superfamily, member 14 (TNFRSF14), also known as herpes virus entry mediator (HVEM).
- HVEM herpes virus entry mediator
- BTLA-HVEM complexes negatively regulate T-cell immune responses, for example, by inhibiting the function of human CD8+ cancer-specific T-cells (see, e.g., Derre et al., J Clin Invest 120:157-67, 2009).
- HVEM herpes virus entry mediator
- BTLA-HVEM complexes negatively regulate T-cell immune responses, for example, by inhibiting the function of human CD8+ cancer-specific T-cells (see, e.g., Derre et al., J Clin Invest 120:157-67, 2009).
- General examples of BTLA antagonists or inhibitors include an antibody or antigen-binding fragment or small molecule that specifically binds to BTLA-4 and reduce one or more of its immune-suppressive
- the agent is an HVEM antagonist or inhibitor, for example, an antagonist or inhibitor that specifically binds to HVEM and interferes with its interaction with BTLA or CD160.
- HVEM antagonists or inhibitors include an antibody or antigen binding fragment or small molecule that specifically binds to HVEM, optionally reduces the HVEM/BTLA and/or HVEM/CD160 interaction, and thereby reduces one or more of the immune- suppressive activities of HVEM.
- the agent is a CD160 antagonist or inhibitor, for example, an antagonist or inhibitor that specifically binds to CD160 and interferes with its interaction with HVEM.
- CD160 antagonists or inhibitors include an antibody or antigen-binding fragment or small molecule that specifically binds to CD160, optionally reduces the CD160/HVEM interaction, and thereby reduces or inhibits one or more of its immune-suppressive activities.
- the agent is a TIGIT antagonist or inhibitor.
- T cell Ig and ITIM domain (TIGIT) is a co-inhibitory receptor that is found on the surface of a variety of lymphoid cells, and suppresses antitumor immunity, for example, via Tregs (Kurtulus et al., J Clin Invest. 125:4053-4062, 2015).
- TIGIT antagonists or inhibitors include an antibody or antigen-binding fragment or small molecule that specifically binds to TIGIT and reduce one or more of its immune- suppressive activities (see, e.g., Johnston et al., Cancer Cell. 26:923-37, 2014).
- the immune checkpoint modulatory agent is an agonist of one or more stimulatory immune checkpoint molecules.
- stimulatory immune checkpoint molecules include 0X40, CD40, Glucocorticoid-Induced TNFR Family Related Gene (GITR), CD137 (4- 1BB), CD27, CD28, CD226, and Herpes Virus Entry Mediator (HVEM).
- the agent is an 0X40 agonist.
- 0X40 (CD134) promotes the expansion of effector and memory T cells, and suppresses the differentiation and activity of T-regulatory cells (see, e.g., Croft et al., Immunol Rev. 229:173-91, 2009).
- Its ligand is OX40L (CD252). Since 0X40 signaling influences both T-cell activation and survival, it plays a key role in the initiation of an anti tumor immune response in the lymph node and in the maintenance of the anti-tumor immune response in the tumor microenvironment.
- 0X40 agonists include an antibody or antigen-binding fragment or small molecule or ligand that specifically binds to 0X40 and increases one or more of its immunostimulatory activities. Specific examples include 0X86, OX-40L, Fc-OX40L, GSK3174998, MEDI0562 (a humanized 0X40 agonist), MEDI6469 (murine 0X4 agonist), and MEDI6383 (an 0X40 agonist), and antigen-binding fragments thereof.
- the agent is a CD40 agonist.
- CD40 is expressed on antigen-presenting cells (APC) and some malignancies. Its ligand is CD40L (CD154).
- CD40 agonist therapy plays an important role in APC maturation and their migration from the tumor to the lymph nodes, resulting in elevated antigen presentation and T cell activation.
- Anti-CD40 agonist antibodies produce substantial responses and durable anticancer immunity in animal models, an effect mediated at least in part by cytotoxic T-cells (see, e.g., Johnson et al. Clin Cancer Res. 21: 1321-1328, 2015; and Vonderheide and Glennie, Clin Cancer Res. 19:1035- 43, 2013).
- CD40 agonists include an antibody or antigen-binding fragment or small molecule or ligand that specifically binds to CD40 and increases one or more of its immunostimulatory activities.
- Specific examples include CP-870,893, dacetuzumab, Chi Lob 7/4, ADC-1013, CD40L, rhCD40L, and antigen-binding fragments thereof.
- the agent is a GITR agonist.
- Glucocorticoid-Induced TNFR family Related gene increases T cell expansion, inhibits the suppressive activity of Tregs, and extends the survival of T-effector cells.
- GITR agonists have been shown to promote an anti-tumor response through loss of Treg lineage stability (see, e.g., Schaer et al., Cancer Immunol Res. 1:320-31, 2013). These diverse mechanisms show that GITR plays an important role in initiating the immune response in the lymph nodes and in maintaining the immune response in the tumor tissue. Its ligand is GITRL.
- GITR agonists include an antibody or antigen-binding fragment or small molecule or ligand that specifically binds to GITR and increases one or more of its immunostimulatory activities.
- Specific examples include GITRL, INCAGN01876, DTA-1, MEDI1873, and antigen-binding fragments thereof.
- the agent is a CD137 agonist.
- CD137 (4-1BB) is a member of the tumor necrosis factor (TNF) receptor family, and crosslinking of CD137 enhances T-cell proliferation, IL-2 secretion, survival, and cytolytic activity.
- CD137-mediated signaling also protects T-cells such as CD8+ T-cells from activation-induced cell death.
- CD137 agonists include an antibody or antigen-binding fragment or small molecule or ligand that specifically binds to CD137 and increases one or more of its immunostimulatory activities. Specific examples include the CD137 (or 4-1BB) ligand (see, e.g., Shao and Schwarz, J Leukoc Biol. 89:21-9, 2011) and the antibody utomilumab, including antigen-binding fragments thereof.
- the agent is a CD27 agonist. Stimulation of CD27 increases antigen- specific expansion of naive T cells and contributes to T-cell memory and long-term maintenance of T- cell immunity. Its ligand is CD70.
- the targeting of human CD27 with an agonist antibody stimulates T-cell activation and antitumor immunity (see, e.g., Thomas et al., Oncoimmunology. 2014;3:e27255. doi:10.4161/onci.27255; and He et al J Immunol. 191:4174-83, 2013).
- CD27 agonists include an antibody or antigen-binding fragment or small molecule or ligand that specifically binds to CD27 and increases one or more of its immunostimulatory activities.
- Specific examples include CD70 and the antibodies varlilumab and CDX-1127 (1F5), including antigen-binding fragments thereof.
- the agent is a CD28 agonist.
- CD28 is constitutively expressed CD4+ T cells some CD8+ T cells.
- Its ligands include CD80 and CD86, and its stimulation increases T-cell expansion.
- General examples of CD28 agonists include an antibody or antigen-binding fragment or small molecule or ligand that specifically binds to CD28 and increases one or more of its immunostimulatory activities. Specific examples include CD80, CD86, the antibody TAB08, and antigen-binding fragments thereof.
- the agent is CD226 agonist.
- CD226 is a stimulating receptor that shares ligands with TIGIT, and opposite to TIGIT, engagement of CD226 enhances T-cell activation (see, e.g., Kurtulus et al., J Clin Invest. 125:4053-4062, 2015; Bottino et al., J Exp Med. 1984:557-567, 2003; and Tahara-Hanaoka et al., Int Immunol. 16:533-538, 2004).
- General examples of CD226 agonists include an antibody or antigen-binding fragment or small molecule or ligand (e.g., CD112, CD155) that specifically binds to CD226 and increases one or more of its immunostimulatory activities.
- the agent is an HVEM agonist.
- Herpesvirus entry mediator also known as tumor necrosis factor receptor superfamily member 14 (TNFRSF14), is a human cell surface receptor of the TNF-receptor superfamily.
- HVEM is found on a variety of cells including T- cells, APCs, and other immune cells. Unlike other receptors, HVEM is expressed at high levels on resting T-cells and down-regulated upon activation. It has been shown that HVEM signaling plays a crucial role in the early phases of T-cell activation and during the expansion of tumor-specific lymphocyte populations in the lymph nodes.
- General examples of HVEM agonists include an antibody or antigen-binding fragment or small molecule or ligand that specifically binds to HVEM and increases one or more of its immunostimulatory activities.
- the cancer immunotherapy agent is a cancer vaccine.
- exemplary cancer vaccines include Oncophage, human papillomavirus HPV vaccines such Gardasil or Cervarix, hepatitis B vaccines such as Engerix-B, Recombivax HB, or Twinrix, and sipuleucel-T (Provenge).
- the cancer vaccine comprises or utilizes one or more cancer antigens, or cancer-associate d antigens.
- Exemplary cancer antigens include, without limitation, human Her2/neu, Herl/EGF receptor (EGFR), Her3, A33 antigen, B7H3, CD5, CD19, CD20, CD22, CD23 (IgE Receptor), MAGE-3, C242 antigen, 5T4, IL-6, IL-13, vascular endothelial growth factor VEGF (e.g., VEGF-A) VEGFR-1, VEGFR-2, VEGFR-3, NRP2, CD30, CD33, CD37, CD40, CD44, CD51, CD52, CD56, CD74, CD80, CD152, CD200, CD221, CCR4, HLA-DR, CTLA-4, NPC-1C, tenascin, vimentin, insulin-like growth factor 1 receptor (IGF-1R), alpha-fetoprotein, insulin-like growth factor 1 (IGF-1), carbonic anhydrase 9 (CA-IX), carcinoembryonic antigen (CEA), guanylyl cycla
- the cancer immunotherapy agent is an oncolytic virus.
- An oncolytic virus is a virus that preferentially infects and kills cancer cells. Included are naturally-occurring and man-made or engineered oncolytic viruses. Most oncolytic viruses are engineered for tumor selectivity, although there are naturally-occurring examples such as Reovirus and the SVV-001 Seneca Valley virus. General examples of oncolytic viruses include VSV, Poliovirus, Reovirus, Senecavirus, and RIGVIR, and engineered versions thereof.
- Non-limiting examples of oncolytic viruses include herpes simplex virus (HSV) and engineered version thereof, talimogene laherparepvec (T-VEC), coxsackievirus A21 (CAVATAKTM), Oncorine (H101), pelareorep (REOLYSIN ® ), Seneca Valley virus (NTX-010), Senecavirus SVV-001, ColoAdl, SEPREHVIR (HSV-1716), CGTG-102 (Ad5/3-D24-GMCSF), GL-ONC1, MV-NIS, and DNX-2401, among others.
- HSV herpes simplex virus
- T-VEC talimogene laherparepvec
- CAVATAKTM coxsackievirus A21
- Oncorine H101
- pelareorep REOLYSIN ®
- Seneca Valley virus NTX-010
- Senecavirus SVV-001 Senecavirus
- the cancer immunotherapy agent is a cytokine.
- cytokines include interferon (IFN)-a, IL-2, IL-12, IL-7, IL-21, and Granulocyte-macrophage colony- stimulating factor (GM-CSF).
- IFN interferon
- IL-2 IL-2
- IL-12 IL-12
- IL-7 IL-21
- GM-CSF Granulocyte-macrophage colony- stimulating factor
- the cancer immunotherapy agent is cell-based immunotherapy, for example, a T-cell based adoptive immunotherapy.
- the cell-based immunotherapy comprises cancer antigen-specific T-cells, optionally ex v/Vo-derived T-cells.
- the cancer antigen-specific T-cells are selected from one or more of chimeric antigen receptor (CAR)-modified T-cells, and T-cell Receptor (TCR)-modified T-cells, tumor infiltrating lymphocytes (TILs), and peptide-induced T-cells.
- CAR-modified T-cell is targeted against CD-19 (see, e.g., Maude et al., Blood.
- the cancer to be treated associates with the cancer antigen, that is, the cancer antigen-specific T-cells are targeted against or enriched for at least one antigen that is known to associate with the cancer to be treated.
- the cancer antigen is selected from one or more of CD19, human Her2/neu, Herl/EGF receptor (EGFR), Fler3, A33 antigen, B7FI3, CD5, CD20, CD22, CD23 (IgE Receptor), MAGE-3, C242 antigen, 5T4, IL-6, IL-13, vascular endothelial growth factor VEGF (e.g., VEGF-A) VEGFR-1, VEGFR-2, CD30, CD33, CD37, CD40, CD44, CD51, CD52, CD56, CD74, CD80, CD152, CD200, CD221, CCR4, HLA-DR, CTLA-4, NPC-1C, tenascin, vimentin, insulin-like growth factor 1 receptor (IGF-1R), alpha-fetoprotein, insulin-like growth factor 1 (IGF-1), carbonic anhydrase 9 (CA-IX), carcinoembryonic antigen (CEA), guanylyl cyclase C
- Additional exemplary cancer antigens include 5T4, 707-AP, 9D7, AFP, AlbZIP HPG1, alpha-5- beta-1 -integrin, alpha- 5-beta-6-integrin, alpha-actinin-4/m, alpha-methylacyl-coenzyme A racemase, ART-4, ARTCl/m, B7H4, BAGE-1, BCL-2, bcr/abl, beta-catenin/m, BING-4, BRCAl/m, BRCA2/m, CA 15-3/CA 27-29, CA 19-9, CA72-4, CA125, calreticulin, CAMEL, CASP-8/m, cathepsin B, cathepsin L, CDC27/m, CDK4/m, CDKN2A/m, CEA, CLCA2, CML28, CML66, COA-l/m, coactosin-like protein, collage XXIII, COX-2, CT-9/BRD6, Cten, cyclin B
- Certain preferred antigens include p53, CA125, EGFR, Her2/neu, hTERT, PAP, MAGE-A1, MAGE-A3, Mesothelin, MUC-1, GP100, MART-1, Tyrosinase, PSA, PSCA, PSMA, STEAP-1, Ras, CEA and WTl, and more preferably PAP, MAGE-A3, WTl, and MUC- 1.
- the antigen is selected from MAGE-A1 (e.g., MAGE-A1 according to accession number M77481 ), MAGE-A2, MAGE-A3, MAGE-A6 (e.g., MAGE-A6 according to accession number NM_005363), MAGE-C1, MAGE-C2, melan-A (e.g., melan-A according to accession number NM_00551 1 ), GP100 (e.g., GP100 according to accession number M77348), tyrosinase (e.g., tyrosinase according to accession number NM_000372), survivin (e.g., survivin according to accession number AF077350), CEA (e.g., CEA according to accession number NM_004363), Her- 2/neu (e.g., Fler-2/neu according to accession number Ml 1 730), WTl (e.g., WTl according to
- the cancer antigen is selected from PCA, PSA, PSMA, STEAP, and optionally MUC-1, including fragments, variants, and derivatives thereof.
- the cancer antigen selected from NY-ESO-1, MAGE-C1, MAGE-C2, survivin, 5T4, and optionally MUC- 1, including fragments, variants, and derivatives thereof.
- cancer antigens encompass idiotypic antigens associated with a cancer or tumor disease, particularly lymphoma or a lymphoma associated disease, for example, wherein the idiotypic antigen is an immunoglobulin idiotype of a lymphoid blood cell or a T cell receptor idiotype of a lymphoid blood cell.
- the cancer antigen-specific T-cells are selected from one or more of chimeric antigen receptor (CAR)-modified T-cells (e.g., targeted against a cancer antigen), and T-cell Receptor (TCR)-modified T-cells, tumor infiltrating lymphocytes (TILs), and peptide-induced T-cells.
- CAR chimeric antigen receptor
- TCR T-cell Receptor
- Chemotherapeutic Agents employ one or more chemotherapeutic agents, for example, small molecule chemotherapeutic agents.
- chemotherapeutic agents include alkylating agents, anti-metabolites, cytotoxic antibiotics, topoisomerase inhibitors (type 1 or type II), an anti-microtubule agents, among others.
- alkylating agents include nitrogen mustards (e.g., mechlorethamine, cyclophosphamide, mustine, melphalan, chlorambucil, ifosfamide , and busulfan), nitrosoureas (e.g., N-Nitroso-N-methylurea (MNU), carmustine (BCNU), lomustine (CCNU), semustine (MeCCNU), fotemustine, and streptozotocin), tetrazines (e.g., dacarbazine, mitozolomide, and temozolomide), aziridines (e.g., thiotepa, mytomycin, and diaziquone (AZQ)), cisplatins and derivatives thereof (e.g., carboplatin and oxaliplatin), and non-classical alkylating agents (optionally procarbazine and hexamethylmelamine).
- nitrogen mustards e.g., mech
- anti-metabolites include anti-folates (e.g., methotrexate and pemetrexed), fluoropyrimidines (e.g., 5-fluorouracil and capecitabine), deoxynucleoside analogues (e.g., ancitabine, enocitabine, cytarabine, gemcitabine, decitabine, azacitidine, fludarabine, nelarabine, cladribine, clofarabine, fludarabine, and pentostatin), and thiopurines (e.g., thioguanine and mercaptopurine);
- anti-folates e.g., methotrexate and pemetrexed
- fluoropyrimidines e.g., 5-fluorouracil and capecitabine
- deoxynucleoside analogues e.g., ancitabine, enocitabine, cytarabine, gemcitabine,
- cytotoxic antibiotics examples include anthracyclines (e.g., doxorubicin, daunorubicin, epirubicin, idarubicin, pirarubicin, aclarubicin, and mitoxantrone), bleomycins, mitomycin C, mitoxantrone, and actinomycin.
- anthracyclines e.g., doxorubicin, daunorubicin, epirubicin, idarubicin, pirarubicin, aclarubicin, and mitoxantrone
- bleomycins mitomycin C
- mitoxantrone examples include camptothecin, irinotecan, topotecan, etoposide, doxorubicin, mitoxantrone, teniposide, novobiocin, merbarone, and aclarubicin.
- anti-microtubule agents examples include taxanes (e.g., paclitaxel and docetaxel) and vinca alkaloids (e.g., vinblastine, vincristine, vindesine, vinorelbine).
- taxanes e.g., paclitaxel and docetaxel
- vinca alkaloids e.g., vinblastine, vincristine, vindesine, vinorelbine
- Hormonal Therapeutic Agents employ at least one hormonal therapeutic agent.
- hormonal therapeutic agents include hormonal agonists and hormonal antagonists.
- hormonal agonists include progestogen (progestin), corticosteroids (e.g., prednisolone, methylprednisolone, dexamethasone), insulin like growth factors, VEGF derived angiogenic and lymphangiogenic factors (e.g., VEGF-A, VEGF-A145, VEGF- A165, VEGF-C, VEGF-D, PIGF-2), fibroblast growth factor (FGF), galectin, hepatocyte growth factor (FIGF), platelet derived growth factor (PDGF), transforming growth factor (TGF)-beta, androgens, estrogens, and somatostatin analogs.
- progestogen progestin
- corticosteroids e.g., prednisolone, methylprednisolone, dexamethasone
- hormonal antagonists include hormone synthesis inhibitors such as aromatase inhibitors and gonadotropin-releasing hormone (GnRFI)s agonists (e.g., leuprolide, goserelin, triptorelin, histrelin) including analogs thereof. Also included are hormone receptor antagonist such as selective estrogen receptor modulators (SERMs; e.g., tamoxifen, raloxifene, toremifene) and anti-androgens (e.g., flutamide, bicalutamide, nilutamide).
- SERMs selective estrogen receptor modulators
- SERMs selective estrogen receptor modulators
- hormonal pathway inhibitors such as antibodies directed against hormonal receptors.
- examples include inhibitors of the the IGF receptor (e.g., IGF-IR1) such as cixutumumab, dalotuzumab, figitumumab, ganitumab, istiratumab, and robatumumab; inhibitors of the vascular endothelial growth factor receptors 1, 2 or 3 (VEGFR1, VEGFR2 or VEGFR3) such as alacizumab pegol, bevacizumab, icrucumab, ramucirumab; inhibitors of the TGF-beta receptors Rl, R2, and R3 such as fresolimumab and metelimumab; inhibitors of c-Met such as naxitamab; inhibitors of the EGF receptor such as cetuximab, depatuxizumab mafodotin, futuximab, imgatuzumab, laprituximab em
- hormonal therapeutic agents described herein can be combined with any one or more of the various anti-NRP2 antibodies (including antigen-binding fragments thereof) described herein, and used according to any one or more of the methods or compositions described herein.
- kinase inhibitors include, without limitation, adavosertib, afanitib, aflibercept, axitinib, bevacizumab, bosutinib, cabozantinib, cetuximab, cobimetinib, crizotinib, dasatinib, entrectinib, erdafitinib, erlotinib, fostamitinib, gefitinib, ibrutinib, imatinib, lapatinib, lenvatinib, mubritinib, nilotinib, panitumumab, pazopanib, pegaptanib, ponatinib, ranibizumab, regorafenib, ruxoli
- Exemplary PI3 kinase inhibitors include alpelisib, buparlisib, copanlisib, CU DC-907, dactolisib, duvelisib, GNE-477, idelasib, IPI-549, LY294002, ME-401, perifosine, PI-103, pictilisib, PWT33597, RP6503, taselisib, umbralisib, voxtalisib, wortmannin, and XL147
- Embodiments of the present disclosure relate in part to the discovery that human histidyl- tRNA synthetase (HRS) polypeptides have unexpected biological properties which are relevant to treating a broad range of diseases and conditions, and that certain of these properties relate to the interactions between HRS and human neuropilin 2 (NRP2). Accordingly, antibodies directed against human NRP2, which interfere with the binding between NRP2 and NRP2 ligands and/or modulate NRP2 receptor signaling can be used as standalone therapies in the treatment of diseases, including NRP2-associated diseases, or in combination with other therapeutic agents as described herein.
- HRS histidyl- tRNA synthetase
- Certain embodiments therefore include methods of treating, ameliorating the symptoms of, and/or reducing the progression of, a disease or condition in a subject in need thereof, comprising administering to the subject at least one antibody or antigen-binding fragment thereof that specifically binds to a human neuropilin-2 (NRP2) polypeptide.
- the at least one antibody or antigen-binding fragment thereof antagonizes the binding/signaling activity between the NRP2 polypeptide and the at least one NRP2 ligand.
- the at least one antibody or antigen-binding fragment thereof mimics or otherwise enhances one or more signaling activities of the NRP2/NRP2 ligand interaction, for example, by acting as an agonist antibody.
- the anti-NRP2 antibody binds selectively to the NRP2a isoform (e.g., variants 1, 2, and/or 3 of Table Nl) of NRP2, and does not substantially bind to the NRP2b isoform (e.g., variants 4 and/or 5 of Table Nl). In some embodiments the anti-NRP2 antibody binds selectively to the NRP2b isoform (e.g., variants 4 and/or 5 of Table Nl), and does not substantially bind to the NRP2a isoform (e.g., variants 1, 2, and/or 3 of Table Nl). Such binding characteristics can apply to any one or more of the embodiments described herein.
- the at least one antibody or antigen-binding fragment thereof selectively modulates the binding and/or signaling of VEGF-C or related NRP2 ligands to or via an NRP2 polypeptide.
- such antibodies or antigen-binding fragment thereof do not substantially block the interaction of semaphorins to an NRP2 polypeptide.
- such antibodies or antigen-binding fragment thereof are antagonistic antibodies with respect to VEGF-C signaling via an NRP2 polypeptide.
- such antibodies are agonistic antibodies with respect to semaphorin 3F signaling via an NRP2 polypeptide.
- the at least one antibody or antigen-binding fragment thereof antagonizes the binding/signaling activity between an NRP2 polypeptide and VEGFR2 or VEGFR3 without substantially modulating the binding/signaling activity between an NRP2 polypeptide and a plexin receptor and/or a semaphorin.
- Some embodiments comprise administering at least one anti-NRP2 antibody to a subject in an amount and at a frequency sufficient to achieve an average, sustained blood plasma concentration of soluble NRP2 of about or less than about 500 pM, 400 pM, 300 pM, 200 pM, lOOpM, 50pm, 40pM, 30 pM, 20 pM, or lOpM. Certain embodiments comprise administering at least one anti-NRP2 antibody in an amount and at a frequency sufficient to achieve a reduction in the circulating levels of FIRS:NRP2 complexes, for example, a reduction of about or at least about 5, 10, 15, 20, 25, 30, 35, 40, 45, 50, 60, 70, 80, 90, 95, 99, or 100%.
- Some embodiments include administering the at least one anti-NRP2 antibody in an amount and at a frequency sufficient to achieve a steady state concentration, or average circulating concentration, of the at least one anti- NRP2 antibody of between about 1 nM and about 1 mM, between about 1 nM and about 100 nM, between about 1 nM and about 10 nM, or between about 1 nM and about 3 mM.
- the disease is or condition is an NRP2-associated disease or condition.
- the NRP2-associated disease or condition is selected from one or more of cancer and diseases and pathways associated with cancer, including cancer cell growth, initiation, migration, adhesion, invasion, chemoresistance, and/or metastasis; diseases associated with inflammation, autoimmunity, and related inflammatory diseases, including diseases associated with inappropriate immune cell activation or migration such as Graft versus host disease (GVFID); diseases associated with lymphatic development, lymphangiogenesis, and lymphatic damage, including, for example, edema, lymphedema, secondary lymphedema, inappropriate fat absorption and deposition, excess fat deposition, and vascular permeability; diseases associated with infections, including latent infections; diseases associated with allergic disorders/diseases, allergic responses, including, for example, chronic obstructive pulmonary disorder (COPD), neutrophilic asthma, antineutrophil cytoplasmic antibody (ANCA)-associated systemic vasculitis, systemic lupus ery
- COPD chronic o
- the disease is a cancer.
- upregulation of NRP2 expression is associated with tumorigenesis, and in particular tumor metastasis and development of chemoresistance, and is correlated with more aggressive disease in several tumor types.
- the semaphorin/plexin/neuropilin signaling axis influences many of the hallmarks of cancer (see, for example, Franzolin and Tamagnone Int. J. Mol. Sci. 20, 377; doi:10.3390/ijms20020377, 2019); Nasarre et al., OncoTargets and Therapy 2014:7 1663-1687; Neufeld et al., Cold Spring Harb Perspect Med. 2:a006718, 2012).
- Semaphorin 3F Semaphorin 3F (SEMA3F), which was initially identified as tumor suppressor gene in lung cancer, and is consistently downregulated in highly metastatic tumor cells, including prostate, bladder, and melanoma cells in vitro and in vivo. Consistent with these studies, increased expression of NRP2 in prostate cancer cells is also induced by the loss of the tumor suppressor gene phosphatase and tensin homolog (PTEN), and its expression correlates with Gleason grade (see, for example, Zhao et al., Thoracic Cancer 8: 203-213, 2017). Additionally, P53 mutations upregulate NRP2 expression via suppression of DLX2 transcription leading to increased cell mobility.
- SEMA3F Semaphorin 3F
- TGF-b signaling is involved in the expression of NRP2b, and up-regulation of EMT in cancer, which may explain why in advanced tumors, higher production of TGF-b is positively associated with tumor aggressiveness and poor prognosis (see, for example, Malfettone et al., Cancer Lett. 392:39-50, 2017).
- Certain embodiments thus include methods of treating ameliorating the symptoms of, or inhibiting the progression of, a cancer in a subject in need thereof, comprising administering to the subject at least one antibody or antigen-binding fragment thereof that specifically binds to a human NRP2 polypeptide (an anti-NRP2 antibody), and which modulates (e.g., interferes with) binding of the human NRP2 polypeptide to a NRP2 ligand (for example, an NRP2 ligand from Table N2 or Table N3 and/or a human HRS polypeptide from Table HI).
- a NRP2 ligand for example, an NRP2 ligand from Table N2 or Table N3 and/or a human HRS polypeptide from Table HI.
- Certain embodiments include reducing or preventing the re-emergence of a cancer in a subject in need thereof, for example, a metastatic cancer and/or a chemoresistant cancer, wherein administration of the therapeutic composition enables generation of an immune memory to the cancer.
- an anti-NRP2 antibody enhances the immune response to the cancer by about, or at least about, 5, 10, 15, 20, 25, 30, 35, 40, 45, 50, 60, 70, 80, 90, 100, 200, 300, 400, 500, 600, 700, 800, 900, 1000, 2000% or more, relative to an untreated control.
- Exemplary immune responses include increasing or enhancing immune cell invasion of a solid tumor, and increasing the biological activity against the cancer.
- an anti-NRP2 antibody enhances an adaptive immune response to the cancer, and in some embodiments, an anti-NRP2 antibody enhances an innate immune response to the cancer. In some-instances, an anti-NRP2 antibody directly or indirectly enhances a T-cell-mediated response to the cancer. In some-instances, an anti-NRP2 antibody enhances a B-cell-mediated or antibody- mediated response to the cancer. In some-instances, an anti-NRP2 antibody modulates a macrophage responses to the cancer. In some-instances, an anti-NRP2 antibody modulates immune cell, or cancer autophagy. In some-instances, an anti-NRP2 antibody modulates immune cell phagocytosis. In some-instances, an anti-NRP2 antibody modulates cancer cell apoptosis. In some- instances, an anti-NRP2 antibody modulates immune cell efferocytosis and/or cancer cell autophagy.
- an anti-NRP2 antibody enhances macrophage responses to the cancer. In some embodiments, an anti-NRP2 inhibits macrophage responses to the cancer. In some embodiments of the anti-NRP2 antibody, the antibody enhances autophagy. In some embodiments, an anti-NRP2 inhibits autophagy. In some embodiments, an anti-NRP2 enhances phagocytosis. In some embodiments, an anti-NRP2 inhibits phagocytosis. In some embodiments, an anti-NRP2 enhances apoptosis. In some embodiments of the anti-NRP2 antibody, the antibody inhibits apoptosis. In some embodiments, an anti-NRP2 antibody enhances efferocytosis. In some embodiments, an anti-NRP2 inhibits efferocytosis.
- an anti-NRP2 antibody reduces cancer initiation, cancer cell migration, adhesion, or cancer cell metastasis by about or at least about 5, 10, 15, 20, 25, 30, 35, 40, 45, 50, 60, 70, 80, 90, 100, 200, 300, 400, 500, 600, 700, 800, 900, 1000, 2000% or more relative to an untreated control.
- an anti-NRP2 antibody reduces cancer mediated lymphangiogenesis by about or at least about 5, 10, 15, 20, 25, 30, 35, 40, 45, 50, 60, 70, 80, 90, 100, 200, 300, 400, 500, 600, 700, 800, 900, 1000, 2000% or more relative to an untreated control.
- the at least one anti-NRP2 antibody reduces the rate of in vitro growth of the cancer (for example, cancer cells isolated from a biopsy or other sample grown in vitro) by about or at least about 5, 10, 15, 20, 25, 30, 35, 40, 45, 50, 60, 70, 80, 90, 100, 200, 300,
- the at least one anti-NRP2 antibody reduces the adhesiveness of the cancer (for example, cancer cells isolated from a biopsy or other sample grown in vitro) to a substrate by about or at least about, 5, 10, 15, 20, 25, 30, 35, 40, 45, 50, 60, 70, 80, 90, 100, 200,
- the substrate comprises laminin.
- the at least one anti-NRP2 antibody reduces the invasiveness of the cancer (for example, cancer cells isolated from a biopsy or other sample grown in vitro) by about or at least about 5, 10, 15, 20, 25, 30, 35, 40, 45, 50, 60, 70, 80, 90, 100, 200, 300, 400, 500, 600, 700, 800, 900, 1000, 2000% or more relative to an untreated control.
- the cancer for example, cancer cells isolated from a biopsy or other sample grown in vitro
- the at least one anti-NRP2 antibody reduces the invasiveness of the cancer (for example, cancer cells isolated from a biopsy or other sample grown in vitro) by about or at least about 5, 10, 15, 20, 25, 30, 35, 40, 45, 50, 60, 70, 80, 90, 100, 200, 300, 400, 500, 600, 700, 800, 900, 1000, 2000% or more relative to an untreated control.
- the at least one anti-NRP2 antibody inhibits the rate of migration or motility of the cancer or a migratory cell (for example, cancer or immune cells isolated from a biopsy or other sample grown in vitro) by about or at least about 5, 10, 15, 20, 25, 30, 35, 40, 45, 50, 60, 70, 80, 90, 100, 200, 300, 400, 500, 600, 700, 800, 900, 1000, 2000% or more relative to an untreated control.
- a migratory cell for example, cancer or immune cells isolated from a biopsy or other sample grown in vitro
- the at least one anti-NRP2 antibody inhibits the rate of autophagy or endosome maturation (for example, endosome acidification) of the cancer or associated immune cells by about or at least about 5, 10, 15, 20, 25, 30, 35, 40, 45, 50, 60, 70, 80, 90, 100, 200, 300, 400, 500, 600, 700, 800, 900, 1000, 2000% or more relative to an untreated control.
- the at least one anti-NRP2 antibody enhances the susceptibility of the cancer to an additional agent (for example, chemotherapeutic agent, hormonal therapeutic agent, and or kinase inhibitor) by about or at least about 5, 10, 15, 20, 25, 30, 35, 40, 45, 50, 60, 70, 80, 90, 100, 200, 300, 400, 500, 600, 700, 800, 900, 1000, 2000% or more relative to the additional agent alone.
- an additional agent for example, chemotherapeutic agent, hormonal therapeutic agent, and or kinase inhibitor
- the at least one anti-NRP2 antibody enhances an anti-tumor and/or immunostimulatory activity of a cancer immunotherapy agent by about or at least about 5, 10, 15, 20, 25, 30, 35, 40, 45, 50, 60, 70, 80, 90, 100, 200, 300, 400, 500, 600, 700, 800, 900, 1000, 2000% or more, relative to the cancer immunotherapy agent alone.
- combination therapies for treating cancers including methods of treating ameliorating the symptoms of, or inhibiting the progression of, a cancer in a subject in need thereof, comprising administering to the subject at least one antibody or antigen-binding fragment thereof that specifically binds to a human NRP2 polypeptide (an anti-NRP2 antibody) in combination with at least one additional agent, for example, a cancer immunotherapy agent, a chemotherapeutic agent, a hormonal therapeutic agent, and/or a kinase inhibitor.
- additional agent for example, a cancer immunotherapy agent, a chemotherapeutic agent, a hormonal therapeutic agent, and/or a kinase inhibitor.
- Exemplary cancer immunotherapy agents, chemotherapeutic agents, hormonal therapeutic agents, and kinase inhibitors are described elsewhere herein.
- an anti-NRP2 antibody and the at least one additional agent are administered separately, for example, in separate therapeutic compositions and at the same or different times. In some embodiments, an anti-NRP2 antibody and the at least one additional agent are administered as part of the same therapeutic composition, at the same time.
- Particular methods employ one or more anti-NRP2 antibodies, or antigen-binding fragments thereof, as part of (i.e., in addition to) a combination therapy regimen.
- exemplary combination regiments are provided in Table Ml below.
- the methods and therapeutic compositions described herein increase median survival time of a subject by 4 weeks, 5 weeks, 6 weeks, 7 weeks, 8 weeks, 9 weeks, 10 weeks, 15 weeks, 20 weeks, 25 weeks, 30 weeks, 40 weeks, or longer. In certain embodiments, the methods and therapeutic compositions described herein (for example, anti-NRP2 antibody, alone or in combination with at least one additional agent) increase median survival time of a subject by 1 year, 2 years, 3 years, or longer.
- the methods and therapeutic compositions described herein increase progression-free survival by 2 weeks, 3 weeks, 4 weeks, 5 weeks, 6 weeks, 7 weeks, 8 weeks, 9 weeks, 10 weeks or longer. In certain embodiments, the methods or therapeutic compositions described herein increase progression-free survival by 1 year, 2 years, 3 years, or longer.
- the methods and therapeutic compositions described herein are sufficient to result in tumor regression, as indicated by a statistically significant decrease in the amount of viable tumor, for example, at least a 10%, 20%, 30%, 40%, 50% or greater decrease in tumor mass, or by altered (e.g., decreased with statistical significance) scan dimensions.
- the methods and therapeutic compositions described herein are sufficient to result in stable disease.
- the methods and therapeutic compositions described herein are sufficient to result in clinically relevant reduction in symptoms of a particular disease indication known to the skilled clinician.
- an anti-NRP2 antibody increases, complements, or otherwise enhances the anti-tumor and/or immunostimulatory activity of the cancer immunotherapy agent, relative to the cancer immunotherapy agent alone.
- an anti-NRP2 antibody enhances the anti-tumor and/or immunostimulatory activity of the cancer immunotherapy agent by about, or at least about, 5, 10, 15, 20, 25, 30, 35, 40, 45, 50, 60, 70, 80, 90, 100, 200, 300, 400, 500, 600, 700, 800, 900, 1000, 2000% or more, relative to the cancer immunotherapy agent alone.
- the cancer is a primary cancer, i.e., a cancer growing at the anatomical site where tumor progression began and yielded a cancerous mass.
- the cancer is a secondary or metastatic cancer, i.e., a cancer which has spread from the primary site or tissue of origin into one or more different sites or tissues.
- the cancer expresses or overexpresses NRP2.
- the subject or patient has a cancer selected from one or more of melanoma (e.g., metastatic melanoma), an epithelial or epithelial-derived tumor, pancreatic cancer, bone cancer, prostate cancer, small cell lung cancer, non-small cell lung cancer (NSCLC), mesothelioma, leukemia (e.g., lymphocytic leukemia, chronic myelogenous leukemia, acute myeloid leukemia, relapsed acute myeloid leukemia), lymphoma, hepatoma (hepatocellular carcinoma or HCC), sarcoma, B-cell malignancy, breast cancer (for example, estrogen receptor positive (ER+), estrogen receptor negative (ER-), Her2 positive (Her2+), Her2 negative (Her2-), or a combination thereof, e.g., ER+/Her2+, ER+/Her2-, ER- /Her2+, or ER-/Her2-; or "triple negative" breast cancer (for example
- the cancer or tumor is a metastatic cancer, for example, a metastatic cancer that expresses NRP2a and/or NRP2b.
- exemplary metastatic cancers include, without limitation, bladder cancers which have metastasized to the bone, liver, and/or lungs; breast cancers which have metastasized to the bone, brain, liver, and/or lungs; colorectal cancers which have metastasized to the liver, lungs, and/or peritoneum; kidney cancers which have metastasized to the adrenal glands, bone, brain, liver, and/or lungs; lung cancers which have metastasized to the adrenal glands, bone, brain, liver, and/or other lung sites; melanomas which have metastasized to the bone, brain, liver, lung, and/or skin/muscle; ovarian cancers which have metastasized to the liver, lung, and/or peritoneum; pancreatic cancers which have metastasized to the liver, lung, and/or peritoneum; pancreatic cancers which have metastasized
- the subject has one or more biomarkers (e.g., increased PD-1 or PD-L1 levels in cells such as cancer cells or cancer-specific CTLs) that make the suitable for PD-1 or PD-L1 inhibitor therapy.
- biomarkers e.g., increased PD-1 or PD-L1 levels in cells such as cancer cells or cancer-specific CTLs
- the subject has increased fractions of programmed cell death 1 high/cytotoxic T lymphocyte-associated protein 4 high (e.g., PD-l hl CTLA- 4 hi ) cells within a tumor-infiltrating CD8+ T cell subset (see, e.g., Daud et al J Clin Invest. 126:3447- 3452, 2016).
- the subject has increased levels of Bim (B cell lymphoma 2-interacting (Bcl2-interacting) mediator) in circulating tumor-reactive (e.g., PD- l + CDlla hl CD8 + ) T cells, and optionally has metastatic melanoma (see, e.g., Dronca et al., JCI Insight. May 5; 1(6): e86014, 2016).
- Bim B cell lymphoma 2-interacting (Bcl2-interacting) mediator
- circulating tumor-reactive e.g., PD- l + CDlla hl CD8 +
- metastatic melanoma see, e.g., Dronca et al., JCI Insight. May 5; 1(6): e86014, 2016.
- Certain specific combinations include an anti-NRP2 antibody and a PD-L1 antagonist or inhibitor, for example, atezolizumab (MPDL3280A), avelumab (MSB0010718C), and durvalumab (MEDI4736), for treating a cancer selected from one or more of colorectal cancer, melanoma, breast cancer, non-small-cell lung carcinoma, bladder cancer, and renal cell carcinoma.
- a PD-L1 antagonist or inhibitor for example, atezolizumab (MPDL3280A), avelumab (MSB0010718C), and durvalumab (MEDI4736), for treating a cancer selected from one or more of colorectal cancer, melanoma, breast cancer, non-small-cell lung carcinoma, bladder cancer, and renal cell carcinoma.
- Some specific combinations include an anti-NRP2 antibody and a PD-1 antagonist, for example, nivolumab, for treating a cancer selected from one or more of Hodgkin's lymphoma, melanoma, non-small cell lung cancer, hepatocellular carcinoma, renal cell carcinoma, and ovarian cancer.
- a PD-1 antagonist for example, nivolumab, for treating a cancer selected from one or more of Hodgkin's lymphoma, melanoma, non-small cell lung cancer, hepatocellular carcinoma, renal cell carcinoma, and ovarian cancer.
- Particular specific combinations include an anti-NRP2 antibody and a PD-1 antagonist, for example, pembrolizumab, for treating a cancer selected from one or more of melanoma, non-small cell lung cancer, small cell lung cancer, head and neck cancer, and urothelial cancer.
- a PD-1 antagonist for example, pembrolizumab
- pembrolizumab for treating a cancer selected from one or more of melanoma, non-small cell lung cancer, small cell lung cancer, head and neck cancer, and urothelial cancer.
- Certain specific combinations include an anti-NRP2 antibody and a CTLA-4 antagonist, for example, ipilimumab and tremelimumab, for treating a cancer selected from one or more of melanoma, prostate cancer, lung cancer, and bladder cancer.
- a CTLA-4 antagonist for example, ipilimumab and tremelimumab, for treating a cancer selected from one or more of melanoma, prostate cancer, lung cancer, and bladder cancer.
- Some specific combinations include an anti-NRP2 antibody and an IDO antagonist, for example, indoximod (NLG-8189), 1-methyl-tryptophan (1MT), b-Carboline (norharmane; 9H- pyrido[3,4-b]indole), rosmarinic acid, or epacadostat, for treating a cancer selected from one or more of metastatic breast cancer and brain cancer optionally Glioblastoma Multiforme, glioma, gliosarcoma or malignant brain tumor.
- IDO antagonist for example, indoximod (NLG-8189), 1-methyl-tryptophan (1MT), b-Carboline (norharmane; 9H- pyrido[3,4-b]indole), rosmarinic acid, or epacadostat, for treating a cancer selected from one or more of metastatic breast cancer and brain cancer optionally Glioblastoma Multiforme, glioma, gliosar
- Certain specific combinations include an anti-NRP2 antibody and the cytokine INF-a for treating melanoma, Kaposi sarcoma, and hematologic cancers. Also included is the combination of an anti-NRP2 antibody and IL-2 (e.g., Aldesleukin) for treating metastatic kidney cancer or metastatic melanoma.
- IL-2 e.g., Aldesleukin
- Some specific combinations include an anti-NRP2 antibody and a T-cell based adoptive immunotherapy, for example, comprising CAR-modified T-cells targeted against CD-19, for treating hematological cancers such as acute lymphoblastic leukemia (ALL), chronic lymphocytic leukemia (CLL), and B-cell neoplasms (see, e.g., Maude et al., 2015, supra; Lorentzen and Straten, Scand J Immunol. 82:307-19, 2015; and Ramos et al., Cancer J. 20:112-118, 2014).
- ALL acute lymphoblastic leukemia
- CLL chronic lymphocytic leukemia
- B-cell neoplasms see, e.g., Maude et al., 2015, supra; Lorentzen and Straten, Scand J Immunol. 82:307-19, 2015; and Ramos et al., Cancer J. 20:112-118, 2014.
- a combination therapy described herein can be administered to a subject before, during, or after other therapeutic interventions, including symptomatic care, radiotherapy, surgery, transplantation, hormone therapy, photodynamic therapy, antibiotic therapy, or any combination thereof.
- Symptomatic care includes administration of corticosteroids, to reduce cerebral edema, headaches, cognitive dysfunction, and emesis, and administration of anti-convulsants, to reduce seizures.
- Radiotherapy includes whole-brain irradiation, fractionated radiotherapy, and radiosurgery, such as stereotactic radiosurgery, which can be further combined with traditional surgery.
- Certain embodiments include the use of the anti-NRP2 antibodies described herein to modulate lymphangiogenesis, and treat related conditions such as lymphedema or tumor metastasis.
- the lymphatic system consists of networks of interconnected capillaries, collecting vessels and lymph nodes that absorb, collect and transport the fluid and protein filtered from the blood vascular system. This system provides a critical homeostatic function: in humans, lymphatic vessels return >4 liters of fluid and a substantial amount of protein per day back into the great veins of the neck.
- Lymphatic vascular dysfunction results in the accumulation of excess fluid (edema) in the interstitium.
- lymphedema is typically not life-threatening, it has serious health consequences, including pain, immobility, fibrosis, inflammation, adipose tissue accumulation, and tissue damage. Because the lymphatic system is also a critical component of immune responses, lymphedema is typically accompanied by an increased risk of infection and other immune system problems.
- Lymphangiogenesis is the formation of new lymphatic vessels from preexisting lymphatic vessels and is associated with diverse pathological conditions including metastatic dissemination, graft rejection (e.g., cornea, kidney and heart), type 2 diabetes, obesity, hypertension, and lymphedema (See, e.g. Alitalo et al. Nature 438:946-953, 2005; Karaman et al. J Clin Invest 124:922- 928, 2014; Kim et al., J Clin Invest 124:936-942, 2014; Maby-EI Hajjami et al., Histochem Cell Biol 130:1063-107, 2008; Machnik et al., Nat Med 15:545-552; Mortimer et al., 2014. J Clin Invest 124:915-921; Skobe et al., 2009. Nat Med 15:993-994).
- Lymphatic vessel invasion in and around a primary tumor compared to invasion of blood vessels is a prognostic marker of the aggressiveness of various types of cancers. Growth of lymphatic vessels is also involved in graft rejection (Dietrich, T., et al., J Immunol 184:535-539, 2010, Hall et al., Arch Otolaryngol Head Neck Surg 129:716-719, 2003.; Maula et al., Cancer Res 63:1920-1926, 2003; Miyata et al., J Urol 176:348-353, 2006; Saad et al., Mod Pathol 19:1317-1323, 2006; Schoppmann et al., Ann Surg 240:306-312, 2004; Zeng et al., Prostate 65:222-230, 2005).
- lymphatics in the pathogenesis of numerous diseases, there has been little progress in the development of anti-lymphangiogenic agents compared to the abundance of anti-angiogenic agents that have entered clinical trials. Therefore, the development of additional lymphangiogenesis inhibitors is of interest for the treatment of a range of conditions, including lymphedema and cancer metastasis.
- Anti-lymphangiogenic agents are useful, for example, for treatment of debilitating diseases of the eye, where the growth of lymphatic vessels is the major reason of corneal graft rejection and a major contributor to neovascularization associated with age related macular degeneration (Dietrich, T., et al., J Immunol 184:535-539, 2010).
- penetrating keratoplasty is the most common form of solid tissue transplantation, with approximately 40,000 corneal transplantations performed each year in the United States.
- the success rate of penetrating keratoplasty is as high as 90% for uncomplicated first grafts performed in avascular low-risk beds.
- the rejection rate of the corneal grafts placed in high-risk vascularized host beds is extremely high (70% to 90%).
- Anti-lymphangiogenesis drugs are useful also for treatment of dry eye disease.
- Significant upregulation of pro-lymphangiogenic factors e.g., VEGF-C, VEGF-D, and VEGFR-3 and selective growth of lymphatic vessels without concurrent growth of blood vessels has been demonstrated in corneas with dry eye disease (Goyal et al., Arch Ophthalmol 128:819-824, 2010).
- Dry eye disease is an immune-mediated disorder affecting about 5 million Americans. It severely impacts the vision- related quality of life and the symptoms can be debilitating. The current therapeutic options for dry eye disease are limited, mostly palliative, and expensive. Therefore, development of lymphangiogenesis inhibitors is of therapeutic value for treatment of dry eye disease.
- metastases are responsible for the vast majority (90%) of deaths from solid tumors (Gupta and Massague, Cell 127, 679-695, 2006).
- the complex process of metastasis involves a series of distinct steps including detachment of tumor cells from the primary tumor, intravasation of tumor cells into lymphatic or blood vessels, and extravasation and growth of tumor cells in secondary sites.
- Analysis of regional lymph nodes in many tumor types suggests that the lymphatic vasculature is an important route for the dissemination of human cancers.
- the presence of tumor cells in lymph nodes is the most important adverse prognostic factor.
- lymphangiogenesis can be induced by solid tumors and can promote tumor spread.
- anti-NRP2 antibodies or antigen-binding fragments thereof represent powerful new tools for the development of both pro and anti- lymphangiogenic therapies.
- differential effects may be mediated for example, via the uses of different anti-NRP2 compositions, differential NRP2a or NRP2b selectivity, differential dosing, differential treatment duration, or the appropriate use of additional co-factors, such as, for example, VEGF-C, or Semaphorin 3F and/or 3G.
- the at least one antibody or antigen-binding fragment thereof selectively modulates the binding and/or signaling of VEGF-C or related NRP2 ligands to or via an NRP2 polypeptide.
- such antibodies or antigen-binding fragment thereof do not substantially block the interaction of semaphorins to an NRP2 polypeptide.
- the at least one antibody or antigen-binding fragment thereof selectively modulates the binding and/or signaling of Semaphorin 3F or related NRP2 ligands to or via an NRP2 polypeptide.
- such antibodies do not substantially block the interaction of VEGF-C to an NRP2 polypeptide.
- such antibodies selectively modulate both the binding of VEGF-C or related NRP2 ligands and semaphorins to an NRP2 polypeptide.
- such antibodies are agonistic antibodies with respect to VEGF-C signaling. In some aspects, such antibodies are antagonistic antibodies with respect to VEGF-C signaling. In some embodiments, such antibodies are agonistic antibodies with respect to semaphorin 3F signaling. In some aspects, such antibodies are antagonistic antibodies with respect to semaphorin 3F signaling.
- the at least one antibody or antigen-binding fragment thereof antagonizes the binding/signaling activity between an NRP2 polypeptide and VEGFR2 or VEGFR3 without substantially modulating the binding/signaling activity between the NRP2 polypeptide and a plexin receptor and/or a semaphorin. In some embodiments, the at least one antibody or antigen binding fragment thereof antagonizes the binding/signaling activity between an NRP2 polypeptide and a plexin receptor and/or a semaphorin without substantially modulating the binding/signaling activity between the NRP2 polypeptide and VEGFR2, VEGFR3, and/or VEGF-C.
- Certain embodiments thus include methods of treating ameliorating the symptoms of, or inhibiting the progression of, lymphangiogenesis, or neovascularization in a subject in need thereof, comprising administering to the subject at least one antibody or antigen-binding fragment thereof that specifically binds to a human NRP2 polypeptide, and which modulates (e.g., interferes with) binding of the human NRP2 polypeptide to VEGF-C, VEGFR1, VEGFR2, and/or VEGFR3.
- Some embodiments include the use of the anti-NRP2 antibodies described herein to modulate smooth muscle contractility, and treat related conditions.
- Reduced smooth muscle (SM) contractility in the bladder can stem from numerous etiologies including partial obstruction secondary to benign prostatic hyperplasia (BPH), posterior urethral valves, diabetes mellitus, multiple sclerosis, spinal cord injury, or idiopathic causes. (See, e.g., Drake et al., Nat Rev Urol. ll(8):454-464, 2014).
- BPH benign prostatic hyperplasia
- posterior urethral valves the bladder contracts against an obstructed outlet.
- the initial response is adaptive, involving a compensatory phase of SM hypertrophy that enables increased force generation to overcome the increased outlet resistance.
- Nrp2 may represent a novel pharmacological target for maintenance or restoration of detrusor contractility in the decompensated bladder.
- NRP2 axis represents a potentially novel pharmacologic target for restoration of SM contractility in partial bladder outlet obstruction syndromes, and provide an important therapeutic opportunity for the development of antibody- based modulators of NRP2 function.
- the anti-NRP2 antibodies described herein could provide new therapies to modulate smooth muscle contractility, including for example, the treatment of reduced smooth muscle (SM) contractility in the bladder, and more specifically syndromes associated with partial bladder outlet obstruction syndromes.
- SM smooth muscle
- Certain embodiments thus include methods of treating ameliorating the symptoms of, or inhibiting the progression of partial bladder outlet obstruction syndromes in a subject in need thereof, comprising administering to the subject at least one antibody or antigen-binding fragment thereof that specifically binds to a human NRP2 polypeptide (an anti-NRP2 antibody), and which modulates (e.g., interferes with) binding of the human NRP2 polypeptide to a NRP2 ligand (for example, an NRP2 ligand from Table N2 or Table N3).
- a human NRP2 polypeptide an anti-NRP2 antibody
- a NRP2 ligand for example, an NRP2 ligand from Table N2 or Table N3
- Certain embodiments also include methods of modulating (e.g., increasing, reducing) smooth muscle contractility in a subject in need thereof, comprising administering to the subject an anti-NRP2 antibody, or antigen-binding fragment thereof, or therapeutic composition provided herein. Certain embodiments include treating, ameliorating the symptoms of, and/or reducing the progression of, reduced smooth muscle contractility in a subject in need thereof, comprising administering to the subject an anti-NRP2 antibody or antigen-binding fragment thereof, or therapeutic composition provided herein.
- the subject has, and/or is selected for treatment based on having, a disease associated with increased levels or expression of at least one NRP2 ligand (for example, an NRP2 ligand from Table N2 or Table N3 and/or an HRS polypeptide from Table HI) and/or a coding mRNA thereof relative to a healthy control.
- NRP2 ligand for example, an NRP2 ligand from Table N2 or Table N3 and/or an HRS polypeptide from Table HI
- a coding mRNA thereof relative to a healthy control.
- the levels of the at least one NRP2 ligand in the diseases subject, cells, or tissue are about or at least about 1.5, 2, 3, 4, 5, 6, 7, 8, 9, 10, 15, 20, 30, 40, 50, 60, 70, 80, 90, 100, 1000 or more times the levels of the at least one NRP2 ligand in a healthy control.
- the subject has, and/or is selected for treatment based on having, a cancer which has increased levels or expression of at least one NRP2 ligand (for example, an NRP2 ligand from Table N2 or Table N3 and/or an HRS polypeptide from Table HI) and/or a coding mRNA thereof relative to a non-cancerous control cell or tissue.
- the levels of the at least one NRP2 ligand in the cancer cells or tissue are about or at least about 1.5, 2, 3, 4, 5, 6, 7, 8, 9, 10, 15, 20, 30, 40, 50, 60, 70, 80, 90, 100, 1000 or more times the levels of the NRP2 ligand in a non-cancerous control or standard.
- certain embodiments include methods of selecting a subject for treatment, comprising (i) detecting increased expression levels of at least one NRP2 ligand (for example, an NRP2 ligand from Table N2 or Table N3 and/or an HRS polypeptide from Table HI) and/or coding mRNA in the subject relative to a control or reference, and (ii) administering to the subject a therapeutic composition comprising at least one anti-NRP2-antibody or antigen-binding fragment thereof, as described herein.
- the HRS polypeptide is a splice variant of full-length HRS.
- the HRS splice variant is selected from one or more of HisRSNl, HisRSN2, HisRSN3, HisRSN4, HisRSN5, HisRSCl, HisRSC2, HisRSC3, HisRSC4, HisRSC5, HisRSC6, HisRSC7, HisRSC8, and HisRSC9.
- the subject has, and/or is selected for treatment based on having, increased circulating or serum levels of a soluble neuropilin 2 (NRP2) polypeptide (selected, for example, from Table Nl), either bound to an HRS polypeptide or free, relative to the levels of a healthy or matched control population of subject(s).
- NRP2 soluble neuropilin 2
- the circulating or serum levels are about or at least about 10, 20, 30, 50, 100, 200, 300, 400, 500, 600, 700, 800, 900, 1000, 1100, 1200, 1300, 1400, 1500, 1600, 1700, 1800, 1900, 2000, 3000, 4000, 5000 pM of the soluble NRP2 polypeptide, or the circulating or serum levels are about 30-50, 50-100, 100- 2000, 200-2000, 300-2000, 400-2000, 500-2000, 600-2000, 700-2000, 800-2000, 900-2000, 1000- 2000, 2000-3000, 3000-4000, 4000-5000 pM of the soluble NRP2 polypeptide.
- the subject has, and/or is selected for treatment based on having, a disease associated with increased levels or expression of an NRP2 polypeptide (optionally selected from Table Nl) and/or a coding mRNA thereof relative to a healthy control (e.g., an NRP2-associated disease).
- the NRP2 polypeptide is an NRP2a isoform (e.g., variants 1, 2, and/or 3 of Table Nl) or a fragment thereof.
- the NRP2 polypeptide is an NRP2b isoform (e.g., variants 4 and/or 5 of Table Nl) or a fragment thereof.
- the levels of the NRP2 polypeptide in the diseased subject, cells, or tissue are about or at least about 1.5, 2, 3, 4, 5, 6, 7, 8, 9, 10, 15, 20, 30, 40, 50, 60, 70, 80, 90, 100 or more times the levels of NRP2 polypeptide in a healthy control.
- the subject has, and/or is selected for treatment based on having, a cancer which has increased levels or expression of a NRP2 polypeptide (selected, for example, from Table Nl) and/or a coding mRNA thereof relative to a control cell or tissue, optionally relative to a non-cancerous cell or tissue of the same type as the cancer.
- the levels of the NRP2 polypeptide in the cancer cells or tissue are about or at least about 1.5, 2, 3, 4, 5, 6, 7, 8, 9, 10, 15,
- Some embodiments thus include methods of selecting a subject for treatment, comprising (i) detecting increased expression levels of a NRP2 polypeptide and/or a coding mRNA thereof in the subject relative to a control or reference, and (ii) administering to the subject a therapeutic composition comprising at least one anti-NRP2-antibody or antigen-binding fragment thereof, as described herein.
- the subject has, and/or is selected for treatment based on having, a disease associated with increased levels or expression of NRP2a (e.g., variants 1, 2, and/or 3 of Table Nl) and/or NRP2b (e.g., variants 4 and/or 5 of Table Nl), or an altered ratio of NRP2a:NRP2b expression, relative to a healthy control or matched control standard or population of subject(s).
- NRP2a e.g., variants 1, 2, and/or 3 of Table Nl
- NRP2b e.g., variants 4 and/or 5 of Table Nl
- the subject has significantly higher expression or levels of NRP2b relative to a healthy control or matched control standard or population of subject(s).
- the levels of NRP2b are increased by about or at least about 10%, 20%, 30%, 40%, 50%, 100%, 200%, 300%, 400%, 500%, 600%, 700%, 800%, 900%, 1000% compared to a healthy control or matched control standard or population of subject(s).
- the subject has, and/or is selected for treatment based on having, increased circulating levels of HRS:NRP2 complexes relative to a healthy or matched control standard or population of subject(s).
- Certain embodiments therefore include methods of selecting a subject for cancer treatment, comprising (i) detecting increased expression levels of HRS:NRP2 complexes in the subject relative to a control or reference, and (ii) administering to the subject a therapeutic composition comprising at least one anti-NRP2- antibody or antigen-binding fragment thereof, as described herein.
- the healthy control or matched control standard or population of subject(s) comprises average ranges for age-matched samples of diseased or non-diseased cells or tissue of the same type, which comprise specific characteristics such as drug resistance, metastatic potential, aggressiveness, genetic signature (e.g., p53 mutations, PTEN deletion, IGFR expression), and/or expression patterns.
- specific characteristics such as drug resistance, metastatic potential, aggressiveness, genetic signature (e.g., p53 mutations, PTEN deletion, IGFR expression), and/or expression patterns.
- the agents described herein are generally incorporated into one or more therapeutic or pharmaceutical compositions prior to administration, including veterinary therapeutic compositions.
- compositions that comprise at least one antibody or antigen-binding fragment thereof that specifically binds to a human NRP2 polypeptide, as described herein.
- a therapeutic or pharmaceutical composition comprises one or more of the agents described herein in combination with a pharmaceutically- or physiologically- acceptable carrier or excipient.
- Certain therapeutic compositions further comprise at least one cancer immunotherapy agent, as described herein.
- Some therapeutic compositions comprise (and certain methods utilize) only one anti-NRP2 antibody or antigen-binding fragment thereof. Certain therapeutic compositions comprise (and certain methods utilize) a mixture of at least two, three, four, or five different anti-NRP2 antibodies or antigen-binding fragments thereof.
- compositions comprise at least two anti-NRP2 antibodies, including a first antibody or antigen-binding fragment thereof that specifically binds to at least one first epitope of a human NRP2 polypeptide, and a second antibody or antigen-binding fragment thereof that specifically binds to at least one second epitope of a human NRP2 polypeptide, wherein the at least one first epitope differs from the at least one second epitope.
- the first and the second antibody or antigen-binding fragment thereof specifically and non-competitively bind to the same domain of the NRP2 polypeptide.
- the first anti-NRP2 antibody or antigen-binding fragment thereof binds selectively to a first epitope that is specific to the NRP2a isoform (e.g., variants 1, 2, and/or 3 of Table Nl), and the second anti-NRP2 antibody or antigen-binding fragment thereof binds selectively to a second epitope which is specific to the NRP2b isoform (e.g., variants 4 and/or 5 of Table Nl).
- the first and the second antibody or antigen-binding fragment thereof specifically and non-competitively bind to different domains of the NRP2 polypeptide.
- the first antibody antagonizes the binding/signaling activity between the NRP2 polypeptide and the at least one NRP2 ligand.
- the second antibody or antigen-binding fragment thereof agonizes or enhances the binding/signaling activity between the NRP2 polypeptide and at least one NRP2 ligand.
- the first and the second antibody or antigen-binding fragments thereof are both blocking antibodies, for example, for at least two different NRP2 ligands. In some embodiments, the first and the second antibody or antigen-binding fragments thereof are both partial-blocking antibodies, for example, for at least two different NRP2 ligands. In some instances, the first and the second antibodies or antigen-binding fragments thereof are both non-blocking antibodies, for example, with respect to at least two different NRP2 ligands.
- the first antibody or antigen-binding fragment thereof is a blocking antibody and the second antibody or antigen-binding fragment thereof is a partial-blocking antibody. In certain instances, the first antibody or antigen-binding fragment thereof is a blocking antibody and the second antibody or antigen-binding fragment thereof is a non-blocking antibody.
- the first and the second antibodies or antigen-binding fragments thereof both comprise an IgG Fc domain with high effector function in humans, for example, an IgGl or lgG3 Fc domain. In some embodiments, the first and the second antibodies or antigen-binding fragments thereof comprise an IgG Fc domain with low effector function in humans, for example, an lgG2 or lgG4 Fc domain.
- the first antibody or antigen-binding fragment thereof comprises an IgG Fc domain with high effector function in humans, for example, an IgGl or lgG3 Fc domain
- the second antibody or antigen-binding fragment thereof comprises an IgG Fc domain with low effector function in humans, for example, an lgG2 or lgG4 Fc domain.
- the therapeutic composition comprising the agents such as antibodies or other polypeptide agents (e.g., anti-NRP2 antibodies) is substantially pure on a protein basis or a weight-weight basis, for example, the composition has a purity of at least about 80%, 85%, 90%, 95%, 98%, or 99% on a protein basis or a weight-weight basis.
- the antibodies e.g., anti-NRP2 antibodies
- the antibodies do not form aggregates, have a desired solubility, and/or have an immunogenicity profile that is suitable for use in humans, as described herein and known in the art.
- the therapeutic composition comprising a polypeptide agent for example, an antibody such as an anti-NRP2 antibody
- compositions comprise less than about 10% (on a protein basis) high molecular weight aggregated proteins, or less than about 5% high molecular weight aggregated proteins, or less than about 4% high molecular weight aggregated proteins, or less than about 3% high molecular weight aggregated proteins, or less than about 2 % high molecular weight aggregated proteins, or less than about 1% high molecular weight aggregated proteins.
- Some compositions comprise a polypeptide agent (e.g., an antibody such as an anti-NRP2 antibody) that is at least about 50%, about 60%, about 70%, about 80%, about 90% or about 95% monodisperse with respect to its apparent molecular mass.
- polypeptide agents such as antibodies (e.g., anti-NRP2 antibodies) are concentrated to about or at least about 0.1 mg/ml, 0.2 mg/ml, 0.3 mg/ml, 0.4 mg/ml, 0.5 mg/ml, 0.6, 0.7, 0.8, 0.9, 1 mg/ml, 2 mg/ml, 3 mg/ml, 4 mg/ml, 5 mg/ml, 6 mg/ml, 7 mg/ml, 8 mg/ml, 9 mg/ml, 10 mg/ml, 11, 12, 13, 14 or 15 mg/ml and are formulated for biotherapeutic uses.
- antibodies e.g., anti-NRP2 antibodies
- an effective or desired amount of one or more agents is mixed with any pharmaceutical carrier(s) or excipient known to those skilled in the art to be suitable for the particular agent and/or mode of administration.
- a pharmaceutical carrier may be liquid, semi-liquid or solid.
- Solutions or suspensions used for parenteral, intradermal, intraocular, subcutaneous, direct instillation into the bladder, or topical application may include, for example, a sterile diluent (such as water), saline solution (e.g., phosphate buffered saline; PBS), fixed oil, polyethylene glycol, glycerin, propylene glycol or other synthetic solvent; antimicrobial agents (such as benzyl alcohol and methyl parabens); antioxidants (such as ascorbic acid and sodium bisulfite) and chelating agents (such as ethylenediaminetetraacetic acid (EDTA)); buffers (such as acetates, citrates and phosphates).
- a sterile diluent such as water
- saline solution e.g., phosphate buffered saline; PBS
- fixed oil polyethylene glycol, glycerin, propylene glycol or other synthetic solvent
- antimicrobial agents such
- suitable carriers include physiological saline or phosphate buffered saline (PBS), and solutions containing thickening and solubilizing agents, such as glucose, polyethylene glycol, polypropylene glycol and mixtures thereof.
- PBS physiological saline or phosphate buffered saline
- the therapeutic or pharmaceutical compositions can be prepared by combining an agent-containing composition with an appropriate physiologically acceptable carrier, diluent or excipient, and may be formulated into preparations in solid, semi-solid, liquid or gaseous forms, such as tablets, capsules, powders, granules, ointments, solutions, suppositories, injections, inhalants, gels, microspheres, and aerosols.
- an appropriate physiologically acceptable carrier such as tablets, capsules, powders, granules, ointments, solutions, suppositories, injections, inhalants, gels, microspheres, and aerosols.
- suitable excipients such as salts, buffers and stabilizers may, but need not, be present within the composition.
- Administration may be achieved by a variety of different routes, including oral, parenteral, nasal, intravenous, intraocular, intradermal, intramuscular, subcutaneous, installation into the bladder, or topical.
- Preferred modes of administration depend upon the nature of the condition to be treated or prevented.
- Particular embodiments include administration by IV infusion.
- Carriers can include, for example, pharmaceutically- or physiologically-acceptable carriers, excipients, or stabilizers that are non-toxic to the cell or mammal being exposed thereto at the dosages and concentrations employed.
- physiologically-acceptable carrier is an aqueous pH buffered solution.
- physiologically acceptable carriers include buffers such as phosphate, citrate, and other organic acids; antioxidants including ascorbic acid; low molecular weight (less than about 10 residues) polypeptide; proteins, such as serum albumin, gelatin, or immunoglobulins; hydrophilic polymers such as polyvinylpyrrolidone; amino acids such as glycine, glutamine, asparagine, arginine or lysine; monosaccharides, disaccharides, and other carbohydrates including glucose, mannose, or dextrins; chelating agents such as EDTA; sugar alcohols such as mannitol or sorbitol; salt-forming counterions such as sodium; and/or nonionic surfactants such as polysorbate 20 (TWEENTM) polyethylene glycol (PEG), and poloxamers (PLURONICSTM), and the like.
- buffers such as phosphate, citrate, and other organic acids
- antioxidants including ascorbic acid
- one or more agents can be entrapped in microcapsules prepared, for example, by coacervation techniques or by interfacial polymerization (for example, hydroxymethylcellulose or gelatin-microcapsules and poly-(methylmethacylate)microcapsules, respectively), in colloidal drug delivery systems (for example, liposomes, albumin microspheres, microemulsions, nano-particles and nanocapsules), or in macroemulsions.
- colloidal drug delivery systems for example, liposomes, albumin microspheres, microemulsions, nano-particles and nanocapsules
- the particle(s) or liposomes may further comprise other therapeutic or diagnostic agents.
- the precise dosage and duration of treatment is a function of the disease being treated and may be determined empirically using known testing protocols or by testing the compositions in model systems known in the art and extrapolating therefrom. Controlled clinical trials may also be performed. Dosages may also vary with the severity of the condition to be alleviated.
- a pharmaceutical composition is generally formulated and administered to exert a therapeutically useful effect while minimizing undesirable side effects.
- the composition may be administered one time, or may be divided into a number of smaller doses to be administered at intervals of time. For any particular subject, specific dosage regimens may be adjusted over time according to the individual need.
- Typical routes of administering these and related therapeutic or pharmaceutical compositions thus include, without limitation, oral, topical, transdermal, inhalation, parenteral, sublingual, buccal, ocular, rectal, vaginal, and intranasal.
- parenteral as used herein includes subcutaneous injections, intravenous, instillation into the bladder, intramuscular, intrasternal injection or infusion techniques.
- Therapeutic or pharmaceutical compositions according to certain embodiments of the present disclosure are formulated so as to allow the active ingredients contained therein to be bioavailable upon administration of the composition to a subject or patient.
- compositions that will be administered to a subject or patient may take the form of one or more dosage units, where for example, a tablet may be a single dosage unit, and a container of a herein described agent in aerosol form may hold a plurality of dosage units.
- Actual methods of preparing such dosage forms are known, or will be apparent, to those skilled in this art; for example, see Remington: The Science and Practice of Pharmacy, 20th Edition (Philadelphia College of Pharmacy and Science, 2000).
- the composition to be administered will typically contain a therapeutically effective amount of an agent described herein, for treatment of a disease or condition of interest.
- a therapeutic or pharmaceutical composition may be in the form of a solid or liquid.
- the carrier(s) are particulate, so that the compositions are, for example, in tablet or powder form.
- the carrier(s) may be liquid, with the compositions being, for example, an oral oil, injectable liquid or an aerosol, which is useful in, for example, inhalatory administration.
- the pharmaceutical composition is preferably in either solid or liquid form, where semi-solid, semi-liquid, suspension and gel forms are included within the forms considered herein as either solid or liquid. Certain embodiments include sterile, injectable solutions.
- the pharmaceutical composition may be formulated into a powder, granule, gel, compressed tablet, pill, capsule, chewing gum, wafer or the like.
- a solid composition will typically contain one or more inert diluents or edible carriers.
- binders such as carboxymethylcellulose, ethyl cellulose, microcrystalline cellulose, gum tragacanth or gelatin; excipients such as starch, lactose or dextrins, disintegrating agents such as alginic acid, sodium alginate, Primogel, corn starch and the like; lubricants such as magnesium stearate or Sterotex; glidants such as colloidal silicon dioxide; sweetening agents such as sucrose or saccharin; a flavoring agent such as peppermint, methyl salicylate or orange flavoring; and a coloring agent.
- a liquid carrier such as polyethylene glycol or oil.
- the therapeutic or pharmaceutical composition may be in the form of a liquid, for example, an elixir, syrup, solution, gel, emulsion or suspension.
- the liquid may be for oral administration or for delivery by injection, as two examples.
- preferred composition contain, in addition to the present compounds, one or more of a sweetening agent, preservatives, dye/colorant and flavor enhancer.
- a surfactant, preservative, wetting agent, dispersing agent, suspending agent, buffer, stabilizer and isotonic agent may be included.
- the liquid therapeutic or pharmaceutical compositions may include one or more of the following adjuvants: sterile diluents such as water for injection, saline solution, preferably physiological saline, Ringer's solution, isotonic sodium chloride, fixed oils such as synthetic mono or diglycerides which may serve as the solvent or suspending medium, polyethylene glycols, glycerin, propylene glycol or other solvents; antibacterial agents such as benzyl alcohol or methyl paraben; antioxidants such as ascorbic acid or sodium bisulfite; chelating agents such as ethylenediaminetetraacetic acid; buffers such as acetates, citrates or phosphates and agents for the adjustment of tonicity such as sodium chloride or dextrose.
- the parenteral preparation can be enclosed in ampoules, disposable syringes or multiple dose vials made of glass or plastic.
- Physiological saline is a preferred adjuvant.
- a liquid therapeutic or pharmaceutical composition intended for either parenteral, intraocular, or oral administration should contain an amount of an agent such that a suitable dosage will be obtained. Typically, this amount is at least 0.01% of the agent of interest in the composition. When intended for oral administration, this amount may be varied to be between 0.1 and about 70% of the weight of the composition. Certain oral therapeutic or pharmaceutical compositions contain between about 4% and about 75% of the agent of interest. In certain embodiments, therapeutic or pharmaceutical compositions and preparations are prepared so that a parenteral dosage unit contains between 0.01 to 10% by weight of the agent of interest prior to dilution.
- the therapeutic or pharmaceutical compositions may be intended for topical administration, in which case the carrier may suitably comprise a solution, emulsion, ointment or gel base.
- the base for example, may comprise one or more of the following: petrolatum, lanolin, polyethylene glycols, bee wax, mineral oil, diluents such as water and alcohol, and emulsifiers and stabilizers.
- Thickening agents may be present in a therapeutic or pharmaceutical composition for topical administration.
- the composition may include a transdermal patch or iontophoresis device.
- compositions may be intended for rectal administration, in the form, for example, of a suppository, which will melt in the rectum and release the drug.
- the composition for rectal administration may contain an oleaginous base as a suitable nonirritating excipient.
- bases include, without limitation, lanolin, cocoa butter, and polyethylene glycol.
- the therapeutic or pharmaceutical composition may include various materials, which modify the physical form of a solid or liquid dosage unit.
- the composition may include materials that form a coating shell around the active ingredients.
- the materials that form the coating shell are typically inert, and may be selected from, for example, sugar, shellac, and other enteric coating agents.
- the active ingredients may be encased in a gelatin capsule.
- the therapeutic or pharmaceutical compositions in solid or liquid form may include a component that binds to agent and thereby assists in the delivery of the compound. Suitable components that may act in this capacity include monoclonal or polyclonal antibodies, one or more proteins or a liposome.
- the therapeutic or pharmaceutical composition may consist essentially of dosage units that can be administered as an aerosol.
- aerosol is used to denote a variety of systems ranging from those of colloidal nature to systems consisting of pressurized packages. Delivery may be by a liquefied or compressed gas or by a suitable pump system that dispenses the active ingredients. Aerosols may be delivered in single phase, bi-phasic, or tri-phasic systems in order to deliver the active ingredient(s). Delivery of the aerosol includes the necessary container, activators, valves, subcontainers, and the like, which together may form a kit. One of ordinary skill in the art, without undue experimentation may determine preferred aerosols.
- compositions described herein may be prepared with carriers that protect the agents against rapid elimination from the body, such as time release formulations or coatings.
- carriers include controlled release formulations, such as, but not limited to, implants and microencapsulated delivery systems, and biodegradable, biocompatible polymers, such as ethylene vinyl acetate, polyanhydrides, polyglycolic acid, polyorthoesters, polylactic acid and others known to those of ordinary skill in the art.
- the therapeutic or pharmaceutical compositions may be prepared by methodology well known in the pharmaceutical art.
- a therapeutic or pharmaceutical composition intended to be administered by injection may comprise one or more of salts, buffers and/or stabilizers, with sterile, distilled water so as to form a solution.
- a surfactant may be added to facilitate the formation of a homogeneous solution or suspension.
- Surfactants are compounds that non-covalently interact with the agent so as to facilitate dissolution or homogeneous suspension of the agent in the aqueous delivery system.
- the therapeutic or pharmaceutical compositions may be administered in a therapeutically effective amount, which will vary depending upon a variety of factors including the activity of the specific compound employed; the metabolic stability and length of action of the compound; the age, body weight, general health, sex, and diet of the subject; the mode and time of administration; the rate of excretion; the drug combination; the severity of the particular disorder or condition; and the subject undergoing therapy.
- a therapeutically effective daily dose is (for a 70 kg mammal) from about 0.001 mg/kg (i.e., ⁇ 0.07 mg) to about 100 mg/kg (i.e., ⁇ 7.0 g); preferably a therapeutically effective dose is (for a 70 kg mammal) from about 0.01 mg/kg (i.e., ⁇ 0.7 mg) to about 50 mg/kg (i.e., ⁇ 3.5 g); more preferably a therapeutically effective dose is (for a 70 kg mammal) from about 1 mg/kg (i.e., ⁇ 70 mg) to about 25 mg/kg (i.e., ⁇ 1.75 g).
- the therapeutically effective dose is administered on a weekly, bi-weekly, or monthly basis. In specific embodiments, the therapeutically effective dose is administered on a weekly, bi weekly, or monthly basis, for example, at a dose of about 1-10 or 1-5 mg/kg, or about 1, 2, 3, 4, 5, 6, 7, 8, 9, or 10 mg/kg.
- the combination therapies described herein may include administration of a single pharmaceutical dosage formulation, which contains an anti-NRP2 antibody and an additional therapeutic agent (e.g., immunotherapy agent, chemotherapeutic agent, hormonal therapeutic agent, kinase inhibitor), as well as administration of compositions comprising an anti-NRP2 antibody and an additional therapeutic agent in its own separate pharmaceutical dosage formulation.
- an anti-NRP2 antibody as described herein and additional therapeutic agent can be administered to the subject together in a single oral dosage composition such as a tablet or capsule, or each agent administered in separate oral dosage formulations.
- an anti-NRP2 antibody as described herein and additional therapeutic agent can be administered to the subject together in a single parenteral dosage composition such as in a saline solution or other physiologically acceptable solution, or each agent administered in separate parenteral dosage formulations.
- an anti-NRP2 antibody can be mixed with the cells prior to administration, administered as part of a separate composition, or both. Where separate dosage formulations are used, the compositions can be administered at essentially the same time, i.e., concurrently, or at separately staggered times, i.e., sequentially and in any order; combination therapy is understood to include all these regimens.
- kits comprising (a) at least one antibody or antigen-binding fragment thereof that specifically binds to a human neuropilin 2 (NRP2) polypeptide (an anti-NRP2 antibody), as described herein; and optionally (b) at least one additional therapeutic agent (e.g., immunotherapy agent, chemotherapeutic agent, hormonal therapeutic agent, kinase inhibitor).
- additional therapeutic agent e.g., immunotherapy agent, chemotherapeutic agent, hormonal therapeutic agent, kinase inhibitor.
- kits are in separate therapeutic compositions.
- (a) and (b) are in the same therapeutic composition.
- kits herein may also include a one or more additional therapeutic agents or other components suitable or desired for the indication being treated, or for the desired diagnostic application.
- the kits herein can also include one or more syringes or other components necessary or desired to facilitate an intended mode of delivery (e.g., stents, implantable depots, etc.).
- a patient care kit contains separate containers, dividers, or compartments for the composition(s) and informational material(s).
- the composition(s) can be contained in a bottle, vial, or syringe, and the informational material(s) can be contained in association with the container.
- the separate elements of the kit are contained within a single, undivided container.
- the composition is contained in a bottle, vial or syringe that has attached thereto the informational material in the form of a label.
- the kit includes a plurality (e.g., a pack) of individual containers, each containing one or more unit dosage forms (e.g., a dosage form described herein) of an anti-NRP2 antibody and optionally at least one additional therapeutic agent.
- the kit includes a plurality of syringes, ampules, foil packets, or blister packs, each containing a single unit dose of an anti-NRP2 antibody and optionally at least one additional therapeutic agent.
- the containers of the kits can be air tight, waterproof (e.g., impermeable to changes in moisture or evaporation), and/or light-tight.
- the patient care kit optionally includes a device suitable for administration of the composition, e.g., a syringe, inhalant, dropper (e.g., eye dropper), swab (e.g., a cotton swab or wooden swab), or any such delivery device.
- a device suitable for administration of the composition e.g., a syringe, inhalant, dropper (e.g., eye dropper), swab (e.g., a cotton swab or wooden swab), or any such delivery device.
- the device is an implantable device that dispenses metered doses of the agent(s).
- methods of providing a kit e.g., by combining the components described herein.
- bioassays that relate to anti-NRP2 antibodies and related agents such as therapeutic and diagnostic reagents. Examples include bioassays and analytical assays that measure purity, biological activity, affinity, solubility, pH, endotoxin levels, among others, many of which are described herein. Also included are assays that establish dose response curves and/or provide one or more bases for comparison between different batches of antibody. Batch comparisons can be based on any one or more of chemical characterization, biological characterization, and clinical characterization. Also included are methods of evaluating the potency, stability, pharmacokinetics, and immunogenicity of a selected antibody. Among other uses, these and other methods can be used for lot releasing testing of biologic or chemical agents, including anti-NRP2 antibodies, described herein.
- bioaffinity assays Such assays can be used to assess the binding affinity, for example, between an anti-NRP2 antibody and at least one NRP2 ligand (for example, an NRP2 ligand from Table N2 or Table N3 and/or an HRS polypeptide from Table HI), including its ability to interfere with the interaction between a human NRP2 polypeptide and the at least one NRP2 ligand, or other cellular binding partner.
- NRP2 ligand for example, an NRP2 ligand from Table N2 or Table N3 and/or an HRS polypeptide from Table HI
- Certain exemplary binding affinity assays may utilize ELISA assays, and other immunoassays as described herein and known in the art.
- Certain assays utilize high-performance receptor binding chromatography (see, e.g., Roswall et al., Biologicals.
- binding affinity assays may utilize surface plasmon resonance (SPR)-based technologies. Examples include BIACore technologies, certain of which integrate SPR technology with a microfluidics system to monitor molecular interactions in real time at concentrations ranging from pM to mM. Also included are KINEXATM assays, which provide accurate measurements of binding specificity, binding affinity, and binding kinetics/rate constants. Certain embodiments relate to immunoassays for evaluating or optimizing the immunogenicity of anti-NRP2 antibodies. Examples include ex vivo human cellular assays and in vitro immuno-enzymatic assays to provide useful information on the immunogenic potential of a therapeutic protein.
- Ex vivo cell-response assays can be used, for example, to reproduce the cellular co-operation between antigen-presenting cells (APCs) and T-cells, and thereby measure T-cells activation after contact with a protein of interest.
- Certain in vitro enzymatic assays may utilize a collection of recombinant HLA-DR molecules that cover a significant portion of a relevant human population, and may include automated immuno-enzymatic assays for testing the binding of peptides (stemming from the fragmentation of the therapeutic protein) with the HLA-DR molecules.
- methods of reducing the immunogenicity of a selected protein such as by using these and related methods to identify and then remove or alter one or more T-cell epitopes from an anti-NRP2 antibody.
- biological release assays for measuring parameters such as specific biological activities, including non-canonical biological activities, and cytotoxicity.
- Certain specific biological assays include, for example, cell-based assays that utilize a cellular binding partner (e.g., cell-surface receptor (for example a NRP2 polypeptide and/or at least one NRP2 ligand (for example, an NRP2 ligand from Table N2 or Table N3) presented on the cell surface), which is either endogenously, or recombinantly expressed on the cell surface), which is functionally coupled to a readout, such as a fluorescent or luminescent indicator of NRP2 or NRP2 ligand binding, or functional activity, as described herein.
- a cellular binding partner e.g., cell-surface receptor (for example a NRP2 polypeptide and/or at least one NRP2 ligand (for example, an NRP2 ligand from Table N2 or Table N3) presented on the cell surface
- a readout such as a fluorescent or lumi
- specific embodiments include a cell that either endogenously or recombinantly expresses a human NRP2 polypeptide on the cell surface, which allows assessment of the ability of anti-NRP2 antibody to bind NRP2.
- the anti-NRP2 antibody and/or the NRP2 polypeptide is/are functionally coupled to a readout or indicator, such as a fluorescent or luminescent indicator to measure the binding and/or biological activity of the NRP2 polypeptide.
- the cell also expresses at least one NRP2 ligand (for example, an NRP2 ligand from Table N2 or Table N3 and/or an HRS polypeptide from Table HI), wherein the at least one NRP2 ligand is coupled to a readout or indicator, such as a fluorescent or luminescent indicator of binding and/or biological activity of the at least one NRP2 ligand.
- a readout or indicator such as a fluorescent or luminescent indicator of binding and/or biological activity of the at least one NRP2 ligand.
- cytotoxicity-based biological assays include release assays (e.g., chromium or europium release assays to measure apoptosis; see, e.g., von Zons et al., Clin Diagn Lab lmmunol.4:202-207, 1997), among others, which can assess the cytotoxicity anti-NRP2 antibodies, whether for establishing dose response curves, batch testing, or other properties related to approval by various regulatory agencies, such as the Food and Drug Administration (FDA).
- release assays e.g., chromium or europium release assays to measure apoptosis; see, e.g., von Zons et al., Clin Diagn Lab lmmunol.4:202-207, 1997), among others, which can assess the cytotoxicity anti-NRP2 antibodies, whether for establishing dose response curves, batch testing, or other properties related to approval by various regulatory agencies, such as the Food and Drug Administration (FDA).
- assays for evaluating the effects of an anti-NRP2 antibody on immune cells include an assay system, comprising an activated population of T-cells and at least one anti-NRP2 antibody, wherein the at least one anti-NRP2 antibody interferes with binding of NRP2 to at least one NRP2 ligand (for example, an NRP2 ligand from Table N2 or Table N3 and/or an FIRS polypeptide from Table HI).
- NRP2 ligand for example, an NRP2 ligand from Table N2 or Table N3 and/or an FIRS polypeptide from Table HI.
- Certain embodiments include an assay system, comprising a single monoclonal anti-NRP2 antibody and at least one human NRP2 polypeptide, wherein the anti-NRP2 antibody binds to the NRP2 polypeptide.
- the at least one antibody comprises an lgG4 Fc domain.
- testing material(s) comprising a purified NRP2 polypeptide, wherein said purified NRP2 polypeptide is bound to a solid substrate in a manner that enables antibody binding detection.
- a dose-response curve is an X-Y graph that relates the magnitude of a stressor to the response of a receptor, such as an NRP2-NRP2 ligand (for example, an NRP2 ligand from Table N2 or Table N3 and/or an FIRS polypeptide from Table HI) interaction; the response may be a physiological or biochemical response, such as a non-canonical biological activity in a cell in vitro or in a cell or tissue in vivo, a therapeutically effective amount as measured in vivo (e.g., as measured by EC50), or death, whether measured in vitro or in vivo (e.g., cell death, organismal death).
- a physiological or biochemical response such as a non-canonical biological activity in a cell in vitro or in a cell or tissue in vivo, a therapeutically effective amount as measured in vivo (e.g., as measured by EC50), or death, whether measured in vitro or in vivo (e
- Death is usually indicated as an LD50, a statistically-derived dose that is lethal to 50% of a modeled population, though it can be indicated by LC01 (lethal dose for 1% of the animal test population), LC100 (lethal dose for 100% of the animal test population), or LCL O (lowest dose causing lethality). Almost any desired effect or endpoint can be characterized in this manner.
- the measured dose of a response curve is typically plotted on the X axis and the response is plotted on the Y axis. More typically, the logarithm of the dose is plotted on the X axis, most often generating a sigmoidal curve with the steepest portion in the middle.
- the No Observable Effect Level refers to the lowest experimental dose for which no measurable effect is observed, and the threshold dose refers to the first point along the graph that indicates a response above zero.
- NOEL No Observable Effect Level
- stronger drugs generate steeper dose response curves.
- the desired effects are found at doses slightly greater than the threshold dose, often because lower doses are relatively ineffective and higher doses lead to undesired side effects.
- a curve can be characterized by values such as pg/kg, mg/kg, or g/kg of body- weight, if desired.
- CV coefficient of variation
- two or three or more different batches of anti-NRP2 antibodies or other agents have a CV between them of less than about 30%, 20%, 15%, 14%, 13%, 12%, 11%, 10%, 9%, 8%, 7%, 6%, 5%, 4%, 3%, 2%, or 1% for a 4, 5, 6, 7, or 8 point dose curve.
- the dose response curve is measured in a cell-based assay, and its readout relates to an increase or a decrease in a selected activity of an anti-NRP2 antibody.
- the dose response curve is measured in a cell release assay or animal model (e.g., mouse model), and its readout relates to cell death or animal death.
- a cell release assay or animal model e.g., mouse model
- Certain embodiments include methods and related compositions for expressing and purifying an anti-NRP2 antibody or other polypeptide-based agent described herein.
- Such recombinant anti-NRP2 antibodies can be conveniently prepared using standard protocols as described for example in Sambrook, et al., (1989, supra), in particular Sections 16 and 17; Ausubel et at., (1994, supra), in particular Chapters 10 and 16; and Coligan et al., Current Protocols in Protein Science (John Wiley & Sons, Inc. 1995-1997), in particular Chapters 1, 5 and 6.
- anti-NRP2 antibodies may be prepared by a procedure including one or more of the steps of: (a) preparing a construct comprising a polynucleotide sequences that encode an anti-NRP2 antibody heavy and light chain and that are operably linked to a regulatory element; (b) introducing the constructs into a host cell; (c) culturing the host cell to express an anti-NRP2 antibody; and (d) isolating an anti-NRP2 antibody from the host cell.
- Anti-NRP2 antibody polynucleotides are described elsewhere herein.
- a nucleotide sequence encoding an anti-NRP2 antibody, or a functional equivalent may be inserted into appropriate expression vector, i.e., a vector which contains the necessary elements for the transcription and translation of the inserted coding sequence.
- appropriate expression vector i.e., a vector which contains the necessary elements for the transcription and translation of the inserted coding sequence.
- Methods which are well known to those skilled in the art may be used to construct expression vectors containing sequences encoding a polypeptide of interest and appropriate transcriptional and translational control elements. These methods include in vitro recombinant DNA techniques, synthetic techniques, and in vivo genetic recombination. Such techniques are described in Sambrook et al., Molecular Cloning, A Laboratory Manual (1989), and Ausubel et al., Current Protocols in Molecular Biology (1989).
- a variety of expression vector/host systems are known and may be utilized to contain and express polynucleotide sequences. These include, but are not limited to, microorganisms such as bacteria transformed with recombinant bacteriophage, plasmid, or cosmid DNA expression vectors; yeast transformed with yeast expression vectors; insect cell systems infected with virus expression vectors (e.g ., baculovirus); plant cell systems transformed with virus expression vectors (e.g ., cauliflower mosaic virus, CaMV; tobacco mosaic virus, TMV) or with bacterial expression vectors (e.g., Ti or pBR322 plasmids); or animal cell systems, including mammalian cell and more specifically human cell systems.
- microorganisms such as bacteria transformed with recombinant bacteriophage, plasmid, or cosmid DNA expression vectors
- yeast transformed with yeast expression vectors insect cell systems infected with virus expression vectors (e.g ., baculovirus)
- control elements or "regulatory sequences" present in an expression vector are those non-translated regions of the vector-enhancers, promoters, 5' and 3' untranslated regions-which interact with host cellular proteins to carry out transcription and translation. Such elements may vary in their strength and specificity. Depending on the vector system and host utilized, any number of suitable transcription and translation elements, including constitutive and inducible promoters, may be used. For example, when cloning in bacterial systems, inducible promoters such as the hybrid lacZ promoter of the PBLUESCRIPT phagemid (Stratagene, La Jolla, Calif.) or PSPORT1 plasmid (Gibco BRL, Gaithersburg, Md.) and the like may be used.
- inducible promoters such as the hybrid lacZ promoter of the PBLUESCRIPT phagemid (Stratagene, La Jolla, Calif.) or PSPORT1 plasmid (Gibco BRL, Gaithersburg, Md.)
- promoters from mammalian genes or from mammalian viruses are generally preferred. If it is necessary to generate a cell line that contains multiple copies of the sequence encoding a polypeptide, vectors based on SV40 or EBV may be advantageously used with an appropriate selectable marker.
- a number of expression vectors may be selected depending upon the use intended for the expressed polypeptide. For example, when large quantities are needed, vectors which direct high level expression of fusion proteins that are readily purified may be used.
- vectors include, but are not limited to, the multifunctional E. coli cloning and expression vectors such as BLUESCRIPT (Stratagene), in which the sequence encoding the polypeptide of interest may be ligated into the vector in frame with sequences for the amino-terminal Met and the subsequent 7 residues of b-galactosidase so that a hybrid protein is produced; pIN vectors (Van Heeke & Schuster, J. Biol. Chem.
- pGEX Vectors may also be used to express foreign polypeptides as fusion proteins with glutathione S-transferase (GST).
- GST glutathione S-transferase
- fusion proteins are soluble and can easily be purified from lysed cells by adsorption to glutathione-agarose beads followed by elution in the presence of free glutathione.
- Proteins made in such systems may be designed to include heparin, thrombin, or factor XA protease cleavage sites so that the cloned polypeptide of interest can be released from the GST moiety at will.
- Certain embodiments may employ E.
- coli-based expression systems see, e.g., Structural Genomics Consortium et al., Nature Methods. 5:135-146, 2008). These and related embodiments may rely partially or totally on ligation-independent cloning (LIC) to produce a suitable expression vector.
- protein expression may be controlled by a T7 RNA polymerase (e.g., pET vector series).
- T7 RNA polymerase e.g., pET vector series
- These and related embodiments may utilize the expression host strain BL21(DE3), a l ⁇ E3 lysogen of BL21 that supports T7-mediated expression and is deficient in Ion and ompT proteases for improved target protein stability.
- expression host strains carrying plasmids encoding tRNAs rarely used in E. coli such as ROSETTA TM (DE3) and Rosetta 2 (DE3) strains.
- Cell lysis and sample handling may also be improved using reagents sold under the trademarks BENZONASE ® nuclease and BUGBUSTER ® Protein Extraction Reagent.
- BENZONASE ® nuclease and BUGBUSTER ® Protein Extraction Reagent.
- auto-inducing media can improve the efficiency of many expression systems, including high-throughput expression systems.
- Media of this type e.g., OVERNIGHT EXPRESSTM Autoinduction System gradually elicit protein expression through metabolic shift without the addition of artificial inducing agents such as IPTG.
- Particular embodiments employ hexahistidine tags (such as those sold under the trademark HIS»TAG ® fusions), followed by immobilized metal affinity chromatography (IMAC) purification, or related techniques.
- clinical grade proteins can be isolated from E. coli inclusion bodies, without or without the use of affinity tags (see, e.g., Shimp et al., Protein Expr Purif. 50:58-67, 2006).
- affinity tags see, e.g., Shimp et al., Protein Expr Purif. 50:58-67, 2006.
- certain embodiments may employ a cold-shock induced E. coli high-yield production system, because over-expression of proteins in Escherichia coli at low temperature improves their solubility and stability (see, e.g., Qing et al., Nature Biotechnology. 22:877-882, 2004).
- high-density bacterial fermentation systems For example, high cell density cultivation of Ralstonia eutropha allows protein production at cell densities of over 150 g/L, and the expression of recombinant proteins at titers exceeding 10 g/L.
- yeast Saccharomyces cerevisiae a number of vectors containing constitutive or inducible promoters such as alpha factor, alcohol oxidase, and PGH may be used.
- constitutive or inducible promoters such as alpha factor, alcohol oxidase, and PGH
- PGH palladium phosphate
- Pichia pandoris expression systems see, e.g., Li et al., Nature Biotechnology. 24, 210 - 215, 2006; and Hamilton et al., Science, 301:1244, 2003).
- Certain embodiments include yeast systems that are engineered to selectively glycosylate proteins, including yeast that have humanized N-glycosylation pathways, among others (see, e.g., Hamilton et al., Science. 313:1441-1443, 2006; Wildt et al.,
- recombinant yeast cultures can be grown in Fernbach Flasks or 15L, 50L, 100L, and 200L fermentors, among others.
- sequences encoding polypeptides may be driven by any of a number of promoters.
- viral promoters such as the 35S and 19S promoters of CaMV may be used alone or in combination with the omega leader sequence from TMV (Takamatsu, EMBO J. 3:1671- 1680 (1984); Broglie et al., Science 224:838-843 (1984); and Winter et al., Results Probl. Cell Differ. 17:85-105 (1991)).
- constructs can be introduced into plant cells by direct DNA transformation or pathogen-mediated transfection.
- direct DNA transformation or pathogen-mediated transfection Such techniques are described in a number of generally available reviews (see, e.g., Flobbs in McGraw Hill, Yearbook of Science and Technology, pp. 191-196 (1992)).
- An insect system may also be used to express a polypeptide of interest.
- Autographa californica nuclear polyhedrosis virus (AcNPV) is used as a vector to express foreign genes in Spodoptera frugiperda cells or in Trichoplusia cells.
- the sequences encoding the polypeptide may be cloned into a non-essential region of the virus, such as the polyhedrin gene, and placed under control of the polyhedrin promoter. Successful insertion of the polypeptide encoding sequence will render the polyhedrin gene inactive and produce recombinant virus lacking coat protein.
- the recombinant viruses may then be used to infect, for example, S.
- frugiperda cells or Trichoplusia cells in which the polypeptide of interest may be expressed (Engelhard et al., Proc. Natl. Acad. Sci. U.S.A. 91:3224-3227 (1994)). Also included are baculovirus expression systems, including those that utilize SF9, SF21, and T. ni cells (see, e.g., Murphy and Piwnica-Worms, Curr Protoc Protein Sci. Chapter 5:Unit5.4, 2001). Insect systems can provide post-translation modifications that are similar to mammalian systems.
- a number of viral-based expression systems are generally available.
- sequences encoding a polypeptide of interest may be ligated into an adenovirus transcription/translation complex consisting of the late promoter and tripartite leader sequence. Insertion in a non-essential El or E3 region of the viral genome may be used to obtain a viable virus which is capable of expressing the polypeptide in infected host cells (Logan & Shenk, Proc. Natl. Acad. Sci. U.S.A. 81:3655-3659 (1984)).
- transcription enhancers such as the Rous sarcoma virus (RSV) enhancer, may be used to increase expression in mammalian host cells.
- RSV Rous sarcoma virus
- Examples of useful mammalian host cell lines include monkey kidney CV1 line transformed by SV40 (COS-7, ATCC CRL 1651); human embryonic kidney line (293 or 293 cells sub-cloned for growth in suspension culture, Graham et al J. Gen Virol. 36:59 (1977)); baby hamster kidney cells (BHK, ATCC CCL 10); mouse sertoli cells (TM4, Mather, Biol. Reprod.
- COS-7 monkey kidney CV1 line transformed by SV40
- human embryonic kidney line (293 or 293 cells sub-cloned for growth in suspension culture, Graham et al J. Gen Virol. 36:59 (1977)
- baby hamster kidney cells BHK, ATCC CCL 10
- mouse sertoli cells TM4, Mather, Biol. Reprod.
- monkey kidney cells (CV1 ATCC CCL 70); African green monkey kidney cells (VERO-76, ATCC CRL-1587); human cervical carcinoma cells (HELA, ATCC CCL 2); canine kidney cells (MDCK, ATCC CCL 34); buffalo rat liver cells (BRL 3A, ATCC CRL 1442); human lung cells (W138, ATCC CCL 75); human liver cells (Hep G2, HB 8065); mouse mammary tumor (MMT 060562, ATCC CCL51); TR1 cells (Mather et al., Annals N.Y. Acad. Sci. 383:44-68 (1982)); MRC 5 cells; FS4 cells; and a human hepatoma line (Hep G2).
- CHO Chinese hamster ovary
- DHFR-CHO cells Urlaub et al., PNAS USA 77:4216 (1980)
- myeloma cell lines such as NSO and Sp2/0.
- CHO Chinese hamster ovary
- myeloma cell lines such as NSO and Sp2/0.
- Certain preferred mammalian cell expression systems include CHO and HEK293-cell based expression systems.
- Mammalian expression systems can utilize attached cell lines, for example, in T- flasks, roller bottles, or cell factories, or suspension cultures, for example, in 1L and 5L spinners, 5L, 14L, 40L, 100L and 200L stir tank bioreactors, or 20/50L and 100/200L WAVE bioreactors, among others known in the art.
- RNA polymerase typically utilize purified RNA polymerase, ribosomes, tRNA and ribonucleotides; these reagents may be produced by extraction from cells or from a cell-based expression system.
- Specific initiation signals may also be used to achieve more efficient translation of sequences encoding a polypeptide of interest. Such signals include the ATG initiation codon and adjacent sequences. In cases where sequences encoding the polypeptide, its initiation codon, and upstream sequences are inserted into the appropriate expression vector, no additional transcriptional or translational control signals may be needed. However, in cases where only coding sequence, or a portion thereof, is inserted, exogenous translational control signals including the ATG initiation codon should be provided. Furthermore, the initiation codon should be in the correct reading frame to ensure translation of the entire insert. Exogenous translational elements and initiation codons may be of various origins, both natural and synthetic. The efficiency of expression may be enhanced by the inclusion of enhancers which are appropriate for the particular cell system which is used, such as those described in the literature (Scharf. et al., Results Probl. Cell Differ. 20:125-162 (1994)).
- a host cell strain may be chosen for its ability to modulate the expression of the inserted sequences or to process the expressed protein in the desired fashion.
- modifications of the polypeptide include, but are not limited to, post-translational modifications such as acetylation, carboxylation, glycosylation, phosphorylation, lipidation, and acylation.
- Post-translational processing which cleaves a "prepro" form of the protein may also be used to facilitate correct insertion, folding and/or function.
- Different host cells such as yeast, CHO, HeLa, MDCK, HEK293, and W138, in addition to bacterial cells, which have or even lack specific cellular machinery and characteristic mechanisms for such post-translational activities, may be chosen to ensure the correct modification and processing of the foreign protein.
- cell lines which stably express a polynucleotide of interest may be transformed using expression vectors which may contain viral origins of replication and/or endogenous expression elements and a selectable marker gene on the same or on a separate vector. Following the introduction of the vector, cells may be allowed to grow for about 1-2 days in an enriched media before they are switched to selective media. The purpose of the selectable marker is to confer resistance to selection, and its presence allows growth and recovery of cells which successfully express the introduced sequences. Resistant clones of stably transformed cells may be proliferated using tissue culture techniques appropriate to the cell type. Transient production, such as by transient transfection or infection, can also be employed. Exemplary mammalian expression systems that are suitable for transient production include FIEK293 and CFIO-based systems.
- selection systems may be used to recover transformed or transduced cell lines. These include, but are not limited to, the herpes simplex virus thymidine kinase (Wigler et al., Cell 11:223-232 (1977)) and adenine phosphoribosyltransferase (Lowy et al., Cell 22:817-823 (1990)) genes which can be employed in tk- or aprt- cells, respectively. Also, antimetabolite, antibiotic or herbicide resistance can be used as the basis for selection; for example, dhfr which confers resistance to methotrexate (Wigler et al., PNAS USA.
- npt which confers resistance to the aminoglycosides, neomycin and G-418 (Colbere-Garapin et al., J. Mol. Biol. 150:1- 14 (1981)); and als or pat, which confer resistance to chlorsulfuron and phosphinotricin acetyltransferase, respectively (Murry, supra). Additional selectable genes have been described, for example, trpB, which allows cells to utilize indole in place of tryptophan, or hisD, which allows cells to utilize histinol in place of histidine (Flartman & Mulligan, Proc. Natl. Acad. Sci. U.S.A.
- GFP green fluorescent protein
- RFP red fluorescent protein
- YFP fluorescent protein
- anthocyanins e.g., RFP, YFP
- anthocyanins e.g., b-glucuronidase and its substrate GUS
- luciferase and its substrate luciferin e.g., luciferase and its substrate luciferin
- high-throughput protein production systems or micro-production systems. Certain aspects may utilize, for example, hexa-histidine fusion tags for protein expression and purification on metal chelate-modified slide surfaces or MagneHis Ni-Particles (see, e.g., Kwon et al BMC Biotechnol. 9:72, 2009; and Lin et al., Methods Mol Biol. 498:129-41, 2009)). Also included are high-throughput cell-free protein expression systems (see, e.g., Sitaraman et al., Methods Mol Biol. 498:229-44, 2009). These and related embodiments can be used, for example, to generate microarrays of anti-NRP2 antibodies which can then be used for screening libraries to identify antibodies and antigen-binding domains that interact with the NRP2 polypeptide(s) of interest.
- Means for producing labeled hybridization or PCR probes for detecting sequences related to polynucleotides include oligolabeling, nick translation, end-labeling or PCR amplification using a labeled nucleotide.
- the sequences, or any portions thereof may be cloned into a vector for the production of an mRNA probe.
- Such vectors are known in the art, are commercially available, and may be used to synthesize RNA probes in vitro by addition of an appropriate RNA polymerase such as T7, T3, or SP6 and labeled nucleotides.
- reporter molecules or labels include radionuclides, enzymes, fluorescent, chemiluminescent, or chromogenic agents as well as substrates, cofactors, inhibitors, magnetic particles, and the like.
- Host cells transformed with a polynucleotide sequence of interest may be cultured under conditions suitable for the expression and recovery of the protein from cell culture.
- Certain specific embodiments utilize serum free cell expression systems. Examples include HEK293 cells and CHO cells that can grown on serum free medium (see, e.g., Rosser et al., Protein Expr. Purif. 40:237-43, 2005; and U.S. Patent number 6,210,922).
- An antibody, or antigen-binding fragment thereof, produced by a recombinant cell may be secreted or contained intracellularly depending on the sequence and/or the vector used.
- expression vectors containing polynucleotides may be designed to contain signal sequences which direct secretion of the encoded polypeptide through a prokaryotic or eukaryotic cell membrane.
- Other recombinant constructions may be used to join sequences encoding a polypeptide of interest to nucleotide sequence encoding a polypeptide domain which will facilitate purification and/or detection of soluble proteins.
- cleavable and non-cleavable affinity purification and epitope tags such as avidin, FLAG tags, poly-histidine tags (e.g., 6xHis), cMyc tags, V5-tags, glutathione S-transferase (GST) tags, and others.
- the protein produced by a recombinant cell can be purified and characterized according to a variety of techniques known in the art.
- Exemplary systems for performing protein purification and analyzing protein purity include fast protein liquid chromatography (FPLC) (e.g., AKTA and Bio-Rad FPLC systems), high-pressure liquid chromatography (HPLC) (e.g., Beckman and Waters H PLC).
- FPLC fast protein liquid chromatography
- HPLC high-pressure liquid chromatography
- Exemplary chemistries for purification include ion exchange chromatography (e.g., Q, S), size exclusion chromatography, salt gradients, affinity purification (e.g., Ni, Co, FLAG, maltose, glutathione, protein A/G), gel filtration, reverse-phase, ceramic HYPERD ® ion exchange chromatography, and hydrophobic interaction columns (HIC), among others known in the art. Also included are analytical methods such as SDS-PAGE (e.g., coomassie, silver stain), immunoblot, Bradford, and ELISA, which may be utilized during any step of the production or purification process, typically to measure the purity of the protein composition.
- affinity purification e.g., Ni, Co, FLAG, maltose, glutathione, protein A/G
- gel filtration e.g., reverse-phase, ceramic HYPERD ® ion exchange chromatography
- HIC hydrophobic interaction columns
- analytical methods such as SDS-PAGE (
- concentrated solutions of anti-NRP2 antibodies may comprise proteins at a concentration of about 5 mg/mL; or about 8 mg/mL; or about 10 mg/mL; about 15 mg/mL; or about 20 mg/mL.
- compositions may be substantially monodisperse, meaning that an at least one anti-NRP2 antibody exists primarily (i.e., at least about 90%, or greater) in one apparent molecular weight form when assessed for example, by size exclusion chromatography, dynamic light scattering, or analytical ultracentrifugation.
- compositions have a purity (on a protein basis) of at least about 90%, or in some aspects at least about 95% purity, or in some embodiments, at least 98% purity. Purity may be determined via any routine analytical method as known in the art.
- compositions have a high molecular weight aggregate content of less than about 10%, compared to the total amount of protein present, or in some embodiments such compositions have a high molecular weight aggregate content of less than about 5%, or in some aspects such compositions have a high molecular weight aggregate content of less than about 3%, or in some embodiments a high molecular weight aggregate content of less than about 1%.
- High molecular weight aggregate content may be determined via a variety of analytical techniques including for example, by size exclusion chromatography, dynamic light scattering, or analytical ultracentrifugation.
- concentration approaches contemplated herein include lyophilization, which is typically employed when the solution contains few soluble components other than the protein of interest. Lyophilization is often performed after HPLC run, and can remove most or all volatile components from the mixture. Also included are ultrafiltration techniques, which typically employ one or more selective permeable membranes to concentrate a protein solution. The membrane allows water and small molecules to pass through and retains the protein; the solution can be forced against the membrane by mechanical pump, gas pressure, or centrifugation, among other techniques.
- the reagents, anti-NRP2 antibodies, or related agents have a purity of at least about 90%, as measured according to routine techniques in the art.
- an anti-NRP2 antibody composition has a purity of at least about 95%.
- an anti-NRP2 antibody composition has a purity of at least about 97% or 98% or 99%.
- anti-NRP2 antibodies can be of lesser purity, and may have a purity of at least about 50%, 60%, 70%, or 80%. Purity can be measured overall or in relation to selected components, such as other proteins, e.g., purity on a protein basis.
- Purified anti-NRP2 antibodies can also be characterized according to their biological characteristics. Binding affinity and binding kinetics can be measured according to a variety of techniques known in the art, such as Biacore ® and related technologies that utilize surface plasmon resonance (SPR), an optical phenomenon that enables detection of unlabeled interactants in real time. SPR-based biosensors can be used in determination of active concentration, screening and characterization in terms of both affinity and kinetics.
- SPR surface plasmon resonance
- the presence or levels of one or more canonical or non-canonical biological activities can be measured according to cell-based assays, including those that utilize a cellular binding partner of a selected anti-NRP2 antibody, which is functionally coupled to a readout or indicator, such as a fluorescent or luminescent indicator of biological activity, as described herein.
- a readout or indicator such as a fluorescent or luminescent indicator of biological activity
- an anti-NRP2 antibody composition is substantially endotoxin free, including, for example, about 95% endotoxin free, preferably about 99% endotoxin free, and more preferably about 99.99% endotoxin free.
- endotoxins can be detected according to routine techniques in the art, as described herein.
- an anti-NRP2 antibody composition is made from a eukaryotic cell such as a mammalian or human cell in substantially serum free media.
- an anti-NRP2 antibody composition has an endotoxin content of less than about 10 EU/mg of anti-NRP2 antibody, or less than about 5 EU/mg of anti-NRP2 antibody, less than about 3 EU/mg of anti-NRP2 antibody, or less than about 1 EU/mg of anti-NRP2 antibody.
- an anti-NRP2 antibody composition comprises less than about 10% wt/wt high molecular weight aggregates, or less than about 5% wt/wt high molecular weight aggregates, or less than about 2% wt/wt high molecular weight aggregates, or less than about or less than about 1% wt/wt high molecular weight aggregates.
- Protein-based analytical assays and methods which can be used to assess, for example, protein purity, size, solubility, and degree of aggregation, among other characteristics.
- Protein purity can be assessed a number of ways. For instance, purity can be assessed based on primary structure, higher order structure, size, charge, hydrophobicity, and glycosylation.
- methods for assessing primary structure include N- and C-terminal sequencing and peptide mapping (see, e.g., Allen et al., Biologicals. 24:255-275, 1996)).
- methods for assessing higher order structure include circular dichroism (see, e.g., Kelly et al., Biochim Biophys Acta.
- Flydrophobicity can be assessed, for example, by reverse-phase HPLC and hydrophobic interaction chromatography HPLC. Glycosylation can affect pharmacokinetics (e.g., clearance), conformation or stability, receptor binding, and protein function, and can be assessed, for example, by mass spectrometry and nuclear magnetic resonance (NMR) spectroscopy.
- pharmacokinetics e.g., clearance
- conformation or stability e.g., conformation or stability
- receptor binding e.g., and protein function
- NMR nuclear magnetic resonance
- certain embodiments include the use of SEC-HPLC to assess protein characteristics such as purity, size (e.g., size homogeneity) or degree of aggregation, and/or to purify proteins, among other uses.
- SEC also including gel-filtration chromatography (GFC) and gel- permeation chromatography (GPC), refers to a chromatographic method in which molecules in solution are separated in a porous material based on their size, or more specifically their hydrodynamic volume, diffusion coefficient, and/or surface properties. The process is generally used to separate biological molecules, and to determine molecular weights and molecular weight distributions of polymers.
- a biological or protein sample (such as a protein extract produced according to the protein expression methods provided herein and known in the art) is loaded into a selected size-exclusion column with a defined stationary phase (the porous material), preferably a phase that does not interact with the proteins in the sample.
- the stationary phase is composed of inert particles packed into a dense three-dimensional matrix within a glass or steel column.
- the mobile phase can be pure water, an aqueous buffer, an organic solvent, or a mixture thereof.
- the stationary-phase particles typically have small pores and/or channels which only allow molecules below a certain size to enter.
- Protein purity for clinical applications is also discussed, for example, by Anicetti et al. (Trends in Biotechnology. 7:342-349, 1989). More recent techniques for analyzing protein purity include, without limitation, the LabChip GXII, an automated platform for rapid analysis of proteins and nucleic acids, which provides high throughput analysis of titer, sizing, and purity analysis of proteins.
- clinical grade proteins such as protein fragments and antibodies can be obtained by utilizing a combination of chromatographic materials in at least two orthogonal steps, among other methods (see, e.g., Therapeutic Proteins: Methods and Protocols.
- protein agents e.g., anti-NRP2 antibodies, and antigen-binding fragments
- protein agents are substantially endotoxin-free, as measured according to techniques known in the art and described herein.
- Protein solubility assays are also included. Such assays can be utilized, for example, to determine optimal growth and purification conditions for recombinant production, to optimize the choice of buffer(s), and to optimize the choice of anti-NRP2 antibodies or variants thereof. Solubility or aggregation can be evaluated according to a variety of parameters, including temperature, pH, salts, and the presence or absence of other additives. Examples of solubility screening assays include, without limitation, microplate-based methods of measuring protein solubility using turbidity or other measure as an end point, high-throughput assays for analysis of the solubility of purified recombinant proteins (see, e.g., Stenvall et al., Biochim Biophys Acta.
- Anti-NRP2 antibodies with increased solubility can be identified or selected for according to routine techniques in the art, including simple in vivo assays for protein solubility (see, e.g., Maxwell et al., Protein Sci. 8:1908-11, 1999).
- Protein solubility and aggregation can also be measured by dynamic light scattering techniques.
- Aggregation is a general term that encompasses several types of interactions or characteristics, including soluble/insoluble, covalent/noncovalent, reversible/irreversible, and native/denatured interactions and characteristics.
- the presence of aggregates is typically considered undesirable because of the concern that aggregates may cause an immunogenic reaction (e.g., small aggregates), or may cause adverse events on administration (e.g., particulates).
- Dynamic light scattering refers to a technique that can be used to determine the size distribution profile of small particles in suspension or polymers such as proteins in solution.
- This technique also referred to as photon correlation spectroscopy (PCS) or quasi-elastic light scattering (QELS), uses scattered light to measure the rate of diffusion of the protein particles. Fluctuations of the scattering intensity can be observed due to the Brownian motion of the molecules and particles in solution.
- This motion data can be conventionally processed to derive a size distribution for the sample, wherein the size is given by the Stokes radius or hydrodynamic radius of the protein particle. The hydrodynamic size depends on both mass and shape (conformation). Dynamic scattering can detect the presence of very small amounts of aggregated protein ( ⁇ 0.01% by weight), even in samples that contain a large range of masses.
- certain embodiments include the use of dynamic light scattering to analyze the solubility and/or presence of aggregates in a sample that contains an anti- NRP2 antibody of the present disclosure.
- humanized anti-NRP2 antibodies were generated from a panel of murine monoclonal antibodies targeting different domains of human NRP2. Humanized antibodies were affinity matured to produce highly selective, potent antibodies with sub nanomolar affinities in the context of primarily human IgG constant domain to limit the potential for immunogenicity in humans. Initial assessments of binding affinity as measured by surface plasmon resonance (SPR), and flow cytometry (FACS) binding to cell lines expressing recombinant NRP2, is presented in Table El.
- SPR surface plasmon resonance
- FACS flow cytometry
- Humanized murine monoclonal antibodies were prepared via grafting of murine CDRs onto human lgG4 with the selective replacement of murine specific amino acid substitutions compared to the corresponding human sequences when necessary to stabilize the antibody, and screening to confirm binding to NRP2 polypeptides.
- Humanized antibodies were affinity matured via the systematic mutation of their CDR sequences, and the most advantageous recombination of the higher affinity combinations identified were fully characterized.
- Recombinant antibodies were purified from conditioned medium starting at 2 weeks of culture by flowing over a Protein A affinity column, eluting and storing in Phosphate Buffered Saline (IX PBS), pH 7.4. Each lot was tested for protein concentration, purity, and endotoxin level. Purity by SDS- PAGE was routinely >90%.
- SPR Surface plasmon resonance
- the sensor chip surface was regenerated between each analyte run to remove anti- NRP2 antibodies and NRP2 protein. Data was double referenced against a surface with no anti-NRP2 antibody captured (immobilized anti-human antibody only) and a buffer only blank. Affinity constants were derived by globally fitting sensograms to a Langmuir (1:1) interaction model in the ProteOn manager software. For each anti-NRP2 antibody, data from the multiple NRP2 concentrations was fit as a single data set with dissociation rate constant (/3 ⁇ 4), association rate constant (k a ) and R max values as global parameters. The reported binding affinity is the equilibrium dissociation constant (K D ) calculated from k k a .
- Running buffer 50 mM HEPES, 300 mM NaCI, 5 mM CaCI 2 , 0.005% Tween-20, pH 7.4
- Antigen Human NRP2 (aa23-855) with C-terminal Avi-, Myc- and His-tags
- Regeneration buffer 10 mM glycine pH 2.0
- Plasmid containing human NRP2 were purchased from Origene. To generate a large stock of plasmids and purify the DNA, plasmid was transformed into chemically competent E. coli cells (One Shot TOP10) according to the manufacturer's instructions. The transformed bacteria were grown in the recommended liquid medium (Difco Dehydrated Miler Luria-Bertani medium powder resuspended in water) containing kanamycin monosulfate (50 pg/mL) as an antibiotic. The plasmid DNA was then purified using the QIAGEN DNA maxi prep kit according to the kit's instructions. DNA concentration and purity were measured on a spectrophotometer (Nanodrop 2000). An A260/A280 absorbance ratio between 1.8 and 2.0 was required for transfection.
- the linearized plasmid described above was transfected into Expi293 cells using an SF Cell Line 4D-Nucleofector ® X Kit L (Lonza Cat#V4XC-2012) and standard protocol T-030 for suspension FIEK293 cells. Cells were allowed to recover in static culture for 17 hours, transferred to suspension and recovered an additional 72 hours, and then were selected with 200-350 pg/mL G418 in 50 pg increments (ThermoFisher Cat#10131035). Cell densities and viabilities were monitored for a period of 3 weeks, with fresh media/antibiotic replacement every 2-3 days.
- Expi293-hNRP2 clonal cells were collected by centrifugation at 300g for 5 minutes, and washed twice by DPBS (with calcium and magnesium, ThermoFisher Cat#14040133). Washed cells were added to a 96-well V-bottom plate (ThermoFisher Cat#1424572) at 100,000 cells/well in 50 pL of DPBS added with Zombie Violet viability stain (Biolegend Cat#423114, diluted at 1:500). From this step on, cells were protected from light.
- Binding was allowed to proceed on ice for 40-60 minutes. Cells were then pelleted at 300g for 5 minutes at 4°C, supernatants removed, and cells washed twice by adding 150 pL of FWB and centrifuging the cells again in the same conditions.
- Cy3-conjugated goat anti-human IgG Fc was added to the cells at a final concentration of 3 pg/mL in 30 pL of FWB. After 30-40 minutes of incubation on ice, cells were pelleted at 300g for 5 minutes at 4°C and supernatants removed, and the cells were washed twice as described previously.
- Expi293 propagation and transient transfection Expi293 cells, a HEK293 transient expression system maintained in suspension cultures, were used to express cynomolgus monkey NRP2. Cells were grown in 60 mL Expi293 medium within 250 mL vented suspension culture flasks. The propagation of cells was carried out in a Multitron Cell incubator at 37°C, with 8% CC , 80% humidity, and shaking at 225 rpm. During the maintenance and expansion phase, Expi293 cells were split twice a week at 0.3 x 10 s cells/mL in order to keep the density within the optimal range for transfection and the viability high. Cell densities and viabilities were determined using a cell counter (Cedex HiRes Cell Analyzer).
- the Expi293 cells were seeded at a density of 2.0 x 10 s cells/mL in order to maintain high viability (>95%) and low density (not to exceed 3-5 x 10 s cells/mL), thereby providing cells with fresh nutrients and avoiding transfection impediments caused by any secreted substances.
- Expi293 cells Prior to DNA transfection, Expi293 cells were counted and reseeded at 2.5 x 10 s cells/mL in 50 mL shake flasks (TPP TubeSpin bioreactor tubes). The transfection procedure was performed using the Expifectamine kit. The manufacturer's protocol was adapted for a transfection in a total volume of 5 mL instead of 30 mL (i.e., all volumes were divided by a factor of 6). Five pg of each plasmid DNA was diluted in Opti-MEM reduced serum medium, complexed with Expifectamine transfection reagent, and transfected into Expi293 cells.
- transfected pools were cultured with shaking at 225 rpm to ensure complete suspension of the cells within the 50 mL bioreactors. Following the manufacturer's protocol, Expifectamine kit enhancers were added after 16-18 hours, and the cultures analyzed by flow cytometry 2 days post-transfection.
- Cynomolgus monkey (cyno) NRP2-transfected Expi293 cells were collected by centrifugation at 300g for 5 minutes, and washed twice by DPBS (with calcium and magnesium, ThermoFisher Cat#14040133). Washed cells were added to a 96-well V-bottom plate (ThermoFisher Cat#1424572) at 100,000 cells/well in 50 pL of DPBS added with Zombie Violet viability stain (Biolegend Cat#423114, diluted at 1:500). From this step on, cells were protected from light.
- NRP2 over expression on the cell surface was validated by a-NRP2 staining (10 pg/mL R&D #AF567 a-NRP2) in separate wells. Binding was allowed to proceed on ice for 40-60 minutes. Cells were then pelleted at 300g for 5 minutes at 4°C, supernatants removed, and cells washed twice by adding 150 pL of FWB and centrifuging the cells again in the same conditions.
- Cy3-conjugated goat anti-human IgG Fc or AF647-conjugated donkey anti-goat IgG was added to the cells at a final concentration of 3 pg/mL in 30 pL of FWB. After 30-40 minutes of incubation on ice, cells were pelleted at 300g for 5 minutes at 4°C and supernatants removed, and the cells were washed twice as described previously. Cells were then resuspended in FWB before acquisition on the Cytoflex. Gains were set based on staining controls. Cells were collected with typically more than 10,000 events. Cells were then analyzed on FlowJo analysis software by excluding dead cells and gating singlets.
- SPR Surface plasmon resonance
- Cynomolgus NRP2 antigen protein was flowed over the captured antibody at varying concentrations (150, 50, 16.67, 5.56, 1.85 nM).
- the sensor chip surface was regenerated between each analyte run to remove anti-NRP2 antibodies and NRP2 protein.
- Data was double referenced against a surface with no anti- NRP2 antibody captured (immobilized anti-human antibody only) and a buffer only blank.
- Affinity constants were derived by globally fitting sensograms to a bivalent analyte interaction model in the ProteOn manager software.
- Running buffer 50 mM HEPES, 300 mM NaCI, 5 mM CaCI 2 , 0.005% Tween-20, pH 7.4
- Regeneration buffer 10 mM glycine pH 2.0
- NRP2a version 2
- NRP2b version 5
- FLT4 VEGFR3
- KDR VEGFR2
- PLXNA1 plexin A1
- Nano- Glo assay substrate (Promega) was added, and the plate was read on a Glomax 96 luminometer at room temperature to establish baseline luminescence. Antibodies were added to the well at lOOnM and the plate was again read to establish a new baseline and monitor the effects of the antibodies on spontaneous receptor dimerization. Depending on the receptor pair, typically 200nM SEMA3F- p95 (aTyr Pharma), 2nM VEGF-C (R&D Systems, Minnesota), or 2nM VEGF I65 (R&D Systems, Minnesota) were then added and the plate was again read to measure dimerization of receptors.
- antibody aNRP2-14v9 which binds to the a2 domain of NRP2, was demonstrated to exhibit extremely potent inhibition of NRP2-plexin heterodimerization, while having no significant impact on NRP2-VEGFR3 heterodimerization.
- these characteristics suggest that this antibody would potently inhibit semaphorin 3 signaling through NRP2, without significantly inhibiting the signaling through VEGFR2 or 3.
- Such characteristics therefore make this antibody well suited for applications where the selective modulation of semaphorin signaling is required. For example, for modulating effects of semaphorin signaling on axonal growth avoidance, lymphatic sprouting, cell migration, smooth muscle contractility, immune cell activation and exhaustion, as more generally modulating cell growth and proliferation.
- antibody aNRP2-10vl0 which binds to the bl domain of NRP2, shows the ability to potently inhibit NRP2-VEGFR3 heterodimerization, without significantly inhibiting NRP2- plexin heterodimerization.
- antibody clone aNRP2-llv7 which binds to the b2 domain of NRP2, shows the ability to inhibit the heterodimerization of NRP2 to FLT4, but increased the ligand induced dimerization signal for both Plexin and KDR. Suggesting that it stabilizers heterodimeric and higher order complexes of NRP2.
- Human NRP2a version 2; see Table Nl
- mouse NRP2v2 cDNAs were obtained from Origene. Because we have previously demonstrated that the aNRP2-10vl0 antibody binds specifically to the bl domain of human NRP2, but not mouse NRP2, mutations in the bl domain of mouse NRP2 sequence (F299Y, K354N, 1383V, M400A, 1407V, and L416S) were made in isolation to restore the amino acids which differ between the human and mouse proteins in this region. Human and mouse NRP2, expression vectors, along with expression vectors encoding all 6 mutants were transfected into Expi293 cells at 1 million cells/mL, by standard techniques.
- aNRP2-10vl0 Approximately 40 hours post transfection cells were co-stained with aNRP2-10vl0, and a species agnostic anti-NRP2 al specific binding antibody. Cells were gated on live, single, NRP2 expressing cells (al binder positive), as shown in Figure 11A, and the degree of aNRP2-10vl0 staining was quantified as mean fluorescent intensity (MFI), as shown in Figure 11B.
- MFI mean fluorescent intensity
- Anchorage-independent growth is the ability of transformed cells to grow independently of a solid surface, and is a hallmark of carcinogenesis.
- the soft agar colony formation assay is a well- established method for characterizing this capability in vitro (J Vis Exp. 2014; (92): 51998).
- Human triple negative breast cancer (TNBC) cell lines MDA-MB-231 (HTB-26TM) and BT549 (HTB122TM) were obtained from ATCC and employed in this assay.
- MDA-MB-231 was cultured in lx RPMI media containing 10% FBS and 1% P/S.
- BT549 was cultured in lx RPMI media containing 10% FBS, 0.023 U/mL insulin and 1% P/S.
- Cells were recovered and expanded from frozen stocks for 2-3 passages.
- the NRP2-high population was sorted out on FACS equipment following cell surface staining by a fluorophore-conjugated anti-NRP2 antibody.
- the colony formation assay was performed using the soft agar colony formation fluorometric assay kit obtained from Cell Biolab (#CBA-130-CB).
- the sorted NRP2-high cells were suspended as single cell suspensions, and seeded at 1-1.5 K cells/96-well in the 3D soft agar matrix. After overnight incubation to stabilize the cells, the treatment reagents were spiked into the culture media. The chemo drug Cisplatin or 5-FU was added at a final concentration of IC30 or 1 ⁇ 2 IC30, based on a preliminary test that determined their inhibition curves on MDA-MB-231 cells, in combination with the antibodies a-NRP2-10vl0 or its isotype control hlgG4 at 100 nM. Reagents were renewed by spiking-in every 3 days. After 6 or 9 days of treatment, the soft agar matrix was dissolved and the formed cell colonies were quantified using CyQuant dye diluted in PBS (provided in the Cell Biolab kit), which produced a fluorescence signal proportional to viable cells.
- PBS Provided in the Cell Biolab kit
- NRP2-high population of TNBC cells were sorted for use in the colony formation assay because NRP2 is expressed preferentially on breast cancer stem cells (CSCs) and VEGF/NRP2 signaling was shown to be important for the genesis of TNBCs and tumor initiation (EMBO Mol Med. 20135(4):488-508).
- CSCs breast cancer stem cells
- VEGF/NRP2 signaling was shown to be important for the genesis of TNBCs and tumor initiation (EMBO Mol Med. 20135(4):488-508).
- the a-NRP2-10vl0 antibody in combination with either Cisplatin or 5-FU showed a significant inhibition of colony formation by MDA-MB-231 cells (Figure 13A). Similar effect was observed for the BT549 cells at certain doses of Cisplatin or 5-FU. ( Figure 13B).
- TNBC MDA-MB-231 cells revealed that >90% of these cells exhibit a cancer stem cell (CSC)-like phenotype (CD44+/CD24-), therefore we further performed the colony formation assay using parental MDA-MB-231 cells without pre-sorting.
- CSC cancer stem cell
- the matrix for 3D colony formation assay was changed to methylcellulose which is more solid, better mimics the extracellular matrix in vivo, and shows better signal-to-background than soft agar.
- Other experimental details are essentially the same as described in the previous example.
- aNRP2-10vl0 in combination with either the chemo drug Cisplatin or the anti-VEGF-A drug Bevacizumab, showed a significantly enhanced inhibition of colony formation by MDA-MB-231 cells, compared to either treatment with the isotype control hlgG4 antibody (see Figure 14).
- aNRP2-10vl0 thus significantly augments the effectiveness of both cisplatin and Bevacizumab in treating triple negative breast cancer.
- Migration assays were performed using a modified Boyden Chamber with 8mM pore size membrane, 16-well CIM plate (ACEA Biosciences.) Both sides of the membrane were coated with 5ug/ml Fibronectin (Sigma) for 30 minutes at 37°C, 5% CO2. 160mI of 191.5pM VEGF-C or assay medium (0.1% BSA, ECM) was added to the lower chamber, the upper well attached, 50ul assay medium added to the upper chamber before replacing the lid, and the plate was incubated for 1 hour at 37°C, 5% CO2 before baseline measurement was taken.
- HLECs were harvested, washed, and re-suspended in assay medium at 100,000 cells/well with aNRP2 antibody or control proteins and incubated for 30 minutes at 37°C, 5% C0 2 . Cells were added to the plate and incubated at room temperature for 30 minutes. Plate was inserted into xCELLigence RTCA DP (ACEA Biosciences) instrument, and migration was measured real-time every 5 minutes over a 24 hour period (2 wells per condition).
- HLECs were inhibited by both NRP2 antibodies to levels consistent with positive control antibodies (aKDR or 3C5) directed against VEGFR2 or VEGFR3 respectively.
- the treatment of cells with Sema3F should specifically block PI3K activity via NRP2 mediated interaction with plexin Al, thereby resulting in reduced phospho-Akt levels.
- lysates were prepared following standard protocols (MesoScale Discovery, Phospho(Ser473)/Total Akt Assay Whole Cell Lysate Kit #K15100D). Serum starved and confluent U251 cells (Sigma, Cat. 09063001) were treated with lOnM rapamycin (Sigma, Cat.
- mice Animals and Animal husbandry. All mice were ear tagged for identification purpose. Upon arrival, animals were examined to ensure that they were healthy. The animals were housed in autoclaved solid floor polycarbonate cages. Housing and sanitation were performed according to industry standards. All animal handling was performed in a laminar flow hood located in a clean room. In all experiments, euthanasia criteria were set for an upper limit on subcutaneous tumor volume (usually >2,000 mm 3 ) and body weight loss (usually > 20% body weight loss for an individual during the study). Animal work was performed at either Comparative Biosciences, Inc., 786 Lucerne Dr., Sunnyvale, CA 94085 or at aTyr Pharma, 3545 John Hopkins Court, Suite 250, San Diego, CA 92121. The test antibody dosing regimen was initiated once the mean tumor volume reached 50 - 100 mm 3 . Tumor measurements were recorded two times a week until study termination, as described below.
- Tumor monitoring Once palpable, sub-cutaneous tumors were measured three times a week with a digital caliper. Tumor volumes were calculated using formula:
- Tumor Volume length x width x width x 1 ⁇ 2
- Mouse B16-F10 cell line was purchased from ATCC. The cells were cultured in 75 cm 2 flasks containing DMEM media supplemented with 10% fetal bovine serum (FBS) and incubated at 37°C in humidified atmosphere of 5% CO2. As cells reached 90% confluence, cultures were expanded to 175 cm 2 flasks until sufficient cells are available for injection. 10,000 cancer cells in PBS with 20% matrigel were subcutaneously into the right flank of each mouse The day on which the tumor was implanted is designated as Day 0. Treatment Regimen. Thirty (30) C57BL/6 mice (Charles River, female, 6-8 wks old) were used in this study.
- FBS fetal bovine serum
- mice were assigned to 3 study groups of 10 mice randomly, and housed as described in the Materials and Methods.
- the antibody dosing regimen is shown in Table E4 below; in brief animals received intraperitoneal injections of the control IgG antibody, positive control antibody (Bevacizumab), and anti-NRP2 antibody (as described in the Materials and Methods), administered according to the protocol below (Table E4).
- Mouse 4T1 cell line was purchased from ATCC. The cells were cultured in 75 cm 2 flasks containing RPMI-1640 media supplemented with 10% FBS and incubated at 37°C in humidified atmosphere of 5% CC . As cells reached 90% confluence, cultures were expanded to 150 cm 2 flasks until sufficient cells are available for injection. 50,000 cancer cells in PBS were implanted subcutaneously into the right flank of each mouse.
- mice Twenty (20) Balb/c mice (Charles River, female, 5-6 wks old) were used in this study. The animals were assigned to 3 study groups of 10 mice randomly, and housed as described in the Materials and Methods. The antibody dosing regimen is shown in Table E5 below; in brief animals received intraperitoneal injections of 10 mg/kg of the control IgG antibody, and aNRP2- 28 (as described in the Materials and Methods), administered according to the protocol below (Table E5); starting one day before cancer cell implantation until termination on day 23).
- mice surrogate antibody aNRP2-28 which recognizes mouse NRP2 (to block endogenous mouse NRP2) in combination with the anti-human NRP2 antibody aNRP2-10vl0 (to block NRP2 on the human MDA-MB-231 cells) in combination with cisplatin in a human xenograft mouse model using MDA-MB-231 cells (Triple Negative Breast Cancer, TNBC cancer model).
- the dosing regimen was initiated when the mean tumor volume of all study animals reached 50 - 100 mm 3 .
- mice Twenty (20) NSG mice (Jackson Laboratory, female, 5-6 wks old) were used in this study. The animals were assigned to two study groups of 10 mice randomly. The MDA- MB-231 cell line was prepared for injection as described in the Materials and Methods. The dosing regimen is shown in Table E6 below; In brief animals received injections of 25 mg/kg of each the mouse surrogate antibody aNRP2-28 and aNRP2-10vl0 or IgG control, which were administered to mice intraperitoneally according to the protocol below (Table E6).
- Human MDA-MB-231 cell line was purchased from ATCC. The cells were cultured in 75 cm2 flasks containing DMEM media supplemented with 10% fetal bovine serum (FBS) and incubated at 37°C in humidified atmosphere of 5% C02. As cells reached 90% confluence, cultures were expanded to 175 cm2 flasks until sufficient cells are available for injection. 1.25 x 10 s cancer cells in PBS with 20% matrigel were injected orthotopically into the mammary fat pad. The day on which the tumor was implanted is designated as Day 0.
- FBS fetal bovine serum
- This study aimed to investigate the in vivo anticancer potential of aNRP2-10vl0 in combination with fluorouracil (5-FU) in a human xenograft mouse model using A549 cells (NSCLC cancer model).
- the dosing regimen was initiated when the mean tumor volume of all study animals reached 50 - 100 mm 3 on day 16.
- mice Twenty (20) Nu/J mice (Jackson Laboratory, female, 6 - 8 wks old) were used in this study. The animals were assigned to two study groups of 10 mice randomly. The A549 cell line was prepared for injection as described in the Materials and Methods. The dosing regimen is shown in Table E7 below; In brief animals received injections of 12.5 mg/kg of aNRP2-10 or IgG control, which were administered to mice intraperitoneally twice a week according to the protocol below (Table E7). Both groups also received 2.5 mg/kg of 5-FU three times a week.
- Human A549 cell line was purchased from ATCC. The cells were thawed and cultured in 75cm 2 flasks containing DMEM media supplemented with 10% FBS and incubated at 37°C in humidified atmosphere of 5% CO2. As cells reached 90% confluence, cultures were expanded to 150 cm 2 flasks until sufficient cells are available for injection. 2 x 10 s cancer cells in PBS with 20% matrigel were subcutaneously implanted into right flank of each mouse. The day on which the tumor was implanted is designated as Day 0.
- mice surrogate antibody aNRP2-28 which recognizes mouse NRP2 (and is a functional surrogate for anti-human NRP2 antibody aNRP2- lOvlO) it was tested in an experimental model of neovascularization.
- NV neovascularization
- mice were randomized into four groups, 10 mice per group.
- NV neovascularization
- mice were treated intraperitoneally with control IgG (Group 1), aNRP2-28 (Group 2) and Bevacizumab (Group 3) on post-injury Day 0, 3, 7 and 10.
- mice were monitored with daily clinical observations and weekly body weights. Additionally, ocular assessments of injured eyes were scored and photos taken on post-injury Day 7 and Day 14. All animals were euthanized on Day 14.
- Figures 23A-23B demonstrate that aNRP2-28 can inhibit neolymphangiogenesis in an experimental model of corneal injury.
- Figure 23A shows representative image scans of Lyve-1 stained corneas of the IgG control and aNRP2-28 group. Plotting the mean values of %Lye-l + area for each treatment group.
Landscapes
- Health & Medical Sciences (AREA)
- Chemical & Material Sciences (AREA)
- Life Sciences & Earth Sciences (AREA)
- Medicinal Chemistry (AREA)
- General Health & Medical Sciences (AREA)
- Organic Chemistry (AREA)
- Veterinary Medicine (AREA)
- Animal Behavior & Ethology (AREA)
- Pharmacology & Pharmacy (AREA)
- Public Health (AREA)
- Immunology (AREA)
- Nuclear Medicine, Radiotherapy & Molecular Imaging (AREA)
- General Chemical & Material Sciences (AREA)
- Chemical Kinetics & Catalysis (AREA)
- Epidemiology (AREA)
- Mycology (AREA)
- Proteomics, Peptides & Aminoacids (AREA)
- Genetics & Genomics (AREA)
- Molecular Biology (AREA)
- Biophysics (AREA)
- Engineering & Computer Science (AREA)
- Bioinformatics & Cheminformatics (AREA)
- Microbiology (AREA)
- Biochemistry (AREA)
- Endocrinology (AREA)
- Oncology (AREA)
- Peptides Or Proteins (AREA)
- Medicines Containing Antibodies Or Antigens For Use As Internal Diagnostic Agents (AREA)
- Micro-Organisms Or Cultivation Processes Thereof (AREA)
- Inorganic Chemistry (AREA)
- Medicinal Preparation (AREA)
- Medicines That Contain Protein Lipid Enzymes And Other Medicines (AREA)
- Apparatus Associated With Microorganisms And Enzymes (AREA)
Abstract
Description










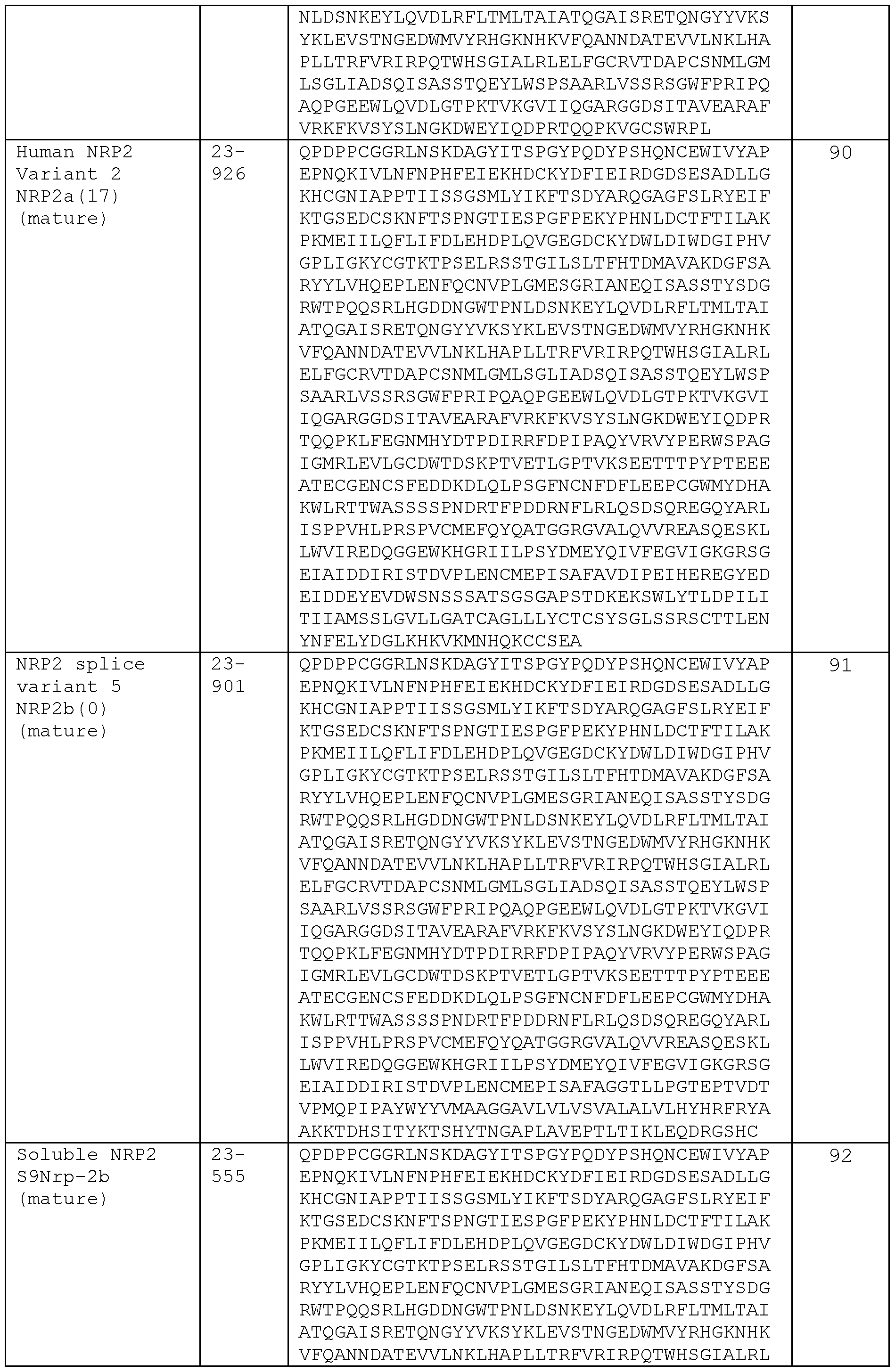










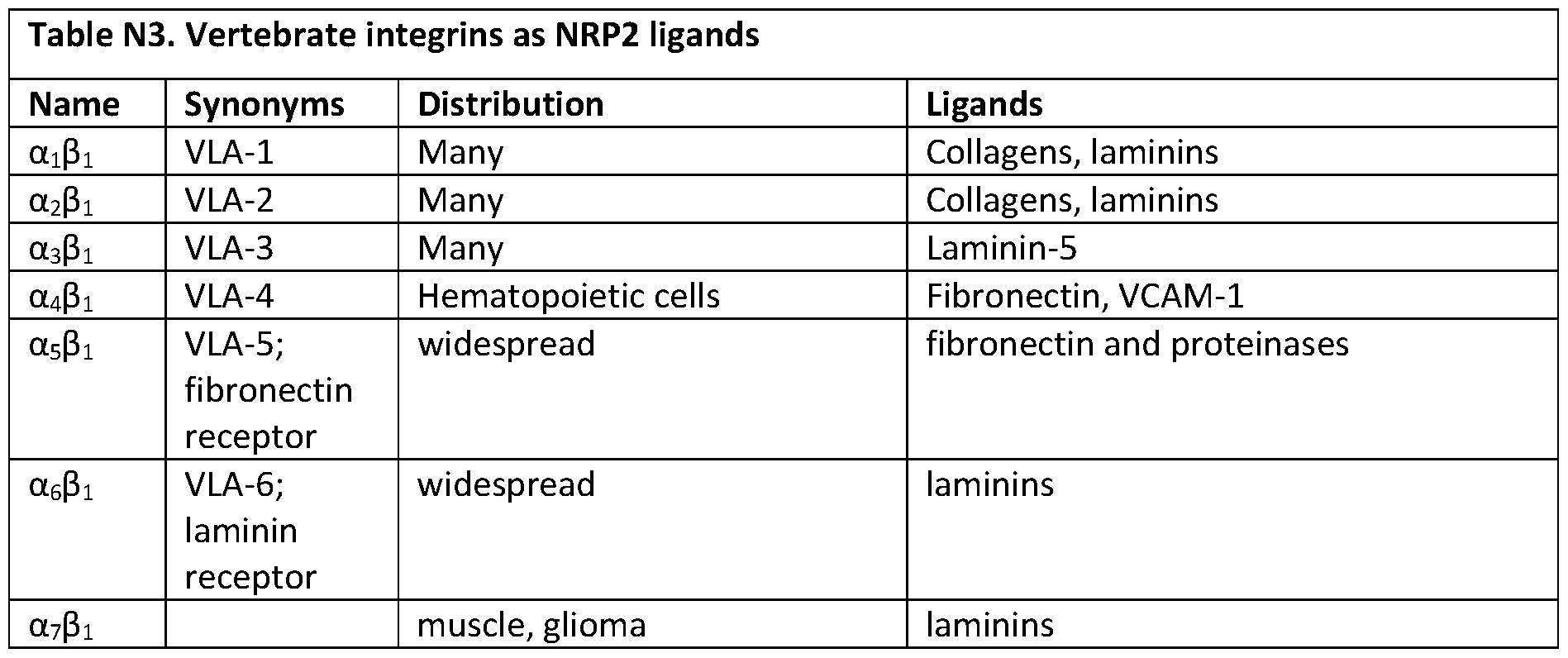











Claims
Priority Applications (5)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| AU2020358854A AU2020358854A1 (en) | 2019-10-03 | 2020-10-02 | Compositions and methods comprising anti-NRP2 antibodies |
| CN202080084174.4A CN114746120A (en) | 2019-10-03 | 2020-10-02 | Compositions and methods comprising anti-NRP 2 antibodies |
| EP20870841.2A EP4037711A4 (en) | 2019-10-03 | 2020-10-02 | Compositions and methods comprising anti-nrp2 antibodies |
| JP2022520527A JP2022551603A (en) | 2019-10-03 | 2020-10-02 | Compositions and methods comprising anti-NRP2 antibodies |
| CA3156803A CA3156803A1 (en) | 2019-10-03 | 2020-10-02 | Compositions and methods comprising anti-nrp2 antibodies |
Applications Claiming Priority (4)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| US201962910042P | 2019-10-03 | 2019-10-03 | |
| US62/910,042 | 2019-10-03 | ||
| US202063024960P | 2020-05-14 | 2020-05-14 | |
| US63/024,960 | 2020-05-14 |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| WO2021067761A1 true WO2021067761A1 (en) | 2021-04-08 |
Family
ID=75338623
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| PCT/US2020/054017 WO2021067761A1 (en) | 2019-10-03 | 2020-10-02 | Compositions and methods comprising anti-nrp2 antibodies |
Country Status (7)
| Country | Link |
|---|---|
| US (2) | US11807687B2 (en) |
| EP (1) | EP4037711A4 (en) |
| JP (1) | JP2022551603A (en) |
| CN (1) | CN114746120A (en) |
| AU (1) | AU2020358854A1 (en) |
| CA (1) | CA3156803A1 (en) |
| WO (1) | WO2021067761A1 (en) |
Cited By (3)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US11505610B2 (en) | 2018-04-06 | 2022-11-22 | Atyr Pharma, Inc. | Compositions and methods comprising anti-NRP2 antibodies |
| WO2023164610A3 (en) * | 2022-02-25 | 2023-09-28 | Atyr Pharma, Inc. | Compositions and methods comprising anti-nrp2b antibodies |
| US11807687B2 (en) | 2019-10-03 | 2023-11-07 | Atyr Pharma, Inc. | Therapeutic compositions comprising anti-NRP2 antibodies |
Families Citing this family (3)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| EP3710471A1 (en) * | 2017-11-16 | 2020-09-23 | Kite Pharma, Inc. | Modified chimeric antigen receptors and methods of use |
| WO2023164689A2 (en) * | 2022-02-28 | 2023-08-31 | University Of Massachusetts | Targeting neuropilin 2 (nrp2) in lethal prostate cancer |
| WO2023245117A2 (en) * | 2022-06-17 | 2023-12-21 | Atyr Pharma, Inc. | Compositions and methods comprising anti-nrp2 antibodies |
Citations (22)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US20020127227A1 (en) * | 1998-11-19 | 2002-09-12 | Smithkline Beecham Corporation | RHAMM antagonist antibodies |
| US20030045691A1 (en) * | 1996-10-04 | 2003-03-06 | Koichiro Ono | Reshaped human anti-hm 1.24 antibody |
| US20030088075A1 (en) * | 1996-11-21 | 2003-05-08 | Kyowa Hakko Kogyo Co., Ltd. | Anti-human VEGF receptor Flt-1 monoclonal antibody |
| US20040005647A1 (en) * | 2001-03-30 | 2004-01-08 | The Regents Of The University Of California | Anti-MUC-1 single chain antibodies for tumor targeting |
| US20040028685A1 (en) * | 2002-05-10 | 2004-02-12 | Kinch Michael S. | EphA2 monoclonal antibodies and methods of use thereof |
| US20040038339A1 (en) * | 2000-03-24 | 2004-02-26 | Peter Kufer | Multifunctional polypeptides comprising a binding site to an epitope of the nkg2d receptor complex |
| US20050064518A1 (en) * | 2002-10-16 | 2005-03-24 | Albone Earl F. | Antibodies that bind cell-associated CA 125/O772P and methods of use thereof |
| US20060280747A1 (en) * | 2003-08-01 | 2006-12-14 | Genentech, Inc. | Anti-VEGF antibodies |
| US20070189962A1 (en) * | 2003-11-25 | 2007-08-16 | The Gov.Of Us, As Represented By The Sec.Of Health | Mutated anti-cd22 antibodies and immunoconjugates |
| US20090196850A1 (en) * | 2005-01-06 | 2009-08-06 | Novo Nordisk A/S | Anti-Kir Combination Treatments and Methods |
| US20100310573A1 (en) * | 2008-12-26 | 2010-12-09 | Kyowa Hakko Kirin Co., Ltd. | Anti-cd4 antibody |
| US20110243932A1 (en) * | 2010-03-31 | 2011-10-06 | Boehringer Ingelheim International Gmbh | Anti-cd40 antibodies |
| US20120282637A1 (en) * | 2009-10-09 | 2012-11-08 | Sanofi | Polypeptides for binding to the receptor for advanced glycation endproducts as well as compositions and methods involving |
| US20130266517A1 (en) * | 2012-01-27 | 2013-10-10 | Neotope Biosciences Limited | Humanized Antibodies That Recognize Alpha-Synuclein |
| US20140234312A1 (en) * | 2007-05-17 | 2014-08-21 | Genentech, Inc. | Inhibition of tumor metastasis |
| US20150218267A1 (en) * | 2014-01-31 | 2015-08-06 | Boehringer Ingelheim International Gmbh | Novel anti-baff antibodies |
| US20160017041A1 (en) * | 2013-03-15 | 2016-01-21 | Biogen Ma Inc. | Treatment and prevention of acute kidney injury using anti-alpha v beta 5 antibodies |
| US20160046711A1 (en) * | 2014-08-12 | 2016-02-18 | Novartis Ag | Anti-cdh6 antibody drug conjugates |
| US20160108113A1 (en) * | 2014-10-16 | 2016-04-21 | Genentech, Inc. | Anti-alpha-synuclein antibodies and methods of use |
| WO2017205377A2 (en) * | 2016-05-23 | 2017-11-30 | New York University | Compositions and methods for antibodies targeting staphylococcal leukotoxins |
| US20180193454A1 (en) * | 2015-07-14 | 2018-07-12 | Immunext, Inc. | Anti-cd154 antibody having improved binding, functional and safety characteristics and use in human immunotherapy |
| WO2019075472A1 (en) * | 2017-10-13 | 2019-04-18 | A&G Pharmaceutical, Inc. | Monoclonal antibodies and conjugates against prostaglandin f2 receptor inhibitor and uses thereof |
Family Cites Families (37)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US6428965B1 (en) | 1997-07-17 | 2002-08-06 | The Johns Hopkins University | Screening assays for the interaction of semaphorins and neuropilins |
| WO1999029858A1 (en) | 1997-12-09 | 1999-06-17 | Children's Medical Center Corporation | Soluble inhibitors of vascular endothelial growth factor and use thereof |
| WO1999030157A2 (en) | 1997-12-09 | 1999-06-17 | Children's Medical Center Corporation | Neuropilins in methods for diagnosis and prognosis of cancer |
| AU1810499A (en) | 1997-12-09 | 1999-06-28 | Children's Medical Center Corporation | Antagonists of neuropilin receptor functional and use thereof |
| US20030113324A1 (en) | 2001-10-01 | 2003-06-19 | Kari Alitalo | Neuropilin/VEGF-C/VEGFR-3 materials and methods |
| US20080045469A1 (en) | 2004-04-16 | 2008-02-21 | Yihali Cao | Compositions and Methods for Inhibiting Angiogenesis |
| EP1739092A1 (en) | 2005-06-28 | 2007-01-03 | I.N.S.E.R.M. Institut National de la Sante et de la Recherche Medicale | Peptidic antagonists of class III semaphorins/neuropilins complexes |
| CA2636367A1 (en) | 2005-07-18 | 2007-01-25 | Trustees Of Boston University | Method to inhibit proliferation and growth of metastases |
| EP1915170A1 (en) | 2005-08-16 | 2008-04-30 | Klinikum der Universität Regensburg | Use of neuropilin-2 antagonists |
| UA96139C2 (en) * | 2005-11-08 | 2011-10-10 | Дженентек, Інк. | Anti-neuropilin-1 (nrp1) antibody |
| US7420041B2 (en) | 2006-02-24 | 2008-09-02 | Arius Research Inc. | Cytotoxicity mediation of cells evidencing surface expression of TROP-2 |
| EP2639316A1 (en) | 2007-05-11 | 2013-09-18 | The Johns Hopkins University | Biomarkers for melanoma |
| US8318163B2 (en) | 2007-05-17 | 2012-11-27 | Genentech, Inc. | Anti-pan neuropilin antibody and binding fragments thereof |
| AR068723A1 (en) | 2007-10-05 | 2009-12-02 | Glaxo Group Ltd | PROTEIN THAT JOINS ANTIGENS THAT JOINS HUMAN IL-23 AND ITS USES |
| BRPI0909541A2 (en) | 2008-05-27 | 2016-10-11 | Pluristem Ltd | '' method for treating inflammatory bowel disease '' |
| FR2935385B1 (en) | 2008-08-27 | 2013-04-19 | Diaclone | INDUCTION OF P53 EXPRESSION BY NEUTRALIZATION OF NEUROPILIN-2 FOR THE TREATMENT OF CANCERS |
| EP2810652A3 (en) | 2009-03-05 | 2015-03-11 | AbbVie Inc. | IL-17 binding proteins |
| CA2755784C (en) | 2009-03-16 | 2020-03-24 | Pangu Biopharma Limited | Compositions and methods comprising histidyl-trna synthetase splice variants having non-canonical biological activities |
| DK2419447T3 (en) | 2009-04-17 | 2017-09-25 | Immunas Pharma Inc | ANTIBODIES THAT SPECIFICALLY BIND TO A BETA OLIGOMER AND USE THEREOF |
| AU2010292060A1 (en) | 2009-09-11 | 2012-04-12 | Genentech, Inc. | Method to identify a patient with an increased likelihood of responding to an anti-cancer agent |
| CN102667484A (en) | 2009-10-13 | 2012-09-12 | 约翰·霍普金斯大学 | Biomarker for identification of melanoma tumor cells |
| WO2012144208A1 (en) | 2011-04-18 | 2012-10-26 | 国立大学法人東京大学 | Diagnosis and treatment of cancer using anti-itm2a antibody |
| WO2013116742A1 (en) | 2012-02-01 | 2013-08-08 | Mayo Foundation For Medical Education And Research | Predicting responses to androgen deprivation therapy and methods for treating prostate cancer |
| WO2014105810A1 (en) | 2012-12-24 | 2014-07-03 | Abbvie Inc. | Prolactin receptor binding proteins and uses thereof |
| WO2014125291A1 (en) | 2013-02-14 | 2014-08-21 | Ucl Business Plc | Agents which induce lymphangiogenesis for use in the treatment of cystic kidney disease |
| CA2907046C (en) | 2013-03-15 | 2021-04-20 | Atyr Pharma, Inc. | Histidyl-trna synthetase-fc conjugates |
| WO2015095686A1 (en) | 2013-12-20 | 2015-06-25 | Trustees Of Boston University | Assays and methods relating to the treatment of melanoma |
| EP3116906A1 (en) | 2014-03-12 | 2017-01-18 | Prothena Biosciences Limited | Anti-laminin4 antibodies specific for lg1-3 |
| JP2017518307A (en) | 2014-06-02 | 2017-07-06 | チルドレンズ メディカル センター コーポレーション | Methods and compositions for immunomodulation |
| CA3045321A1 (en) * | 2016-11-30 | 2018-06-07 | Atyr Pharma, Inc. | Anti-hrs antibodies and combination therapies for treating cancers |
| EP3704136A1 (en) | 2017-10-30 | 2020-09-09 | Miltenyi Biotec B.V. & Co. KG | Adapter-based retroviral vector system for the selective transduction of target cells |
| CN113226367A (en) | 2018-04-06 | 2021-08-06 | Atyr 医药公司 | Compositions and methods comprising anti-NRP 2 antibodies |
| BR112021019135A2 (en) | 2019-04-01 | 2021-11-30 | Jiangsu Hengrui Medicine Co | Anti-claudin antibody 18.2 and its application |
| WO2021058548A1 (en) | 2019-09-23 | 2021-04-01 | Centro Nacional De Investigaciones Cardiovasculares Carlos Iii (F.S.P.) | Antibodies for the diagnosis and/or treatment of atherosclerosis |
| CA3156803A1 (en) | 2019-10-03 | 2021-04-08 | Atyr Pharma, Inc. | Compositions and methods comprising anti-nrp2 antibodies |
| CN116075525A (en) | 2020-03-31 | 2023-05-05 | 艾莱克特有限责任公司 | anti-MERTK antibodies and methods of use thereof |
| WO2023076998A1 (en) | 2021-10-27 | 2023-05-04 | Atyr Pharma, Inc. | COMPOSITIONS AND METHODS COMPRISING ANTI-NRP2a ANTIBODIES |
-
2020
- 2020-10-02 CA CA3156803A patent/CA3156803A1/en active Pending
- 2020-10-02 EP EP20870841.2A patent/EP4037711A4/en active Pending
- 2020-10-02 AU AU2020358854A patent/AU2020358854A1/en active Pending
- 2020-10-02 US US17/062,100 patent/US11807687B2/en active Active
- 2020-10-02 JP JP2022520527A patent/JP2022551603A/en active Pending
- 2020-10-02 CN CN202080084174.4A patent/CN114746120A/en active Pending
- 2020-10-02 WO PCT/US2020/054017 patent/WO2021067761A1/en unknown
-
2023
- 2023-09-28 US US18/477,113 patent/US20240092917A1/en active Pending
Patent Citations (22)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US20030045691A1 (en) * | 1996-10-04 | 2003-03-06 | Koichiro Ono | Reshaped human anti-hm 1.24 antibody |
| US20030088075A1 (en) * | 1996-11-21 | 2003-05-08 | Kyowa Hakko Kogyo Co., Ltd. | Anti-human VEGF receptor Flt-1 monoclonal antibody |
| US20020127227A1 (en) * | 1998-11-19 | 2002-09-12 | Smithkline Beecham Corporation | RHAMM antagonist antibodies |
| US20040038339A1 (en) * | 2000-03-24 | 2004-02-26 | Peter Kufer | Multifunctional polypeptides comprising a binding site to an epitope of the nkg2d receptor complex |
| US20040005647A1 (en) * | 2001-03-30 | 2004-01-08 | The Regents Of The University Of California | Anti-MUC-1 single chain antibodies for tumor targeting |
| US20040028685A1 (en) * | 2002-05-10 | 2004-02-12 | Kinch Michael S. | EphA2 monoclonal antibodies and methods of use thereof |
| US20050064518A1 (en) * | 2002-10-16 | 2005-03-24 | Albone Earl F. | Antibodies that bind cell-associated CA 125/O772P and methods of use thereof |
| US20060280747A1 (en) * | 2003-08-01 | 2006-12-14 | Genentech, Inc. | Anti-VEGF antibodies |
| US20070189962A1 (en) * | 2003-11-25 | 2007-08-16 | The Gov.Of Us, As Represented By The Sec.Of Health | Mutated anti-cd22 antibodies and immunoconjugates |
| US20090196850A1 (en) * | 2005-01-06 | 2009-08-06 | Novo Nordisk A/S | Anti-Kir Combination Treatments and Methods |
| US20140234312A1 (en) * | 2007-05-17 | 2014-08-21 | Genentech, Inc. | Inhibition of tumor metastasis |
| US20100310573A1 (en) * | 2008-12-26 | 2010-12-09 | Kyowa Hakko Kirin Co., Ltd. | Anti-cd4 antibody |
| US20120282637A1 (en) * | 2009-10-09 | 2012-11-08 | Sanofi | Polypeptides for binding to the receptor for advanced glycation endproducts as well as compositions and methods involving |
| US20110243932A1 (en) * | 2010-03-31 | 2011-10-06 | Boehringer Ingelheim International Gmbh | Anti-cd40 antibodies |
| US20130266517A1 (en) * | 2012-01-27 | 2013-10-10 | Neotope Biosciences Limited | Humanized Antibodies That Recognize Alpha-Synuclein |
| US20160017041A1 (en) * | 2013-03-15 | 2016-01-21 | Biogen Ma Inc. | Treatment and prevention of acute kidney injury using anti-alpha v beta 5 antibodies |
| US20150218267A1 (en) * | 2014-01-31 | 2015-08-06 | Boehringer Ingelheim International Gmbh | Novel anti-baff antibodies |
| US20160046711A1 (en) * | 2014-08-12 | 2016-02-18 | Novartis Ag | Anti-cdh6 antibody drug conjugates |
| US20160108113A1 (en) * | 2014-10-16 | 2016-04-21 | Genentech, Inc. | Anti-alpha-synuclein antibodies and methods of use |
| US20180193454A1 (en) * | 2015-07-14 | 2018-07-12 | Immunext, Inc. | Anti-cd154 antibody having improved binding, functional and safety characteristics and use in human immunotherapy |
| WO2017205377A2 (en) * | 2016-05-23 | 2017-11-30 | New York University | Compositions and methods for antibodies targeting staphylococcal leukotoxins |
| WO2019075472A1 (en) * | 2017-10-13 | 2019-04-18 | A&G Pharmaceutical, Inc. | Monoclonal antibodies and conjugates against prostaglandin f2 receptor inhibitor and uses thereof |
Non-Patent Citations (2)
| Title |
|---|
| DATABASE UniProtKB [online] 2 November 2016 (2016-11-02), Database accession no. A0A1C0YHR0 * |
| See also references of EP4037711A4 * |
Cited By (3)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US11505610B2 (en) | 2018-04-06 | 2022-11-22 | Atyr Pharma, Inc. | Compositions and methods comprising anti-NRP2 antibodies |
| US11807687B2 (en) | 2019-10-03 | 2023-11-07 | Atyr Pharma, Inc. | Therapeutic compositions comprising anti-NRP2 antibodies |
| WO2023164610A3 (en) * | 2022-02-25 | 2023-09-28 | Atyr Pharma, Inc. | Compositions and methods comprising anti-nrp2b antibodies |
Also Published As
| Publication number | Publication date |
|---|---|
| US11807687B2 (en) | 2023-11-07 |
| JP2022551603A (en) | 2022-12-12 |
| US20210163606A1 (en) | 2021-06-03 |
| CA3156803A1 (en) | 2021-04-08 |
| EP4037711A4 (en) | 2024-02-14 |
| EP4037711A1 (en) | 2022-08-10 |
| AU2020358854A1 (en) | 2022-05-26 |
| US20240092917A1 (en) | 2024-03-21 |
| CN114746120A (en) | 2022-07-12 |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| US20230312730A1 (en) | Compositions and methods comprising anti-nrp2 antibodies | |
| US11807687B2 (en) | Therapeutic compositions comprising anti-NRP2 antibodies | |
| US20180282402A1 (en) | Anti-hrs antibodies and combinaton therapies for treating cancers | |
| RU2725811C1 (en) | Anti-human 4-1bb antibodies and use thereof | |
| CA3136491A1 (en) | Anti-cd40 antibodies and uses thereof | |
| WO2023076998A1 (en) | COMPOSITIONS AND METHODS COMPRISING ANTI-NRP2a ANTIBODIES | |
| US20230257453A1 (en) | Collagen-targeted fusion proteins and antibodies | |
| EP3882271A2 (en) | Ifn-gamma-inducible regulatory t cell convertible anti-cancer (irtca) antibody and uses thereof | |
| WO2023164610A2 (en) | Compositions and methods comprising anti-nrp2b antibodies | |
| US20230250193A1 (en) | Antibodies to fibroblast activation protein and b7h3 | |
| WO2022156726A1 (en) | Methods of cancer treatment using anti-tigit antibodies in combination with anti-pd1 antibodies | |
| RU2777573C2 (en) | Antibodies against human 4-1bb and their use | |
| CA3205839A1 (en) | Methods of cancer treatment using anti-tigit antibodies in combination with anti-pd1 antibodies | |
| KR20220103105A (en) | Method for treating cancer using anti-OX40 antibody in combination with anti-TIM3 antibody |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| 121 | Ep: the epo has been informed by wipo that ep was designated in this application |
Ref document number: 20870841 Country of ref document: EP Kind code of ref document: A1 |
|
| ENP | Entry into the national phase |
Ref document number: 2022520527 Country of ref document: JP Kind code of ref document: A Ref document number: 3156803 Country of ref document: CA |
|
| NENP | Non-entry into the national phase |
Ref country code: DE |
|
| ENP | Entry into the national phase |
Ref document number: 2020870841 Country of ref document: EP Effective date: 20220503 |
|
| ENP | Entry into the national phase |
Ref document number: 2020358854 Country of ref document: AU Date of ref document: 20201002 Kind code of ref document: A |