WO2016176208A1 - Compositions of obeticholic acid and methods of use - Google Patents
Compositions of obeticholic acid and methods of use Download PDFInfo
- Publication number
- WO2016176208A1 WO2016176208A1 PCT/US2016/029369 US2016029369W WO2016176208A1 WO 2016176208 A1 WO2016176208 A1 WO 2016176208A1 US 2016029369 W US2016029369 W US 2016029369W WO 2016176208 A1 WO2016176208 A1 WO 2016176208A1
- Authority
- WO
- WIPO (PCT)
- Prior art keywords
- obeticholic acid
- composition
- particles
- patient
- less
- Prior art date
Links
Classifications
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/56—Compounds containing cyclopenta[a]hydrophenanthrene ring systems; Derivatives thereof, e.g. steroids
- A61K31/575—Compounds containing cyclopenta[a]hydrophenanthrene ring systems; Derivatives thereof, e.g. steroids substituted in position 17 beta by a chain of three or more carbon atoms, e.g. cholane, cholestane, ergosterol, sitosterol
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K45/00—Medicinal preparations containing active ingredients not provided for in groups A61K31/00 - A61K41/00
- A61K45/06—Mixtures of active ingredients without chemical characterisation, e.g. antiphlogistics and cardiaca
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K47/00—Medicinal preparations characterised by the non-active ingredients used, e.g. carriers or inert additives; Targeting or modifying agents chemically bound to the active ingredient
- A61K47/50—Medicinal preparations characterised by the non-active ingredients used, e.g. carriers or inert additives; Targeting or modifying agents chemically bound to the active ingredient the non-active ingredient being chemically bound to the active ingredient, e.g. polymer-drug conjugates
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K9/00—Medicinal preparations characterised by special physical form
- A61K9/14—Particulate form, e.g. powders, Processes for size reducing of pure drugs or the resulting products, Pure drug nanoparticles
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K9/00—Medicinal preparations characterised by special physical form
- A61K9/14—Particulate form, e.g. powders, Processes for size reducing of pure drugs or the resulting products, Pure drug nanoparticles
- A61K9/16—Agglomerates; Granulates; Microbeadlets ; Microspheres; Pellets; Solid products obtained by spray drying, spray freeze drying, spray congealing,(multiple) emulsion solvent evaporation or extraction
- A61K9/1605—Excipients; Inactive ingredients
- A61K9/1617—Organic compounds, e.g. phospholipids, fats
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K9/00—Medicinal preparations characterised by special physical form
- A61K9/14—Particulate form, e.g. powders, Processes for size reducing of pure drugs or the resulting products, Pure drug nanoparticles
- A61K9/16—Agglomerates; Granulates; Microbeadlets ; Microspheres; Pellets; Solid products obtained by spray drying, spray freeze drying, spray congealing,(multiple) emulsion solvent evaporation or extraction
- A61K9/1605—Excipients; Inactive ingredients
- A61K9/1629—Organic macromolecular compounds
- A61K9/1652—Polysaccharides, e.g. alginate, cellulose derivatives; Cyclodextrin
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K9/00—Medicinal preparations characterised by special physical form
- A61K9/20—Pills, tablets, discs, rods
- A61K9/2004—Excipients; Inactive ingredients
- A61K9/2022—Organic macromolecular compounds
- A61K9/205—Polysaccharides, e.g. alginate, gums; Cyclodextrin
- A61K9/2054—Cellulose; Cellulose derivatives, e.g. hydroxypropyl methylcellulose
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K9/00—Medicinal preparations characterised by special physical form
- A61K9/20—Pills, tablets, discs, rods
- A61K9/2004—Excipients; Inactive ingredients
- A61K9/2022—Organic macromolecular compounds
- A61K9/205—Polysaccharides, e.g. alginate, gums; Cyclodextrin
- A61K9/2059—Starch, including chemically or physically modified derivatives; Amylose; Amylopectin; Dextrin
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K9/00—Medicinal preparations characterised by special physical form
- A61K9/20—Pills, tablets, discs, rods
- A61K9/2072—Pills, tablets, discs, rods characterised by shape, structure or size; Tablets with holes, special break lines or identification marks; Partially coated tablets; Disintegrating flat shaped forms
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P1/00—Drugs for disorders of the alimentary tract or the digestive system
- A61P1/16—Drugs for disorders of the alimentary tract or the digestive system for liver or gallbladder disorders, e.g. hepatoprotective agents, cholagogues, litholytics
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P31/00—Antiinfectives, i.e. antibiotics, antiseptics, chemotherapeutics
- A61P31/12—Antivirals
- A61P31/14—Antivirals for RNA viruses
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P43/00—Drugs for specific purposes, not provided for in groups A61P1/00-A61P41/00
-
- C—CHEMISTRY; METALLURGY
- C07—ORGANIC CHEMISTRY
- C07J—STEROIDS
- C07J9/00—Normal steroids containing carbon, hydrogen, halogen or oxygen substituted in position 17 beta by a chain of more than two carbon atoms, e.g. cholane, cholestane, coprostane
- C07J9/005—Normal steroids containing carbon, hydrogen, halogen or oxygen substituted in position 17 beta by a chain of more than two carbon atoms, e.g. cholane, cholestane, coprostane containing a carboxylic function directly attached or attached by a chain containing only carbon atoms to the cyclopenta[a]hydrophenanthrene skeleton
Definitions
- the farnesoid X receptor also known as the bile acid receptor (BAR) or NR1H4, is a member of the nuclear receptor superfamily of ligand-activated transcription factors. FXR forms with retinoid X receptor (RXR) a heterodimer receptor crucial for bile acid homeostasis. FXR is expressed in various tissues including the liver, kidney, intestine, colon, ovary, and adrenal gland, and is activated by a variety of naturally occurring bile acids, including the primary bile acid chenodeoxycholic acid (CDCA) and its taurine and glycine conjugates. Upon activation, the FXR-RXR heterodimer binds the promoter region of target genes and regulates their expression.
- DCA primary bile acid chenodeoxycholic acid
- 6-Ethyl-chenodeoxycholic acid (6-ECDCA, or obeticholic acid, or OCA), a bile acid derivative, shows a potent FXR activating activity, and accordingly offers great promise for the treatment of FXR-mediated diseases or conditions.
- 6-Ethyl-chenodeoxycholic acid (6-ECDCA, or obeticholic acid, or OCA)
- OCA obeticholic acid
- the present disclosure relates to novel formulations of obeticholic acid, an FXR agonist, with improved stability, dissolution, and solubility, methods of preparing the same and methods of using the novel formulations for treating a disease or condition.
- the disease or condition is primary biliary cirrhosis (PBC), also known as primary biliary cholangitis.
- PBC primary biliary cirrhosis
- the disease or condition is primary sclerosing cholangitis (PSC), chronic liver disease, nonalcoholic fatty liver disease (NAFLD), nonalcoholic steatohepatitis (NASH), hepatitis C infection, alcoholic liver disease, liver damage due to progressive fibrosis, or liver fibrosis.
- the disease is NASH.
- the disease or condition is solid-tumor cancer such as, for example, hepatocellular carcinoma (HCC), colorectal cancer, gastric cancer, liver cancer, breast cancer, kidney cancer, or pancreatic cancer.
- HCC hepatocellular carcinoma
- colorectal cancer gastric cancer
- liver cancer breast cancer
- kidney cancer pancreatic cancer
- pancreatic cancer pancreatic cancer
- a first aspect of the disclosure relates to a composition
- a composition comprising obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, wherein obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is in the form of particles, and wherein at least 50% of the particles have a diameter of less than 200 ⁇ m .
- Such compositions include all those described herein.
- Another aspect of the disclosure relates to treating a disease or condition described herein in a patient in need thereof by administering a composition that includes obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, where the obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is in the form of particles.
- Another aspect of the disclosure relates to treating a disease or condition described herein in a patient in need thereof by administering a composition that includes obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, where the obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is in the form of particles, and wherein at least 50% of the particles have a diameter of 200 ⁇ m or less.
- Another aspect of the disclosure relates to treating primary biliary cirrhosis (PBC) in a patient in need thereof by administering a composition that includes obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, optionally in a titration period, where the obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is in the form of particles, and wherein at least 50% of the particles have a diameter of 200 ⁇ m or less.
- PBC primary biliary cirrhosis
- a method of treating primary sclerosing cholangitis (PSC), chronic liver disease, nonalcoholic fatty liver disease (NAFLD), nonalcoholic steatohepatitis (NASH), hepatitis C infection, alcoholic liver disease, liver damage due to progressive fibrosis, or liver fibrosis in a patient in need thereof by administering a composition that includes obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, optionally in a titration period, where the obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is in the form of particles. In one example, at least 50% of the particles have a diameter of 200 ⁇ m or less.
- in yet another aspect of the disclosure is a method of treating a solid-tumor cancer in a patient in need thereof by administering a composition that includes obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, optionally in a titration period, where the obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is in the form of particles.
- a composition that includes obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, optionally in a titration period, where the obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is in the form of particles.
- at least 50% of the particles have a diameter of 200 ⁇ m or less.
- a method of treating an autoimmune disease in a patient in need thereof by administering a composition that obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, optionally in a titration period, where the obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is in the form of particles.
- a composition that obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is in the form of particles.
- at least 50% of the particles have a diameter of 200 ⁇ m or less.
- obeticholic acid compositions described herein are administered as part of a treatment regimen that includes a titration period and a starting dose of the obeticholic acid composition at an amount of about 5 mg or 10 mg.
- methods include daily (QD) administration of an obeticholic acid described herein during the titration period.
- QD daily
- methods also include administration of an adjusted dose of an obeticholic acid composition described herein after the titration period.
- compositions comprising obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, wherein obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is in the form of particles, and wherein at least 50% of the particles have a diameter of less than 200 ⁇ m .
- a composition comprising obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, and a pharmaceutically acceptable excipient (e.g. , sodium starch glycolate) having a low alcohol (e.g. , ethanol or methanol) content (e.g., less than 5% (wt/wt)).
- the disclosure relates to a pharmaceutical composition, comprising a therapeutically effective amount of obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, in the form of particles, and a pharmaceutically acceptable excipient (e.g., sodium starch glycolate) having a low alcohol (e.g. , ethanol or methanol) content (e.g. , less than 5% (wt/wt)), wherein at least 50% of the particles have a diameter of less than 200 ⁇ m.
- a pharmaceutically acceptable excipient e.g., sodium starch glycolate
- a low alcohol e.g. , ethanol or methanol
- compositions comprising obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, in the form of particles, wherein at least 50% of the particles have a diameter of less than 200 ⁇ m, at about 1% to about 6% by weight, sodium starch glycolate at about 2% to about 8 % by weight having a low alcohol (e.g. , ethanol or methanol) content (e.g.
- a low alcohol e.g. , ethanol or methanol
- a lubricant e.g., magnesium stearate
- a diluent e.g., microcrystalline cellulose
- the disclosure relates to a method for preparing a composition comprising obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, in the form of particles, wherein at least 50% of the particles have a diameter of less than 200 ⁇ , comprising forming the particles through jet-milling.
- Another aspect of the disclosure relates to a tablet comprising an intra-granular portion and an extra-granular portion, the intra-granular portion comprising obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, microcrystalline cellulose, and one or more additional pharmaceutical excipients, and the extra-granular portion comprising one or more pharmaceutical excipients.
- Another aspect of the disclosure relates to a tablet comprising an intra-granular portion and an extra-granular portion, the intra-granular portion comprising obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, microcrystalline cellulose, and one or more additional pharmaceutical excipients, and the extra-granular portion comprising microcrystalline cellulose and one or more additional pharmaceutical excipients.
- the disclosure relates to methods for treating or preventing an FXR mediated disease or condition or a disease or condition in which elevated concentrations of circulating lipid compounds or glucose in the blood, or decreased insulin level, or increased insulin resistance is involved, or inhibiting or reversing fibrosis, comprising administering a therapeutically effective amount of a composition of the present disclosure to a subject in need thereof.
- Another aspect of the disclosure relates to use of a composition of the present disclosure for treating or preventing an FXR mediated disease or condition or a disease or condition in which elevated concentrations of circulating lipid compounds or glucose in the blood, or decreased insulin level, or increased insulin resistance is involved, or for inhibiting or reversing fibrosis.
- the disclosure relates to use of a composition of the present disclosure in the manufacture of a medicament for treating or preventing an FXR mediated disease or condition or a disease or condition in which elevated concentrations of circulating lipid compounds or glucose in the blood, or decreased insulin level, or increased insulin resistance is involved, or for inhibiting or reversing fibrosis.
- compositions and methods of the present disclosure address unmet needs in the treatment or prevention of an FXR mediated disease or a disease or disorder in which elevated concentrations of circulating lipid compounds in the blood such as cholesterol and triglycerides or glucose are involved.
- compositions and methods of the present disclosure address unmet needs in the treatment of diseases and conditions described herein, including for example, PBC, PSC, NAFLD, NASH, cancer, and autoimmune diseases described herein.
- FIG. 1 is a particle size distribution histogram of obeticholic acid before jet- milling.
- FIG. 2 is a particle size distribution histogram of obeticholic acid after jet-milling.
- FIG. 3 is a graph showing the dissolution profile of 10 mg tablets containing unmilled/non-agglomerated, unmilled/agglomerated, or jet-milled obeticholic acid.
- FIG. 4 is a graph showing the dissolution profile of 5 mg tablets containing unmilled or jet-milled obeticholic acid.
- FIG. 5 is a graph showing solubility of obeticholic acid in various buffers at 37 °C over a pH range of about 1.2 to about 12. The dashed and dotted lines represent the
- Biopharmaceutical Classification System (BCS) limit for 5 mg and 10 mg doses, respectively (5 and 10 mg/250 mL)
- FIG. 6 is a graph showing obeticholic acid solubility in various biologically relevant buffers over a pH range of about 1.2 to about 12.
- the dashed and dotted lines represent the Biopharmaceutical Classification System (BCS) high-solubility limit for 5 mg and 10 mg doses, respectively (5 and 10 mg/250 mL).
- BCS Biopharmaceutical Classification System
- FIG. 7A shows the LC/HRMS spectrum in the positive mode of a sample of obeticholic acid OCA and the synthesized ethyl ester of obeticholic acid OCA.
- FIG. 7B shows the mass spectrum in the positive mode of a sample of obeticholic acid OCA and the synthesized ethyl ester of obeticholic acid OCA.
- FIG. 8A shows the total ion count (TIC) chromatogram in the positive ion mode acquired on Q-TOF LC/MS of a sample of obeticholic acid OCA containing the PEG impurity
- FIG. 8B shows the mass spectra in the positive mode acquired on Q-TOF LC/MS of a sample of obeticholic acid OCA containing the PEG impurity
- FIG. 8C shows the total ion count (TIC) chromatogram acquired on triple quad (QQQ) mass spectrometer of a sample of obeticholic acid OCA containing the PEG impurity.
- FIG. 9 shows an enlarged spectrum of the co-eluting peaks containing obeticholic acid OCA and the PEG impurity displaying spacing characteristics of PEG.
- FIG. 11 illustrates ALP Concentration (U/L) over duration of treatment.
- FIG. 12 illustrates TB Concentration ( ⁇ /L) over duration of treatment.
- FIG. 13 illustrates proposed metabolic pathways of OCA in human plasma.
- FIG. 14 illustrates Observed Individual Patient-Level Change in ALP from
- FIG. 15A illustrates mean ALP over time and FIG. 15B illustrates mean total bilirubin (TB) over time.
- FIG. 16 illustrates the mean plasma concentration- time profile (Semi-log) of total OCA following a single oral dose of 10 mg OCA (inset shows expanded view of first 24 hours).
- FIG. 17A illustrates ALP levels and FIG. 17 B illustrates change in ALP from baseline with OCA monotherapy and combination therapy with UDCA, based on pooled data from study 747-201, study 747-202 and Phase 3 study 747-301.
- FIG. 18 illustrates the Goodness of Fit: Observed Concentrations vs Predicted Concentrations of OCA.
- FIG. 18A shows the individual glyco-OCA group
- FIG. 18B shows the individual unconjugated OCA group
- FIG. 18C shows individual tauro-OCA group
- FIG. 18D shows the population glyco-OCA group
- FIG. 18E shows the population unconjugated OCA group
- FIG. 18F shows the population tauro-OCA group.
- FIG. 19 illustrates the Goodness of Fit: Residuals.
- FIG. 19A shows the glyco- OCA group vs. concentration
- FIG. 19B shows the unconjugated OCA group vs.
- FIG. 19C shows the tauro-OCA group vs. concentration
- FIG. 19D shows the glyco-OCA group vs. time
- FIG. 19E shows the unconjugated OCA group vs. time
- FIG. 19E shows the tauro-OCA group vs. time.
- FIG 20 illustrates External Validation of Model in Subjects with Normal Hepatic Function.
- FIG. 20A shows the single dose of 5 mg OCA
- FIG. 20B shows the single dose of 10 mg OCA
- FIG. 20C shows the single dose of 25 mg OCA
- FIG. 20D shows the multiple dose of 5 mg OCA
- FIG. 20E shows the multiple dose of 10 mg OCA
- FIG. 20F shows the multiple dose of 25 mg OCA.
- FIG 21 illustrates External Validation of Model in Subjects with Normal Hepatic Function.
- FIG. 21 A shows the 6 day profile in Period 1
- FIG. 21B shows the 24 hour profile in Period 1
- FIG. 21 C shows the 6 day profile in Period 2
- FIG. 21D shows the 24 hour profile in Period 2.
- FIG 22 illustrates External Validation of Model in Patients with Impaired Hepatic Function.
- FIG. 22A shows the effect of 10 mg OCA in mild impairment
- FIG. 20B shows the effect of 10 mg OCA in moderate impairment
- FIG. 20C shows the effect of 10 mg OCA in severe impairment
- FIG. 22D shows the effect of 25 mg OCA in mild impairment
- FIG. 20E shows the effect of 25 mg OCA in moderate impairment
- FIG. 20E shows the effect of 25 mg OCA in severe impairment.
- FIG. 23 A and FIG. 23B illustrates plasma OCA Concentrations are a Poor Surrogate for Liver OCA Concentrations.
- FIG. 24 A, FIG 24B, and FIG. 24C illustrate changes in FIG 4, APRI Score, and NFS during the course of treating NASH using the obeticholic acid compositions described herein, respectively.
- P-values were calculated using ANCOVA models, regressing change from baseline at each post-baseline visit on treatment group and baseline value of the outcome.
- FIG. 25 illustrates a Visual Predictive Check of PK Model in Subjects with Normal Hepatic Function
- FIG. 25A shows a 6-day profile
- FIG. 25B shows a 24-hour profile
- FIG. 25 C shows a 6-day profile over period 2
- FIG. 25 D shows a 24-hour profile over period 2.
- FIG. 26 shows Visual Predictive Check of PK model in Patients with Normal and Impaired Hepatic Function where FIG. 26A shows normal function, FIG. 26B shows mild impairment, FIG. 26C shows moderate impairment and FIG. 26D shows severe impairment.
- FIG. 27 shows External Validation of Model in Subjects with Normal Hepatic Function
- FIG. 27A shows a single dose of OCA 5 mg
- FIG. 27B shows a single dose of OCA 10 mg
- FIG. 27C shows a single dose of OCA 25 mg
- FIG. 27D shows a multiple dose of OCA 5 mg
- FIG. 27E shows a multiple dose of OCA 10 mg
- FIG. 27F shows a multiple dose of OCA 25 mg.
- FIG 28 shows External Validation of Model in Patients with Impaired Hepatic Function where FIG. 28 A shows mild impairment of OCA 10 mg, FIG. 28B shows moderate impairment of OCA 10 mg, FIG. 28C shows severe impairment of OCA 10 mg, FIG. 28D shows mild impairment of OCA 25 mg, FIG. 28E shows moderate impairment of OCA 25 mg, and FIG. 28F shows severe impairment of OCA 25 mg.
- compositions containing a poorly water-soluble drug require some tools for improving the dissolution property of the drug, for example, adding a surfactant or other additive, or amorphizing the drug.
- a surfactant or other additive can chemically destabilize the drug, and methods of amorphizing the drug may require changing the crystal form.
- compositions containing a high concentration of a poorly water-soluble drug are produced, usually, powders are tableted by direct compression or granules are produced by dry or wet granulation methods and tableted.
- compositions and formulations of obeticholic acid also known as INT-747) having the chemical structure:
- a pharmaceutically acceptable salt, ester, or amino acid conjugate such as, e.g. , glycine, taurine or sarcosine conjugate
- a pharmaceutically acceptable salt, ester, or amino acid conjugate such as, e.g. , glycine, taurine or sarcosine conjugate
- viscosity enhancer refers to an agent or a mixture of agents that increases the thickness of a liquid thereby keeping the active ingredient suspended to allow accurate dosing.
- Viscosity enhancers include, but are not limited to, xantham gum, guar gum, acacia, alginic acid, sodium alginate, propylene glycol alginate, povidone, carbomer, salts of carboxymethylcellulose, methylcellulose, ethylcellulose, hydroxyethyl cellulose, hydroxypropyl cellulose, hydroxypropyl methylcellulose, bentonite, polydextrose, carrageenan, sucrose, sorbitol, xylitol, dextrose, fructose, malitol, gelatin, tragacanth, a polyvinyl alcohol, cetearyl alcohol, colloidal silicon dioxide and mixtures thereof.
- the viscosity enhancer can be any viscosity enhancer known in the art.
- flavoring agent refers to an agent or a mixture of agents that adds flavor to a mixture. Flavoring agents include, but are not limited to, artificial strawberry flavor, art banana flavor and artificial cream flavor. In one embodiment, the flavoring agent can be any flavoring agent known in the art.
- preservative refers to an agent or mixture of agents that is used to protect a composition against antimicrobial (e.g. , yeast, mold, bacteria) activity.
- Preservatives include, but are not limited to, sodium benzoate, benzoic acid, ethylenediaminetetraacetic acid, sorbic acid, benzethonium chloride, benzalkonium chloride, bronopol, butyl paraben, methyl paraben, ethylparaben, propyl paraben, thiomerosol, sodium propionate, chlorhexidine, chlorobutanol, chlorocresol, cresol, imidurea, phenol,
- the preservative can be any preservative known in the art.
- organ refers to a differentiated structure (as in a heart, lung, kidney, liver, etc.) consisting of cells and tissues and performing some specific function in an organism. This term also encompasses bodily parts performing a function or cooperating in an activity (e.g., an eye and related structures that make up the visual organs). The term “organ” further encompasses any partial structure of differentiated cells and tissues that is potentially capable of developing into a complete structure (e.g., a lobe or a section of a liver).
- OCA obeticholic acid
- obeticholic acid examples include: 3 ⁇ ,7 ⁇ -dihydroxy-6 ⁇ -ethyl-5 ⁇ - cholan-24-oic acid, 6 ⁇ -ethyl-chenodeoxycholic acid, 6-ethyl-CDCA, 6ECDCA, cholan-24- oic acid,6-ethyl-3,7-dihydroxy-,(3 ⁇ ,5 , 6 ⁇ ,7 ⁇ )- and INT-747.
- the CAS registry number for obeticholic acid is 459789-99-2. This term refers to all forms of obeticholic acid, e.g. , non- crystalline, crystalline and substantially pure.
- obeticholic acid composition refers to obeticholic acid administered to a patient in any form described herein including as a component of a pharmaceutical composition.
- the term "purity" refers to a chemical analysis of a compound obtained from, e.g., HPLC.
- the purity of a compound is compared to the purity of the reference standard, e.g. , obeticholic acid, via the area under their respective peak for comparisons.
- purity accounts for the organic impurities in a sample.
- Treating includes any effect, e.g. , lessening, reducing, modulating, or eliminating, that results in the improvement of the condition, disease, disorder, etc.
- Treating" or “treatment” of a disease state includes: inhibiting the disease state, i.e., arresting the development of the disease state or its clinical symptoms; or relieving the disease state, i.e. , causing temporary or permanent regression of the disease state or its clinical symptoms.
- a regimen can include periods of active administration and periods of rest as known in the art. Active administration periods include administration of the obeticholic acid compositions described herein in a defined course of time, including, for example, the number of and timing of dosages of the compositions. In some regimens, one or more rest periods can be included where no compound is actively administered, and in certain instances, includes time periods where the efficacy of such compounds can be minimal.
- the term “enhance” refers to an increase or improvement in the function or activity of a protein or cell after administration or contacting with a combination described herein compared to the protein or cell prior to such administration or contact.
- Preventing the disease state includes causing the clinical symptoms of the disease state not to develop in a subject that may be exposed to or predisposed to the disease state, but does not yet experience or display symptoms of the disease state.
- inhibitors refers to any detectable positive effect on the development or progression of a disease or condition. Such a positive effect may include the delay or prevention of the onset of at least one symptom or sign of the disease or condition, alleviation or reversal of the symptom(s) or sign(s), and slowing or prevention of the further worsening of the symptom(s) or sign(s).
- Disease state means any disease, disorder, condition, symptom, or indication.
- the term "effective amount” as used herein refers to an amount of obeticholic acid (e.g., an FXR-activating ligand) that produces an acute or chronic therapeutic effect upon appropriate dose administration.
- the effect includes the prevention, correction, inhibition, or reversal of the symptoms, signs and underlying pathology of a disease/condition (e.g. , fibrosis of the liver, kidney, or intestine) and related complications to any detectable extent.
- a therapeutically effective amount means the amount of obeticholic acid that, when administered to a mammal for treating a disease, is sufficient to effect such treatment for the disease.
- the "therapeutically effective amount” will vary depending on obeticholic acid, the disease and its severity and the age, weight, etc., of the mammal to be treated.
- a therapeutically effective amount can refer to a starting dose or adjusted dose as set forth herein.
- a therapeutically effective amount of obeticholic acid can be formulated with a pharmaceutically acceptable carrier for administration to a human or an animal. Accordingly, obeticholic acid or its formulations can be administered, for example, via oral, parenteral, or topical routes, to provide an effective amount of the compound.
- obeticholic acid prepared in accordance with the present disclosure can be used to coat or impregnate a medical device, e.g. , a stent.
- the therapeutically effective amount can be estimated initially either in cell culture assays or in animal models, usually rats, mice, rabbits, dogs, or pigs.
- the animal model may also be used to determine the appropriate concentration range and route of administration. Such information can then be used to determine useful doses and routes for administration in humans.
- Therapeutic/prophylactic efficacy and toxicity may be determined by standard pharmaceutical procedures in cell cultures or experimental animals, e.g., ED50 (the dose therapeutically effective in 50% of the population) and LD50 (the dose lethal to 50% of the population).
- the dose ratio between toxic and therapeutic effects is the therapeutic index, and it can be expressed as the ratio, LD50/ED50.
- Pharmaceutical compositions that exhibit large therapeutic indices are preferred. The dosage may vary within this range depending upon the dosage form employed, sensitivity of the patient, and the route of administration.
- Dosage and administration are adjusted to provide sufficient levels of the active agent(s) or to maintain the desired effect.
- Factors which may be taken into account include the severity of the disease state, general health of the subject, age, weight, and gender of the subject, diet, time and frequency of administration, drug combination(s), reaction
- a "starting dose” as used herein refers to an initial dose provided to a patient to provide a clinical effect while minimizing onset or occurrence of an adverse effect.
- a starting dose can, in certain instances, be less than an amount typically administered to a patient.
- a starting dose is provided in an amount that is titrated or gradually increased over the course of a titration period or during the course of treatment with an obeticholic acid composition described herein.
- a "titration period” refers to a length of time for which a starting dose is administered to a patient. A titration period continues for a specified length of time, where the patient is often monitored for liver function and/or liver biochemistry as described herein. In one embodiment a titration period concludes when a patient tolerates an obeticholic acid composition described herein but has a decreased or minimal reduction in alkaline phosphatase.
- An “adjusted dose” as used herein refers to a dose of an obeticholic acid composition described herein administered after the termination of a titration period.
- An adjusted dose is often increased compared to a starting dose but, as provided herein, patient tolerance and other factors described herein determine the dosage amount of an adjusted dose.
- a "re-adjusted dose” as used herein refers to any changed dosage amount or dose frequency of an adjusted dose in a patient.
- Hepatic impairment is used in accordance with its standard meaning(s) in the art and can, in certain embodiments herein refer to scoring based upon the Child-Pugh Score of A, B, and C.
- administering refers to the act of delivering an obeticholic acid composition described herein into a subject by such routes as oral, mucosal, topical, suppository, intravenous, parenteral, intraperitoneal, intramuscular, intralesional, intrathecal, intranasal or subcutaneous administration.
- Parenteral administration includes intravenous, intramuscular, intra-arterial, intradermal, subcutaneous, intraperitoneal, intraventricular, and intracranial administration.
- the term can also refer to the frequency (e.g. , daily, weekly, monthly, etc.) of providing an obeticholic acid composition described herein to a patient.
- Administration generally occurs after the onset of the disease, disorder, or condition, or its symptoms but, in certain instances, can occur before the onset of the disease, disorder, or condition, or its symptoms (e.g., administration for patients prone to such a disease, disorder, or condition).
- administration as used herein refers to oral administration.
- co-administration refers to administration of two or more agents (e.g., an obeticholic acid composition described herein and another active agent such as UDCA or an anti-cancer agent described herein).
- the timing of co-administration depends in part of the combination and the compositions administered and can include administration at the same time, prior to, or after the administration of one or more additional therapies.
- An obeticholic acid composition of the instant invention can be administered alone or can be coadministered to the patient.
- Co-administration is meant to include simultaneous or sequential
- an obeticholic acid composition individually or in combination (more than one compound or agent).
- the preparations can also be combined, when desired, with other active substances (e.g., to reduce metabolic degradation).
- the obeticholic acid compositions described herein can be used in combination with each other (i.e., two different obeticholic acid compositions), with other active agents known to be useful in treating a disease, or with adjunctive agents that are not effective alone, but can contribute to or enhance the efficacy of the active agent.
- anti-cancer agent is used in accordance with its plain ordinary meaning and refers to a composition having anti-neoplastic properties or the ability to inhibit the growth or proliferation of cells.
- an anti-cancer agent is a
- an anti-cancer agent is an agent identified herein having utility in methods of treating cancer.
- an anti-cancer agent is an agent approved by the FDA or similar regulatory agency of a country other than the USA, for treating cancer.
- pharmacological effect means that primary indications of the subject being treated are prevented, alleviated, or reduced.
- a pharmacological effect would be one that results in the prevention, alleviation or reduction of primary indications in a treated subject.
- a pharmacological effect means that disorders or symptoms of the primary indications of the subject being treated are prevented, alleviated, or reduced.
- a pharmacological effect would be one that results in the prevention or reduction of primary indications in a treated subject.
- Gaometric Isomers means the diastereomers that owe their existence to hindered rotation about double bonds. These configurations are differentiated in their names by the prefixes cis and trans, or Z and E, which indicate that the groups are on the same or opposite side of the double bond in the molecule according to the Cahn-Ingold-Prelog rules.
- Solidvates means solvent addition forms that contain either stoichiometric or non- stoichiometric amounts of solvent.
- Obeticholic acid may have a tendency to trap a fixed molar ratio of solvent molecules in the crystalline solid state, thus forming a solvate. If the solvent is water the solvate formed is a hydrate, when the solvent is alcohol, the solvate formed is an alcoholate. Hydrates are formed by the combination of one or more molecules of water with one of the substances in which the water retains its molecular state as H2O, such combination being able to form one or more hydrate.
- the compounds of the present disclosure can exist in either hydrated or unhydrated (the anhydrous) form or as solvates with other solvent molecules.
- Non-limiting examples of hydrates include monohydrates, dihydrates, etc.
- Non-limiting examples of solvates include ethanol solvates, acetone solvates, etc.
- obeticholic acid may be depicted as different tautomers.
- all tautomeric forms are intended to be within the scope of the disclosure, and the naming of obeticholic acid does not exclude any tautomer form, obeticholic acid and synthetic intermediates of the disclosure can exist in several tautomeric forms, including the keto-enol.
- keto-enol tautomerism a simultaneous shift of electrons and a hydrogen atom occurs.
- Tautomers exist as mixtures of a tautomeric set in solution. In solid form, usually one tautomer predominates. Even though one tautomer may be described, the present disclosure includes all tautomers of the present compounds.
- Alkenes can include either the E- or Z-geometry, where appropriate.
- Obeticholic acid and synthetic intermediates may exist in stereoisomeric form, and therefore can be produced as individual stereoisomers or as mixtures.
- a "pharmaceutical composition” is a formulation containing obeticholic acid in a form suitable for administration to a subject.
- the pharmaceutical composition is in bulk or in unit dosage form. It is can be advantageous to formulate compositions in dosage unit form for ease of administration and uniformity of dosage.
- Dosage unit form refers to physically discrete units suited as unitary dosages for the subject to be treated; each unit containing a predetermined quantity of active reagent calculated to produce the desired therapeutic effect in association with the required pharmaceutical carrier.
- the specification for the dosage unit forms of the disclosure are dictated by and directly dependent on the unique characteristics of the active reagent and the particular therapeutic effect to be achieved, and the limitations inherent in the art of compounding such an active agent for the treatment of individuals.
- unit dosage form refers to physically discrete units suitable as unitary dosages for human subjects and other mammals, each unit containing a predetermined quantity of active material calculated to produce the desired therapeutic effect, in association with a suitable pharmaceutical excipient as described above.
- the unit dosage form is any of a variety of forms, including, for example, a capsule, an IV bag, a tablet, a single pump on an aerosol inhaler, or a vial.
- the quantity obeticholic acid (e.g. , a formulation of obeticholic acid, or a pharmaceutically acceptable salt, solvate, or amino acid conjugate thereof) in a unit dose of composition is an effective amount and is varied according to the particular treatment involved.
- obeticholic acid e.g. , a formulation of obeticholic acid, or a pharmaceutically acceptable salt, solvate, or amino acid conjugate thereof
- the dosage will also depend on the route of administration.
- routes including oral, pulmonary, rectal, parenteral, transdermal, subcutaneous, intravenous, intramuscular, intraperitoneal, inhalational, buccal, sublingual, intrapleural, intrathecal, intranasal, and the like.
- Dosage forms for the topical or transdermal administration of a compound of this disclosure include powders, sprays, ointments, pastes, creams, lotions, gels, solutions, patches and inhalants.
- obeticholic acid is mixed under sterile conditions with a pharmaceutically acceptable carrier, and with any preservatives, buffers, or propellants that are required.
- flash dose refers to obeticholic acid formulations that are rapidly dispersing dosage forms.
- immediate release is defined as a release of obeticholic acid from a dosage form in a relatively brief period of time, generally up to about 60 minutes.
- modified release is defined to include delayed release, extended release, and pulsed release.
- pulsed release is defined as a series of releases of drug from a dosage form.
- a "subject" or “patient” includes mammals, e.g. , humans, companion animals (e.g. , dogs, cats, birds, and the like), farm animals (e.g., cows, sheep, pigs, horses, fowl, and the like) and laboratory animals (e.g. , rats, mice, guinea pigs, birds, and the like).
- the patient is human.
- the subject is human child (e.g. , between about 30 kg to about 70 kg).
- the human child has had a Kasai procedure, where the Kasai procedure effectively gives them a functional bile duct when they are born either without a bile duct or a bile duct that is completely blocked at birth.
- the phrase "pharmaceutically acceptable” refers to those compounds, materials, compositions, carriers, and/or dosage forms which are, within the scope of sound medical judgment, suitable for use in contact with the tissues of human beings and animals without excessive toxicity, irritation, allergic response, or other problem or complication, commensurate with a reasonable benefit/risk ratio.
- “Pharmaceutically acceptable excipient” means an excipient that is useful in preparing a pharmaceutical composition that is generally safe, non-toxic and neither biologically nor otherwise undesirable, and includes excipient that is acceptable for veterinary use as well as human pharmaceutical use.
- a “pharmaceutically acceptable excipient” as used in the specification and claims includes both one and more than one such excipient.
- a pharmaceutical composition of the disclosure is formulated to be compatible with its intended route of administration.
- routes of administration include parenteral, e.g., intravenous, intradermal, subcutaneous, oral (e.g., inhalation), transdermal (topical), and transmucosal administration.
- Solutions or suspensions used for parenteral, intradermal, or subcutaneous application can include the following components: a sterile diluent such as water for injection, saline solution, fixed oils, polyethylene glycols, glycerine, propylene glycol or other synthetic solvents; antibacterial agents such as benzyl alcohol or methyl parabens; antioxidants such as ascorbic acid or sodium bisulfite; chelating agents such as ethylenediaminetetraacetic acid (EDTA); buffers such as acetates, citrates or phosphates, and agents for the adjustment of tonicity such as sodium chloride or dextrose.
- the pH can be adjusted with acids or bases, such as hydrochloric acid or sodium hydroxide.
- the parenteral preparation can be enclosed in ampoules, disposable syringes or multiple dose vials made of glass or plastic.
- Process of the disclosure refers to a method for preparing obeticholic acid as described herein, wherein the method comprises preparing a crystalline form of obeticholic acid.
- a "control” as used herein refers to a baseline level determined on a patient-by- patient basis, an amount or level considered by those skilled in the art as a normal value, or any level or measure of a condition or biomarker described herein taken from a patient or population of patients at any given time for a given condition.
- Fibrosis refers to a condition involving the development of excessive fibrous connective tissue, e.g. , scar tissue, in a tissue or organ. Such generation of scar tissue may occur in response to infection, inflammation, or injury of the organ due to a disease, trauma, chemical toxicity, and so on. Fibrosis may develop in a variety of different tissues and organs, including the liver, kidney, intestine, lung, heart, etc.
- a "cholestatic condition” refers to any disease or condition in which bile excretion from the liver is impaired or blocked, which can occur either in the liver or in the bile ducts.
- Intrahepatic cholestasis and extrahepatic cholestasis are the two types of cholestatic conditions.
- Intrahepatic cholestasis (which occurs inside the liver) is most commonly seen in primary biliary cirrhosis, primary sclerosing cholangitis, sepsis
- Extrahepatic cholestasis (which occurs outside the liver) can be caused by bile duct tumors, strictures, cysts, diverticula, stone formation in the common bile duct, pancreatitis, pancreatic tumor or pseudocyst, and compression due to a mass or tumor in a nearby organ.
- Clinical symptoms and signs of a cholestatic condition include: itching (pruritus), fatigue, jaundiced skin or eyes, inability to digest certain foods, nausea, vomiting, pale stools, dark urine, and right upper quadrant abdominal pain.
- a patient with a cholestatic condition can be diagnosed and followed clinically based on a set of standard clinical laboratory tests, including measurement of levels of alkaline phosphatase, ⁇ -glutamyl transpeptidase (GGT), 5' nucleotidase, bilirubin, bile acids, and cholesterol in a patient's blood serum.
- GTT ⁇ -glutamyl transpeptidase
- a patient is diagnosed as having a cholestatic condition if serum levels of all three of the diagnostic markers alkaline phosphatase, GGT, and 5' nucleotidase, are considered abnormally elevated.
- the normal serum level of these markers may vary to some degree from laboratory to laboratory and from procedure to procedure, depending on the testing protocol. Thus, a physician will be able to determine, based on the specific laboratory and test procedure, what an abnormally elevated blood level is for each of the markers.
- a patient suffering from a cholestatic condition generally has greater than about 125 IU/L alkaline phosphatase, greater than about 65 IU/L GGT, and greater than about 17 NIL 5' nucleotidase in the blood. Because of the variability in the level of serum markers, a cholestatic condition may be diagnosed on the basis of abnormal levels of these three markers in addition to at least one of the symptoms mentioned above, such as itching (pruritus).
- the disclosure provides a composition comprising obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, wherein obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is in the form of particles, and wherein at least 50% of the particles have a diameter of less than 200 ⁇ m.
- the composition of the disclosure possesses advantageous properties, including improved dissolution profile and solubility.
- 90% of the particles have a diameter of 400 ⁇ m or less, 300 ⁇ m or less, 200 ⁇ m or less, 100 ⁇ m or less, 90 ⁇ m or less, 80 ⁇ m or less, 70 ⁇ m or less, 60 ⁇ m or less, 50 ⁇ m or less, 25 ⁇ m or less.
- 90% of the particles have a diameter of 300 ⁇ m or less, such as 200 ⁇ m or less, 100 ⁇ m or less, 90 ⁇ m or less, 80 ⁇ m or less, 70 ⁇ m or less, 60 ⁇ m or less, 50 ⁇ m or less, 25 ⁇ m or less.
- 90% of the particles have a diameter of 100 ⁇ m or less, such as 90 ⁇ m or less, 80 ⁇ m or less, 70 ⁇ m or less, more preferably 60 ⁇ m or less, more preferably 50 ⁇ m or less, 25 ⁇ m or less. In a further embodiment, 90% of the particles have a diameter of 90 ⁇ m or less, such as 80 ⁇ m or less, 70 ⁇ m or less, 60 ⁇ m or less, 50 ⁇ m or less, 25 ⁇ m or less. In a further embodiment, 90% of the particles have a diameter of 50 ⁇ m or less, such as 25 ⁇ m or less. In a further embodiment, 90% of the particles have a diameter of 25 ⁇ m or less.
- 50% of the particles have a diameter of 200 ⁇ m or less, such as 150 ⁇ m or less, 100 ⁇ m or less, 80 ⁇ m or less, 60 ⁇ m or less, 40 ⁇ m or less, 20 ⁇ m or less, 15 ⁇ m or less, 10 ⁇ m or less, 5 ⁇ m or less.
- 50% of the particles have a diameter of 100 ⁇ m or less, such as 80 ⁇ m or less, 60 ⁇ m or less, 40 ⁇ m or less, 20 ⁇ m or less, 15 ⁇ m or less, more preferably 10 ⁇ m or less, 5 ⁇ m or less.
- 50% of the particles have a diameter of 20 ⁇ m or less, such as 15 ⁇ m or less, 10 ⁇ m or less, 5 ⁇ m or less. In a further embodiment, 50% of the particles have a diameter of 10 ⁇ m or less, such as 5 ⁇ m or less. In a further embodiment, 50% of the particles have a diameter of 5 ⁇ m or less.
- 10% of the particles have a diameter of 5 ⁇ m or less, such as 4 ⁇ m or less, 3 ⁇ m or less, 2 ⁇ m or less, 1 ⁇ m or less. In a further embodiment, 10% of the particles have a diameter of 3 ⁇ m or less, 2 ⁇ m or less, or 1 ⁇ m or less. In a further embodiment, 10% of the particles have a diameter of 2 ⁇ m or less, such as, e.g.,1 ⁇ m or less. In a further embodiment, 10% of the particles have a diameter of 1 ⁇ m or less.
- 90% of the particles have a diameter of 400 ⁇ m or less, 50% of the particles have a diameter of 200 ⁇ m or less, and 10% of the particles have a diameter of 5 ⁇ m or less. In a further embodiment, 90% of the particles have a diameter of 300 ⁇ m or less, 50% of the particles have a diameter of 150 ⁇ m or less, and 10% of the particles have a diameter of 5 ⁇ m or less. In another embodiment, 90% of the particles have a diameter of 100 ⁇ m or less, 50% of the particles have a diameter of 50 ⁇ m or less, and 10% of the particles have a diameter of 5 ⁇ m or less. In another embodiment, 90% of the particles have a diameter of 100 ⁇ m or less, 50% of the particles have a diameter of 20 ⁇ m or less, and 10% of the particles have a diameter of 5 ⁇ m or less.
- 90% of the particles have a diameter of 100 ⁇ m or less, 50% of the particles have a diameter of 10 ⁇ m or less, and 10% of the particles have a diameter of 5 ⁇ m or less. In yet another embodiment, 90% of the particles have a diameter of 90 ⁇ m or less, 50% of the particles have a diameter of 10 ⁇ m or less, and 10% of the particles have a diameter of 5 ⁇ m or less. In another embodiment, 90% of the particles have a diameter of 50 ⁇ m or less, 50% of the particles have a diameter of 10 ⁇ m or less, and 10% of the particles have a diameter of 5 ⁇ m or less.
- 90% of the particles have a diameter of 50 ⁇ m or less, 50% of the particles have a diameter of 5 ⁇ m or less, and 10% of the particles have a diameter of 1 ⁇ m or less. In a further embodiment, 90% of the particles have a diameter of 25 ⁇ m or less, 50% of the particles have a diameter of 5 ⁇ m or less, and 10% of the particles have a diameter of 1 ⁇ m or less.
- 99% of the particles have a diameter of 200 ⁇ m or less, such as 1 ⁇ m to 100 ⁇ m, and 1 ⁇ m to 80 ⁇ m; 90% of the particles have a diameter of 200 ⁇ m or less, such as 2 ⁇ m to 100 ⁇ m, and 2 ⁇ m to 80 ⁇ m; and 50% of the particles have a diameter of 200 ⁇ m or less, such as 7 ⁇ m to 100 ⁇ m, 8 ⁇ m to 100 ⁇ m, and 9 ⁇ m to 80 ⁇ m.
- the particles have a diameter of 100 ⁇ m or less, and 50% of the particles have a diameter of 90 ⁇ m or less.
- 50% of the particles have a diameter of 100 ⁇ m or less, such as 5 ⁇ m to 100 ⁇ m, and 5 ⁇ m to 50 ⁇ m; 90% of the particles have a diameter of 200 ⁇ m or less, such as 3 ⁇ m to 200 ⁇ m, and 3 ⁇ m to 150 ⁇ m; and 99% of the particles have a diameter of 300 ⁇ m or less, such as 1 ⁇ m to 300 ⁇ m, and 1 ⁇ m to 200 ⁇ m.
- 90% of the particles have a diameter of 150 ⁇ m or less, such as 3 ⁇ m to 150 ⁇ m, and 3 ⁇ m to 100 ⁇ m; and 99% of the particles have a diameter of 200 ⁇ m or less, such as 1 ⁇ m to 200 ⁇ m, and 1 ⁇ m to 150 ⁇ m. In a further embodiment, 99% of the particles have a diameter of 150 ⁇ m or less, preferably 2 ⁇ m to 150 ⁇ m, and more preferably 2 ⁇ m to 100 ⁇ m.
- the“particle size reduction” is carried out for the purpose of crushing solid particles by the application of mechanical force such as impact, shearing, or friction thereto to reduce the particle sizes, thereby facilitating the formation of a homogeneous mixed state and improving the dissolution rate and bioavailability of the drug owing to the increased surface area (which refers to as specific surface area, or“SSA”) of the drug.
- mechanical force such as impact, shearing, or friction thereto to reduce the particle sizes
- Known particle size reduction methods include, but are not limited to: high-speed rotating impact mills (hammer mills and impact mills), which reduce particle size by means of the impact force of a high-speed rotating hammer or pin in a chamber; carrier mills (ball mills or vibration mills) which reduce particle size powder by means of impact force or friction force in a rotating cylinder in which the powder and magnetic balls are placed; and fluid energy mills (jet mills), which reduce particle size by jetting compressed air and raw material particles from a nozzle and colliding the particles accelerated by the jet of air with swirling particles in a chamber.
- high-speed rotating impact mills hammer mills and impact mills
- carrier mills ball mills or vibration mills
- jet mills which reduce particle size by jetting compressed air and raw material particles from a nozzle and colliding the particles accelerated by the jet of air with swirling particles in a chamber.
- the particle size of obeticholic acid is reduced using a jet mill.“Micronization,” as defined herein, is a reduction of particle size of an active ingredient, i.e., obeticholic acid, to a diameter that is less than about 200 ⁇ m, such as less than about 100 ⁇ m, less than about 50 ⁇ m, and less than 25 ⁇ m.
- obeticholic acid has a particle size distribution with a D 50 of not more than 100 ⁇ m.
- the D 50 is not more than 50 ⁇ m, not more than 20 ⁇ m, or not more than 10 ⁇ m.
- the D90 is not more than 200 ⁇ m, or not more than 100 ⁇ m.
- the D 10 is not more than 20 ⁇ m, not more than 10 ⁇ m, or not more than 5 ⁇ m.
- Particle size analysis can be carried out via different methods.
- Non-limiting examples of the methods include, but are not limited to, sieve technique, wet dispersion method with laser diffraction analysis, dry dispersion method with laser diffraction analysis, or a combination thereof.
- Particle size analysis is not limited to the methods described herein and can be carried out using any method known to one skilled in the art.
- particle size analysis can be performed via a sieve technique.
- particle size analysis can be performed using a wet dispersion method (e.g., water as the dispersing agent, and analysis by laser diffraction using, e.g. , Sympatec equipment).
- particle size analysis can be performed using a dry dispersion method and analyzed by laser diffraction using, e.g. , Sympatec equipment.
- particle size distribution (% volume at each particle size) is measured via a Sympatec laser diffraction analyzer (e.g., Helos/KF-Magic F71000 with Rodos Dispersing Unit, Vibri sampling unit with Sniffer rotation, Nilfisk exhaustion, or equivalent).
- particle size distribution (% volume at each particle size) is measured via a Malvern laser diffraction analyzer.
- particles can be measured using the following:
- Particle diameter distribution measurement apparatus HELOS (KF-Magic F71000) & RODOS System (manufactured by Sympatec GmbH);
- Measurement range of laser diffraction apparatus 0.5/0.9 to 175 ⁇ m;
- Dispersive pressure 1.0 bar.
- composition of the present disclosure comprising obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, in the form of particles, offers improved dissolution and solubility.
- OCA obeticholic acid
- in vitro dissolution rates or profiles of the entire active ingredient of the pharmaceutical composition are measured from the entire pharmaceutical composition according to the steps and conditions in Example 3.
- the dissolution rate can be measured in a variety of buffers, which optionally contains one or more surfactants.
- buffers include acetate buffer, phosphate buffers, and alkaline borate buffers, or a combination thereof.
- Non-limiting examples of surfactants include, polysorbate 80 (Tween 80®), potassium laurate, sodium laurate, triethanol ammonium iaurate, potassium myristate, sodium myri state, triethanol ammonium myristate, sodium iauryi sulfate, polyoxyethyiene aikyl ether sodium sulfate, sodium alkyl ⁇ -alanine, sodium suifosuccinate.
- polysorbate 80 Teween 80®
- potassium laurate sodium laurate
- triethanol ammonium iaurate potassium myristate
- sodium myri state sodium myri state
- triethanol ammonium myristate sodium iauryi sulfate
- sodium iauryi sulfate polyoxyethyiene aikyl ether sodium sulfate
- sodium alkyl ⁇ -alanine sodium suifosuccinate.
- acylmethyl taurine sodium alkyl ethane sulfonate, polyoxyethylene aikyl ether sodium carbox late, trimethyl ammonium chloride, benzalkonium chloride, iauryi amine oxide, amide propyl betaine coconut fatly acid, amide propyl betaine laurate, amide propyl betaine myristate, sorbitan nionolaurate, sorbitan monopalmitate, sorbitan sesquioleate,
- the dissolution rate is measured in Disodium Hydrogen Phosphate Buffer (Na2HP04). In another embodiment, the dissolution rate is measured in a buffer containing a surfactant (e.g. , 0.01-0.1 % wt/wt). In one embodiment, the surfactant is polysorbate 80 (Tween 80®).
- in vitro dissolution rates or profiles are measured by using a using USP II paddle apparatus in Disodium Hydrogen Phosphate Buffer (Na2HP04) at a temperature of about 37 ⁇ 0.5°C and paddles rotation between about 50 rpm to about 100 rpm.
- in vitro dissolution rates or profiles are measured by using a using USP II paddle apparatus in Disodium Hydrogen Phosphate Buffer (Na2HP04) containing polysorbate 80 (Tween 80®) (e.g., 0.01-0.1% wt/wt) at a temperature of about 37 ⁇ 0.5°C and paddles rotation between about 50 rpm to about 100 rpm.
- Tween 80® polysorbate 80
- composition includes the entire active ingredient and if the pharmaceutical composition contains a capsule shell, carrier, excipient, diluent, disintegrating agent, lubricant, binder or any additional agent described in the Pharmaceutical Composition Section below, the measurement is performed with those components.
- in vitro dissolution is conducted at about 75 rpm using Disodium Hydrogen Phosphate Buffer (Na2HP04). In another embodiment, in vitro dissolution is conducted at 75 rpm using about 900 mL of a Disodium Hydrogen Phosphate Buffer (Na2HP04). Solutions are collected at 15 minutes, 30 minutes, 45 minutes, 60 minutes, and 75 minutes after the start of the dissolution. The dissolution rate of the compound is measured by high-performance liquid chromatography (HPLC) with Corona Charged Aerosol Detection (CAD).
- HPLC high-performance liquid chromatography
- CAD Corona Charged Aerosol Detection
- the concentration for OCA (e.g. , in a Disodium Hydrogen Phosphate Buffer, optionally containing a surfactant, such as polysorbate 80 (Tween 80®)), after dissolution is between about 0.001 mg/mL to about 0.01 mg/mL, or between about 0.001 mg/mL to about 0.03 mg/mL. Above pH 6.8, the solubility of OCA is well above 0.01 mg/mL.
- the concentration for dissolved 5 mg tablets of OCA is between about 0.001 mg/mL to about 0.02 mg/mL. In another embodiment, the concentration for dissolved 5 mg tablets of OCA is between about 0.003 mg/mL to about 0.01 mg/mL. In yet another embodiment, the concentration for dissolved 5 mg tablets of OCA is between about 0.004 mg/mL to about 0.009 mg/mL. In another embodiment, the concentration for dissolved 5 mg tablets of OCA is between about 0.005 mg/mL to about 0.008 mg/mL. In yet another embodiment, the concentration for dissolved 5 mg tablets of OCA is between about 0.006 mg/mL to about 0.007 mg/mL. In another embodiment, the concentration for dissolved 5 mg tablets of OCA is about 0.006 mg/mL. In yet another embodiment, the concentration for dissolved 5 mg tablets of OCA is about 0.0056 mg/mL.
- the concentration for dissolved 10 mg tablets of OCA is between about 0.001 mg/mL to about 0.03 mg/mL. In another embodiment, the concentration for dissolved 10 mg tablets of OCA is between about 0.005 mg/mL to about 0.025 mg/mL. In yet another embodiment, the concentration for dissolved 10 mg tablets of OCA is between about 0.008 mg/mL to about 0.02 mg/mL. In another embodiment, the concentration for dissolved 10 mg tablets of OCA is between about 0.009 mg/mL to about 0.015 mg/mL. In yet another embodiment, the concentration for dissolved 10 mg tablets of OCA is about 0.011 mg/mL. In another embodiment, the concentration for dissolved 10 mg tablets of OCA is about 0.010 mg/mL.
- the concentration for dissolved 25 mg tablets of OCA is between about 0.001 mg/mL to about 0.05 mg/mL. In another embodiment, the concentration for dissolved 25 mg tablets of OCA is between about 0.01 mg/mL to about 0.08 mg/mL. In yet another embodiment, the concentration for dissolved 25 mg tablets of OCA is between about 0.02 mg/mL to about 0.06 mg/mL. In another embodiment, the concentration for dissolved 25 mg tablets of OCA is between about 0.025 mg/mL to about 0.04 mg/mL. In yet another embodiment, the concentration for dissolved 25 mg tablets of OCA is about 0.026 mg/mL to about 0.03 mg/mL. In another embodiment, the concentration for dissolved 25 mg tablets of OCA is about 0.028 mg/mL.
- composition of the present disclosure comprising obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, in the form of particles, provides improved dissolution of obeticholic acid or a
- obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof in the particle composition of the present disclosure dissolves (e.g. , in a Disodium Hydrogen Phosphate Buffer) at a rate that is at least 2%, 3%, 4%, 5%, 6%, 7%, 8%, 9%, 10%, 15%, 20%, 30%, 40%, 50%, 80%, or 100% faster than the dissolution rate when obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is not present in the particle composition of the present disclosure.
- obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof in the particle composition of the present disclosure is dissolved within about 15 minutes, or about 65% to about 95% is dissolved within about 30 minutes, or about 80% to about 95% is dissolved within about 45 minutes, or about 87% to about 97% is dissolved within about 60 minutes, or about 87% to about 99% is dissolved within about 75 minutes.
- obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof in the particle composition of the present disclosure is dissolved within about 15 minutes, or about 75% to about 91 % is dissolved within about 30 minutes, or about 85% to about 93% is dissolved within about 45 minutes, or about 90% to about 96% is dissolved within about 60 minutes, or about 90% to about 97% is dissolved within about 75 minutes.
- obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof in the particle composition of the present disclosure is dissolved within about 15 minutes, or about 80% to about 90% is dissolved within about 30 minutes, or about 87% to about 94% is dissolved within about 45 minutes, or about 92% to about 96% is dissolved within about 60 minutes, or about 91 % to about 97% is dissolved within about 75 minutes.
- obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof in the particle composition of the present disclosure is dissolved within about 15 minutes, or about 70% to about 90% is dissolved within about 30 minutes, or about 85% to about 92% is dissolved within about 45 minutes, or about 89% to about 96% is dissolved within about 60 minutes, or about 90% to about 96% is dissolved within about 75 minutes.
- at least about 60% obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof in the particle composition of the present disclosure is dissolved within about 15 minutes, or at least about 90% is dissolved within about 60 minutes.
- obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof in the particle composition of the present disclosure has an in vitro dissolution profile of about 51% dissolved within about 15 minutes, or about 66% dissolved within about 30 minutes, or about 79% dissolved within about 45 minutes, or about 85% dissolved within about 60 minutes.
- composition of the present disclosure comprising obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, in the form of particles, provides improved solubility of obeticholic acid or a
- obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof in the particle composition of the present disclosure has a solubility (e.g., in a Disodium Hydrogen Phosphate Buffer) that is at least 2%, 3%, 4%, 5%, 6%, 7%, 8%, 9%, 10%, 15%, 20%, 30%, 40%, 50%, 80%, or 100% higher than the solubility when obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is not present in the particle composition of the present disclosure.
- obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof in the particle composition of the present disclosure has a solubility (e.g., in a Disodium Hydrogen Phosphate Buffer) that is at least 2%, 3%, 4%, 5%, 6%, 7%, 8%, 9%, 10%, 15%, 20%, 30%, 40%, 50%, 80%, or 100% higher than
- composition of the present disclosure has a solubility (e.g. , in a Disodium Hydrogen
- Phosphate Buffer that is at least 2%, 3%, 4%, 5%, 6%, 7%, 8%, 9%, 10%, 15%, or 20% higher than the solubility when obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is not present in the particle composition of the present disclosure at a pH (e.g., pH 6.8) at which obeticholic acid has the highest solubility (e.g. , freely soluble) when not present in the particle composition of the present disclosure.
- a pH e.g., pH 6.8
- solubility e.g. , freely soluble
- obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, and/or particles of obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof has a solubility of about 0.001 to about 0.600 mg/mL.
- obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, and/or particles of obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof has a solubility of about 0.02 to about 0.500 mg/mL.
- obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, and/or particles of obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof has a solubility of about 0.03 to about 0.48 mg/mL.
- obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, and/or particles of obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof has a solubility of about 0.05 to about 0.46 mg/mL.
- obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, and/or particles of obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof has a solubility of about 0.1 to about 0.5 mg/mL.
- obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, and/or particles of obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof has a solubility of about 0.2 to about 0.6 mg/mL.
- the disclosure also comprehends isotopically-labeled obeticholic acid, or pharmaceutically acceptable salts, solvate, or amino acid conjugates thereof, which are identical to those recited in formulae of the disclosure and following, but for the fact that one or more atoms are replaced by an atom having an atomic mass or mass number different from the atomic mass or mass number most commonly found in nature.
- isotopes that can be incorporated into obeticholic acid, or pharmaceutically acceptable salts, solvate, or amino acid conjugates thereof include isotopes of hydrogen, carbon, nitrogen, fluorine, such as 3 H, 11 C, 14 C and 18 F.
- Obeticholic acid, or pharmaceutically acceptable salts, solvates, or amino acid conjugates thereof that contain the aforementioned isotopes and/or other isotopes of other atoms are within the scope of the present disclosure.
- Isotopically-labeled obeticholic acid, or pharmaceutically acceptable salts, solvates, or amino acid conjugates thereof, for example those into which radioactive isotopes such as 3 H, 14 C are incorporated, are useful in drug and/or substrate tissue distribution assays. Tritiated, i.e. , 3 H, and carbon-14, i.e. , 14 C, isotopes are particularly preferred for their ease of preparation and detectability.
- isotopically labeled obeticholic acid or pharmaceutically acceptable salts, solvates, or amino acid conjugates thereof can generally be prepared by carrying out the procedures disclosed in the Schemes and/or in the Examples of the disclosure, by substituting a readily available isotopically labeled reagent for a non-isotopically labeled reagent.
- obeticholic acid, or pharmaceutically acceptable salts, solvates, or amino acid conjugates thereof are not isotopically labeled.
- deuterated obeticholic acid is useful for bioanalytical assays.
- obeticholic acid, or pharmaceutically acceptable salts, solvates, or amino acid conjugates thereof are radiolabeled.
- the disclosure provides a composition comprising obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, and a pharmaceutically acceptable excipient having a low alcohol (e.g. , an impurity having at least one primary OH group, such as ethanol or methanol) content.
- the alcohol is a primary alcohol.
- primary alcohol is an alcohol which has a hydroxy group connected to a primary carbon atom.
- the composition of the disclosure possesses advantageous properties, including improved stability of obeticholic acid in the composition.
- the excipient can be any excipient present in the composition comprising obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof.
- excipients include, but are not limited to, calcium phosphate, microcrystalline cellulose, sodium starch glycolate and magnesium stearate, or a combination thereof.
- the excipient can be any excipient known in the art.
- the excipient is selected from calcium phosphate, microcrystalline cellulose, sodium starch glycolate and magnesium stearate.
- the excipient is selected from microcrystalline cellulose, sodium starch glycolate and magnesium stearate.
- the excipient is the excipient is magnesium stearate.
- the excipient is microcrystalline cellulose.
- the excipient is sodium starch glycolate.
- the excipient has an impurity having a primary alcohol group.
- the impurity in the excipient is ethanol, methanol, polyvinyl alcohol, polyethylene glycol, or a substance having at least one primary OH moiety.
- the total alcohol (e.g. , the impurity having at least one primary OH group) content in the excipient is less than 6%, 5%, 4.5%, 4%, 3.5%, 3%, 2.5%, 2%, 1.5%, 1%, or 0.5% (wt/wt).
- the alcohol is a substance having at least one primary OH moiety.
- the alcohol is ethanol, methanol, polyvinyl alcohol, polyethylene glycol, or a combination thereof.
- the total content of ethanol, methanol, polyvinyl alcohol, polyethylene glycol, or a combination thereof in the excipient is less than 6%, 5%, 4.5%, 4%, 3.5%, 3%, 2.5%, 2%, 1.5%, 1%, or 0.5% (wt/wt).
- the alcohol is ethanol.
- the total ethanol content in the excipient is less than 6%, 5%, 4.5%, 4%, 3.5%, 3%, 2.5%, 2%, 1.5%, 1%, or 0.5% (wt/wt).
- the excipient is sodium starch glycolate.
- the sodium starch glycolate comprises less than 6%, 5%, 4.5%, 4%, 3.5%, 3%, 2.5%, 2%, 1.5%, 1%, or 0.5% (wt/wt) ethanol.
- the alcohol is methanol.
- the total methanol content in the excipient is less than 6%, 5%, 4.5%, 4%, 3.5%, 3%, 2.5%, 2%, 1.5%, 1%, or 0.5% (wt/wt).
- the alcohol is a substance having at least one primary OH moiety.
- the total content of the substance having at least one primary OH moiety in the excipient is less than 6%, 5%, 4.5%, 4%, 3.5%, 3%, 2.5%, 2%, 1.5%, 1 %, or 0.5% (wt/wt).
- the alcohol is polyvinyl alcohol.
- the total polyvinyl alcohol content in the excipient is less than 6%, 5%, 4.5%, 4%, 3.5%, 3%, 2.5%, 2%, 1.5%, 1%, or 0.5% (wt/wt).
- the excipient is sodium starch glycolate.
- the sodium starch glycolate comprises less than 6%, 5%, 4.5%, 4%, 3.5%, 3%, 2.5%, 2%, 1.5%, 1%, or 0.5% (wt/wt) polyvinyl alcohol.
- the alcohol is polyethylene glycol.
- the total polyethylene glycol content in the excipient is less than 6%, 5%, 4.5%, 4%, 3.5%, 3%, 2.5%, 2%, 1.5%, 1%, or 0.5% (wt/wt).
- the excipient is sodium starch glycolate.
- the sodium starch glycolate comprises less than 6%, 5%, 4.5%, 4%, 3.5%, 3%, 2.5%, 2%, 1.5%, 1%, or 0.5% (wt/wt) polyethylene glycol.
- composition comprising obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, and a pharmaceutically acceptable excipient having low alcohol content offers advantageous stability of obeticholic acid upon storage under various conditions.
- composition comprising obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, and a
- pharmaceutically acceptable excipient having a low primary alcohol content comprises a decreased amount of impurities, as compared to an obeticholic acid composition comprising an excipient having a high alcohol (e.g. , greater than or equal to 6% (wt/wt) content).
- the impurity is an ester of obeticholic acid. In one embodiment, the amount of the ester of obeticholic acid is decreased by at least 10%, 20%, 30%, 40%, 50%, 60%, 70%, 80%, 90%, 95%, or 99%. In one embodiment, the amount of the ester of obeticholic acid is decreased by at least 50%, 60%, 70%, 80%, 90%, 95%, or 99%.
- the impurity is an ethyl ester of obeticholic acid.
- the amount of the ethyl ester of obeticholic acid is decreased by at least 10%, 20%, 30%, 40%, 50%, 60%, 70%, 80%, 90%, 95%, or 99%. In one embodiment, the amount of the ethyl ester of obeticholic acid is decreased by at least 50%, 60%, 70%, 80%, 90%, 95%, or 99%. In another embodiment, the amount of the ethyl ester of obeticholic acid is less than 0.5%, 0.4%, 0.3%, 0.2%, 0.1%, 0.09%, 0.08%, 0.07%, 0.06%, 0.05%, 0.04%, 0.03%, 0.02%, or 0.01% (wt wt).
- the amount of the ethyl ester of obeticholic acid is less than 0.5%, 0.4%, 0.3%, 0.2%, 0.1 %, 0.09%, 0.08%, 0.07%, 0.06%, 0.05%, 0.04%, 0.03%, 0.02%, or 0.01% (wt/wt) at the storage condition of 40°C, 75% RH for 4 weeks.
- the amount of the ethyl ester of obeticholic acid is less than 0.2%, 0.1 %, 0.09%, 0.08%, 0.07%, 0.06%, 0.05%, 0.04%, 0.03%, 0.02%, or 0.01% (wt/wt) at the storage condition of 40°C, 75% RH for 4 weeks.
- the impurity is a methyl ester of obeticholic acid.
- the amount of the methyl ester of obeticholic acid is decreased by at least 10%, 20%, 30%, 40%, 50%, 60%, 70%, 80%, 90%, 95%, or 99%.
- the amount of the methyl ester of obeticholic acid is decreased by at least 50%, 60%, 70%, 80%, 90%, 95%, or 99%.
- the amount of the methyl ester of obeticholic acid is less than 0.5%, 0.4%, 0.3%, 0.2%, 0.1%, 0.09%, 0.08%, 0.07%, 0.06%, 0.05%, 0.04%, 0.03%, 0.02%, or 0.01% (wt/wt).
- An analysis of the impurities in an obeticholic acid composition can be conducted with methods known to one skilled in the art, for example, with LC/HRMS using LTQ-Orbitrap.
- the identities of various impurities can be confirmed through various techniques available in the art. For example, to determine whether an ethyl ester of obeticholic acid is an impurity, obeticholic acid can be dissolved in ethanol, and treated with concentrated acid and heated to synthesize the ethyl ester. The retention time and mass spectrometry of the impurity can be compared with those of the synthesized ethyl ester of obeticholic acid. The excipients were analyzed for ethanol content and excipients containing higher ethanol content were substituted with a low ethanol content excipient.
- composition comprising obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, in the form of particles, or the composition comprising obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, and a pharmaceutically acceptable excipient having a low alcohol content, as disclosed herein, can be incorporated into a pharmaceutical composition suitable for administration (e.g. , oral administration).
- the present disclosure provides a pharmaceutical composition, comprising a therapeutically effective amount of obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, and a
- the pharmaceutical composition has a low alcohol content as described herein.
- the pharmaceutical composition comprises sodium starch glycolate comprising less than 5% alcohol (e.g., ethanol).
- the pharmaceutical composition comprises a
- obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, and a pharmaceutically acceptable excipient having a low alcohol content, wherein obeticholic acid is in the form of particles.
- the particles have a size distribution as described herein..
- the pharmaceutical composition further comprises one or more pharmaceutical excipients.
- the excipient can be one or more selected from the group consisting of diluents, sweeteners, viscosity enhancing agents, dispersing agents, preservatives, flavoring agents and the like.
- One excipient can perform more than one function.
- the one or more pharmaceutical excipients include a lubricant and/or a diluent.
- Non-limiting examples of sweeteners include natural sweeteners such as sugars, e.g. , fructose, glucose, sucrose, sugar alcohols such as mannitol, sorbitol or mixtures thereof and artificial sweeteners such as sodium saccharine, sodium cyclamate and aspartame.
- the sweetener can be any sweetener known in the art.
- the sweetener is selected from fructose, glucose, sucrose, mannitol, and sorbitol, or a combination thereof .
- Dispersing agents include, but are not limited to, colloidal silicon dioxide and surfactants, wherein the surfactant is used alone or as an admixture with one or more surfactant.
- the dispersing agent can be any dispersing agent known in the art. Combinations of colloidal silicon dioxide with one or more surfactants can also be used.
- the lubricant can be any lubricant known in the art.
- Non- limiting examples of lubricants include magnesium stearate, calcium stearate, stearic acid, glyceryl behenate, hydrogenated vegetable oil, and glycerine fumarate, and/or a combination thereof.
- the lubricant is selected from magnesium stearate, calcium stearate, stearic acid, glyceryl behenate, hydrogenated vegetable oil, and glycerine fumarate.
- the lubricant is calcium stearate.
- the lubricant is stearic acid.
- the lubricant is magnesium stearate.
- the diluent can be any diluent known in the art.
- Non-limiting examples of diluents include starch, pregelatinized starch, microcrystalline cellulose, calcium carbonate, dibasic calcium phosphate, tribasic calcium phosphate, calcium phosphate, lactose, dextrose, fructose, lactitol, lactose, magnesium carbonate, magnesium oxide, maltitol, maltodextrin, maltose, simethicone, sodium chloride, talc, xylitol, sorbitol, mannitol, and sucrose, and/or a combination thereof.
- the diluent is selected from starch, pregelatinized starch, microcrystalline cellulose, calcium phosphate, lactose, sorbitol, mannitol, and sucrose.
- the diluent is calcium phosphate.
- the diluent is mannitol.
- the diluent is microcrystalline cellulose.
- the pharmaceutical composition may further comprise a coating agent such as sugar-based coating agents, water-soluble film coating agents, enteric coating agents and delayed release coating agents or a coating composition comprising any combination thereof.
- a coating agent such as sugar-based coating agents, water-soluble film coating agents, enteric coating agents and delayed release coating agents or a coating composition comprising any combination thereof.
- the coating agent can be any coating agent known in the art. Examples of coating agents include, but are not limited to, saccharose used alone or together with any of the agents such as talc, calcium carbonate, calcium phosphate, calcium sulphate, gelatine, gum arabic, polyvinylpyrrolidone and pullulan or any
- cellulose derivatives such as hydroxypropyl cellulose, hydroxypropyl methyl cellulose, hydroxyethyl cellulose, methyl hydroxyethyl cellulose and sodium carboxymethyl cellulose; synthetic polymers such as polyvinyl acetal diethyl amino acetate, aminoalkyl methacrylate copolymers and polyvinylpyrrolidone; polysaccharides such as pullulan; hydroxypropyl methyl cellulose phthalate; hydroxypropyl methyl cellulose acetate succinate; carboxymethyl ethyl cellulose; cellulose acetate phthalate; acrylic acid derivatives such as methacrylic acid copolymer L, methacrylic acid copolymer LD and methacrylic acid copolymer S; natural substances such as shellac; titanium dioxide; polyvinyl alcohol (e.g.
- the coating agent is selected from hydroxypropyl cellulose, hydroxypropyl methyl cellulose, hydroxyethyl cellulose, methyl hydroxyethyl cellulose, sodium carboxymethyl cellulose, polyvinyl acetal diethyl amino acetate, polyvinyl alcohol, polyethylene glycol, and lecithin, or a combination thereof.
- the coating agent is Opadry® II (e.g. , Opadry® II green, white, yellow, etc.).
- the pharmaceutical composition comprising obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, in the form of particles, at about 1 % to about 6% by weight, sodium starch glycolate at about 2% to about 8 % by weight having a low alcohol content, a lubricant (e.g. , magnesium stearate) at about 0.1% to about 2.0% by weight, and a diluent (e.g. , microcrystalline cellulose) at about 85% to about 95% by weight.
- the sodium starch glycolate comprises less than 6% (wt/wt) ethanol.
- the pharmaceutically composition is in solid particle form.
- Any inert excipient that is commonly used as a carrier or diluent may be used in the pharmaceutical composition of the present disclosure, such as for example, a gum, a starch, a sugar, a cellulosic material, a glycolate, an acrylate, or mixtures thereof.
- the filler/diluent is microcrystalline cellulose.
- the pharmaceutical composition may further comprise a disintegrating agent (e.g. , sodium starch glycolate) and/or a lubricant (e.g., magnesium stearate).
- the pharmaceutical composition may comprise one or more additives selected from a buffer, a surfactant, a solubilizing agent, a plasticizer, an emulsifier, a stabilizing agent, a viscosity increasing agent, a sweetener, a film forming agent, or any combination thereof.
- the pharmaceutical composition of the present disclosure may be in the form of controlled release of immediate release formulations.
- the percentage of the active ingredient i.e., obeticholic acid, or a
- the composition may comprise between about 0.1 and about 99%, between about 1- 50%, between about 1-25%, or about 1-6% by weight of active ingredient.
- the composition may comprise between about 20-99%, between about 45-97%, between about 65-96%, or between about 85-95% by weight microcrystalline cellulose as a filler or diluent.
- the composition may comprise between about 1-30%, between about 1 -20%, or between about 2-8% by weight sodium starch glycolate as a disintegrant.
- the composition may comprise between about 0.1 -5% or about 0.5-2.0% by weight magnesium stearate as a lubricant.
- the pharmaceutical composition of the present disclosure is about 0.1 % to about 10% by weight of active ingredient (i. e. , obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof), about 0.1% to about 20 % by weight of sodium starch glycolate, about 0.01% to about 8.0% by weight of magnesium stearate, and about 65% to about 99% by weight of microcrystalline cellulose.
- the pharmaceutical composition of the present disclosure is about 0.5% to about 8% by weight of active ingredient, about 1% to about 10 % by weight of sodium starch glycolate, about 0.05% to about 4.0% by weight of magnesium stearate, and about 75% to about 97 % by weight of microcrystalline cellulose.
- the pharmaceutical composition of the present disclosure is about 1 % to about 6% by weight of active ingredient, about 2% to about 8 % by weight of sodium starch glycolate, about 0.1% to about 2.0% by weight of magnesium stearate, and about 85% to about 95% by weight of microcrystalline cellulose.
- obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, in the pharmaceutical composition is in the form of particles, as described herein.
- the present disclosure provides a pharmaceutical composition, comprising a therapeutically effective amount of obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, in the form of particles, and a pharmaceutically acceptable excipient having a low alcohol content.
- the obeticholic acid particle composition is an obeticholic acid particle composition described herein.
- the pharmaceutical composition has a low alcohol content as described herein.
- the pharmaceutical composition comprises sodium starch glycolate comprising less than 6% alcohol (e.g. , ethanol).
- the present disclosure provides a method for preparing a pharmaceutical composition containing a therapeutically effective amount of obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, in the form of particles, comprising i) micronizing obeticholic acid acceptable salt, ester, or amino acid conjugate thereof until at least 90% of the particles have a diameter of less than 100 ⁇ , such as less than 90 ⁇ , less than 50 ⁇ , less than 25 ⁇ , less than 20 ⁇ , less than 15 ⁇ , less than 10 ⁇ , less than 5 ⁇ , or less than 1 ⁇ , and ii) combining the micronized obeticholic acid particles with at least one pharmaceutically acceptable excipient.
- the micronizing is carried out using a jet-mill.
- the present disclosure provides a method for preparing a pharmaceutical composition containing a therapeutically effective amount of obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, in the form of particles, comprising i) micronizing obeticholic acid acceptable salt, ester, or amino acid conjugate thereof until at least 50% of the particles have a diameter of less than 10 ⁇ m, i.e., less than 5 ⁇ m, and ii) combining the micronized obeticholic acid particles with at least one pharmaceutically acceptable excipient.
- the micronizing is carried out using a jet-mill.
- the present disclosure provides a method for preparing a pharmaceutical composition containing a therapeutically effective amount of obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, in the form of particles, comprising i) micronizing obeticholic acid acceptable salt, ester, or amino acid conjugate thereof until at least 10% of the particles have a diameter of less than 5 ⁇ m, i.e., less than 1 ⁇ m, and ii) combining the micronized obeticholic acid particles with at least one pharmaceutically acceptable excipient.
- the micronizing is carried out using a jet-mill.
- the present disclosure provides a method for preparing a pharmaceutical composition containing a therapeutically effective amount of obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, in the form of particles, comprising i) micronizing obeticholic acid acceptable salt, ester, or amino acid conjugate thereof until at least 90% of the particles have a diameter of less than 100 ⁇ m, preferably less than 90 ⁇ m, less than 50 ⁇ m, less than 25 ⁇ m, less than 20 ⁇ m, less than 15 ⁇ ,, less than 10 ⁇ m, less than 5 ⁇ m, less than 1 ⁇ m; at least 50% of the particles have a diameter of less than 10 ⁇ m, less than 5 ⁇ m, less than 1 ⁇ m; and at least 10% of the particles have a diameter of less than 5 ⁇ m, or less than 1 ⁇ m, and ii) combining the micronized obeticholic acid particles with at least one pharmaceutically acceptable excipient.
- the present disclosure provides a method for preparing a pharmaceutical composition containing a therapeutically effective amount of obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, in the form of particles, comprising i) micronizing obeticholic acid acceptable salt, ester, or amino acid conjugate thereof until at least 90% of the particles have a diameter of less than 100 ⁇ m, at least 50% of the particles have a diameter of less than 10 ⁇ , and at least 10% of the particles have a diameter of less than 5 ⁇ m, and ii) combining the micronized obeticholic acid particles with at least one pharmaceutically acceptable excipient.
- the micronizing is carried out using a jet-mill.
- the present disclosure provides a method for preparing a pharmaceutical composition containing a therapeutically effective amount of obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, in the form of particles, comprising i) micronizing obeticholic acid acceptable salt, ester, or amino acid conjugate thereof until at least 90% of the particles have a diameter of less than 25 ⁇ , at least 50% of the particles have a diameter of less than 5 ⁇ m, and at least 10% of the particles have a diameter of less than 1 ⁇ m, and ii) combining the micronized obeticholic acid particles with at least one pharmaceutically acceptable excipient.
- the micronizing is carried out using a jet-mill.
- the present disclosure provides a method for treating or preventing a disease or condition, comprising administering an effective amount of an obeticholic acid composition of the present disclosure to a patient in need thereof.
- the present disclosure provides a method for treating a disease or condition by administering an effective amount of an obeticholic acid composition described herein to a patient in need thereof.
- the effective amount refers to a titrated dosage administered during a titration period as set forth herein.
- the effective amount refers to an adjusted or re-adjusted dosage administered after a titration period as set forth herein.
- the methods described herein refer generally to the obeticholic acid compositions set forth herein.
- the methods described herein can include any specific formulation provided herein, for example, that provided in Example 11.
- the obeticholic acid composition useful in the methods of treating described herein is a composition provided in Example 11.
- the obeticholic acid composition useful in the methods of treating described herein is a composition that includes microcrystalline cellulose, sodium starch glycolate, and magnesium stearate as excipients.
- Such a composition can be provided in a dosage form set forth herein, e.g., an oral dosage form such as a tablet or coated tablet.
- the obeticholic acid composition useful in the methods is a tablet or coated tablet for oral administration.
- the oral dosage form of the obeticholic acid composition includes a film coating that includes one or more excipients selected from polyvinyl alcohol (part hydrolyzed), titanium dioxide, macrogol (polyethylene glycol 3350), talc, and iron oxide.
- the disease or condition is an FXR mediated disease or condition.
- the FXR mediated diseases or conditions include, but not limited to, liver diseases such as a cholestatic liver disease such as primary biliary cirrhosis (PBC) also known as primary biliary cholangitis (PBC), primary sclerosing cholangitis (PSC), chronic liver disease, nonalcoholic fatty liver disease (NAFLD), nonalcoholic steatohepatitis (NASH), hepatitis C infection, alcoholic liver disease, liver damage due to progressive fibrosis, and liver fibrosis.
- PBC primary biliary cirrhosis
- PSC primary biliary cholangitis
- NAFLD nonalcoholic fatty liver disease
- NASH nonalcoholic steatohepatitis
- hepatitis C infection alcoholic liver disease
- liver damage due to progressive fibrosis and liver fibrosis
- liver fibrosis also include portal hypertension, bile acid diarrhea,
- the present disclosure provides methods of treating or preventing a disease or condition described herein by administering an obeticholic acid composition described herein (e.g. , obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, where the obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is in the form of particles, and wherein at least 50% of the particles have a diameter of 200 ⁇ or less).
- an obeticholic acid composition described herein e.g. , obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, where the obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is in the form of particles, and wherein at least 50% of the particles have a diameter of 200 ⁇ or less).
- the present disclosure provides a method of treating primary biliary cirrhosis (PBC) by administering an obeticholic acid composition described herein (e.g. , obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, where the obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is in the form of particles, and wherein at least 50% of the particles have a diameter of 200 ⁇ or less), optionally in a titration period.
- the method comprise administering a starting dose in a titration period. The starting dose, adjusted dose, and titration period are as described below.
- the PBC can be advanced stage PBC.
- “Advanced stage PBC” refers to PBC characterized by one or more of the following: Baseline total bilirubin > upper liming of normal (ULN); Baseline total ALP > 5x ULN; Baseline transient elastography (TE) > 10.7 kPa; Cirrhosis based on an initial or baseline biopsy result or patient having an Ishak score 6 (cirrhosis) or Ludwig/Scheuer PBC Stage 4; or Medical history of ascites, hepatic cirrhosis, jaundice, portal hypertension, portal hypertensive gastropathy or varices esophageal.
- PSC primary sclerosing cholangitis
- NAFLD nonalcoholic fatty liver disease
- NAFLD nonalcoholic steatohepatitis
- hepatitis C infection alcoholic liver disease
- alcoholic liver disease liver damage due to progressive fibrosis
- liver fibrosis liver fibrosis in a patient in need thereof by administering an effective amount of an obeticholic acid composition described above.
- the method is a method of treating NAFLD by administering an effective amount of an obeticholic acid composition described above.
- the method is a method of treating PSC by administering an effective amount of an obeticholic acid composition described above.
- the method is a method of treating fibrosis (e.g. , progressive or liver fibrosis) by administering an effective amount of an obeticholic acid composition described above.
- the method is a method of treating cirrhosis by administering an effective amount of an obeticholic acid composition described above.
- NAFLD is a medical condition that is characterized by the buildup of fat (called fatty infiltration) in the liver.
- NAFLD is one of the most common causes of chronic liver disease, and encompasses a spectrum of conditions associated with lipid deposition in hepatocytes. It ranges from steatosis (simple fatty liver), to nonalcoholic steatohepatitis (NASH), to advanced fibrosis and cirrhosis. The disease is mostly silent and is often discovered through incidentally elevated liver enzyme levels.
- NAFLD is strongly associated with obesity and insulin resistance and is currently considered by many as the hepatic component of the metabolic syndrome.
- Nonalcoholic steatohepatitis is a condition that causes inflammation and accumulation of fat and fibrous (scar) tissue in the liver. Liver enzyme levels in the blood may be more elevated than the mild elevations seen with nonalcoholic fatty liver (NAFL). Although similar conditions can occur in people who abuse alcohol, NASH occurs in those who drink little to no alcohol. NASH affects 2 to 5 percent of Americans, and is most frequently seen in people with one of more of the following conditions: obesity, diabetes, hyperlipidemia, insulin resistance, uses of certain medications, and exposure to toxins. NASH is an increasingly common cause of chronic liver disease worldwide and is associated with increased liver-related mortality and hepatocellular carcinoma, even in the absence of cirrhosis.
- the method is a method of treating NASH by administering an obeticholic acid composition described herein, optionally in a titration period as described herein.
- the NASH patient can be a high risk NASH patient.
- a "high risk NASH patient” refers to characterization by one or more of: NAS > 4; baseline fibrosis stage 2 or 3; or baseline fibrosis stage 1 with a comorbidity (type 2 diabetes, BMI > 30 kg/m2 or ALT > 60 U/L).
- the disease or condition is hyperlipidemia.
- the disease or condition is a cholestatic liver disease.
- the disease or condition is PBC.
- the disease or condition is a cardiovascular disease.
- the cardiovascular disease is atherosclerosis, hypercholesteremia, or hypertriglyceridemia.
- the present disclosure also provides a method for treating or preventing NAFLD or NASH. In one embodiment, the present disclosure provides a method for treating or preventing NAFLD or NASH that is associated with hyperlipidemia. In one embodiment, the present disclosure provides a method for treating or preventing NASH. In one embodiment, the present disclosure provides a method for treating or preventing NASH that is associated with hyperlipidemia.
- the present disclosure also provides a method for decreasing liver enzymes, comprising administering a therapeutically effective amount of the composition of the present disclosure to a subject in need thereof.
- the subject is not suffering from a cholestatic condition.
- the subject is suffering from a cholestatic condition.
- the liver enzyme is alkaline phosphatase, 7-glutamyl transpeptidase (GGT), and/or 5' nucleotidase.
- the methods described herein also include assessing, monitoring, measuring, or otherwise detecting liver function. Assessing, monitoring, measuring, or otherwise detecting liver function can be performed before, during, or after a titration period described herein, or in other instances, performed during the course of any treatment described herein. Liver function can be determined by, for example, assessing, monitoring, measuring, or otherwise detecting a level of one or more liver biomarkers compared to a control. In certain instances the control is a baseline taken from the patient before beginning treatment. In other instances the control is preestablished baseline considered as a normal value. [00181] Values for measure or detection of liver function biomarkers and controls can be expressed as a comparison to Upper Limit of Normal (ULN).
- UPN Upper Limit of Normal
- Liver biomarkers can be used to ascertain, quantify the efficacy of the course of treatment with an obeticholic acid composition described herein. In other instances, liver biomarkers described herein can be used to ascertain, quantify liver function during the course of treatment with an obeticholic acid composition described herein. Liver biomarkers can also be used to predict whether a patient or patient population will be susceptible to treatment with an obeticholic acid composition described herein.
- the liver biomarkers include assessing, monitoring, measuring or otherwise detecting an amount or level of aspartate transaminase (AST), alanine transaminase (ALT), alkaline phosphatase (ALP), bilirubin, glycine conjugated obeticholic acid, taurine conjugated obeticholic acid, a bile acid, a bile acid glycine conjugate, or a bile acid taurine conjugate.
- AST aspartate transaminase
- ALT alanine transaminase
- ALP alkaline phosphatase
- bilirubin glycine conjugated obeticholic acid
- taurine conjugated obeticholic acid taurine conjugated obeticholic acid
- a bile acid a bile acid glycine conjugate
- the liver biomarker assessed, monitored, measured, or detected can be ALP.
- the ALP level can be a measure of ULN.
- a patient before treatment can have an ALP level of at least 1.1 x ULN to at least 20 x ULN; at least 1.1 x ULN to at least 15 x ULN; at least 1.1 x ULN to at least 12 x ULN; at least 1.1 x ULN to at least 10 x ULN; at least 1.1 x ULN to at least 8 x ULN; at least 1.1 x ULN to at least 6 x ULN; at least 1.1 x ULN to at least 5 x ULN; at least 1.1 x ULN to at least 4 x ULN; at least 1.1 x ULN to at least 3 x ULN; or at least 1.1 x ULN to at least 2 x ULN.
- a patient before a treatment described herein can have an ALP level of about 1.5 x ULN to about 20 x ULN; about 1.5 x ULN to about 15 x ULN; about 1.5 x ULN to about 10 ULN; about 1.5 x ULN to about 5 x ULN; or about 1.5 x ULN to about 3 x ULN.
- a patient before treatment can have an ALP level before a treatment described herein of about 1.5x, 2x, 3x, 4x, 5x, 8x, 10 x, 15x, or 20x ULN.
- a patient before treatment can have an ALP level before a treatment described herein of greater than about 1.5x, 2x, 3x, 4x, 5x, 8x, 10x, 15x, or 20x ULN.
- a patient has an ALP level of about 1.5 x ULN.
- a patient has an ALP level of about 2 x ULN.
- a patient has a ALP level of about 5 x ULN.
- a patient has an ALP level of about 10 x ULN.
- a patient has a bilirubin level of about 15 x ULN.
- a patient has an ALP level greater than about 1.5 x ULN.
- a patient has an ALP level greater than about 2 x ULN. In one embodiment, a patient has a ALP level greater than about 5 x ULN. In one embodiment, a patient has an ALP level greater than about 10 x ULN. In one embodiment, a patient has a bilirubin level greater than about 15 x ULN.
- the liver biomarker assessed, monitored, measured, or detected can be bilirubin.
- the bilirubin level can be a measure of ULN.
- a patient before treatment can have a bilirubin level of at least 1.1 x ULN to at least 20 x ULN; at least 1.1 x ULN to at least 15 x ULN; at least 1.1 x ULN to at least 12 x ULN; at least 1.1 x ULN to at least 10 x ULN; at least 1.1 x ULN to at least 8 x ULN; at least 1.1 x ULN to at least 6 x ULN; at least 1.1 x ULN to at least 5 x ULN; at least 1.1 x ULN to at least 4 x ULN; at least 1.1 x ULN to at least 3 x ULN; or at least 1.1 x ULN to at least 2 x ULN;
- a patient before a treatment described herein can have a bilirubin level of about 1.5 x ULN to about 20 x ULN; about 1.5 x ULN to about 15 x ULN; about 1.5 x ULN to about 10 ULN; about 1.5 x ULN to about 5 x ULN; or about 1.5 x ULN to about 3 x ULN.
- a patient before a treatment described herein can have a bilirubin level of about 2 x ULN to about 20 x ULN; about 2 x ULN to about 15 x ULN; about 2 x ULN to about 10 ULN; about 2 x ULN to about 5 x ULN; or about 2 x ULN to about 3 x ULN.
- a patient before a treatment described herein can have a bilirubin level of greater than about 2 x ULN to greater than about 20 x ULN; greater than about 2 x ULN to greater than about 15 x ULN; greater than about 2 x ULN to greater than about 10 ULN; greater than about 2 x ULN to greater than about 5 x ULN; or greater than about 2 x ULN to greater than about 3 x ULN.
- a patient before treatment can have a bilirubin level before a treatment described herein of about 1.5x, 2x, 3x, 4x, 5x, 8x, 10x, 15x, or 20x ULN.
- a patient before treatment can have a bilirubin level before a treatment described herein of greater than about 1.5x, 2x, 3x, 4x, 5x, 8x, 10 x, 15x, or 20x ULN.
- a patient has a bilirubin level greater than about 2 x ULN.
- a patient has a bilirubin level greater than about 5 x ULN.
- a patient has a bilirubin level greater than about 10 x ULN. In one embodiment, a patient has a bilirubin level greater than about 15 x ULN. In one embodiment, a patient has a bilirubin level less than about 2 x ULN. In one embodiment, a patient has a bilirubin level less than about 5 x ULN. In one embodiment, a patient has a bilirubin level less than about 10 x ULN. In one embodiment, a patient has a bilirubin level less than about 15 x ULN.
- a patient has an ALP level as provided above (e.g. , about 1.5 x ULN to about 10 x ULN) and a bilirubin level as provided above (e.g. , less than about 5 x ULN).
- the patient has an ALP level between about 1.5 x ULN to about 10 x ULN and a bilirubin level less than about 2 x ULN.
- Treatment with a obeticholic acid composition described herein can reduce the levels of ALP and/or bilirubin in a patient described herein.
- a disease or condition described herein e.g. , PBC
- an obeticholic acid composition described herein can reduce the level of ALP by 2, 4, 5, 6, 8, 9, 10, 12, 15, 18, 20, 21 , 22, 23, 24, 25, 26, 27, 28, 29, 30, 35, 40, 45, 50, 55, 60, 65, 70, 75, 80, 85, 88, 90, 92, 94, 96, 97, 98, 99, 99.2, 99.4, 99.6, 99.7, 99.8, 99.9, or 100%.
- the level of ALP can be reduced by at least 100%, at least 125%, at least 150%, at least 175%, at least 200%, at least 225%, at least 250% or at least 300%. [00191] In another example, the level of ALP can be reduced by about 5% to about 50%; about 10% to about 55%; about 10% to about 45%; about 10% to about 40%; about 10% to about 33%, about 10% to about 30%; about 15% to about 30%; about 15% to about 25%; about 20% to about 50%, about 20% to about 40%; about 20% to about 35%; about 20% to about 30%; 20% to about 27%; or about 20% to about 27%. In another example, the level of ALP can be reduced by at least 50%. The level of ALP can be reduced by at least 40%.
- the level of ALP can be reduced by at least 35%.
- the level of ALP can be reduced by at least 30%.
- the level of ALP can be reduced by at least 27%.
- the level of ALP can be reduced by at least 25%.
- the level of ALP can be reduced by at least 20%.
- the reduction of ALP levels can be represented by the fold change over ULN.
- treatment with an obeticholic acid described herein can reduce the ALP level of a patient described herein to less than about 5 x ULN; less than about 4 x ULN, less than about 3 x ULN, less than about 2 x ULN, less than about 1.7 x ULN, less than about 1.5 x ULN, less than about 1.25 x ULN, or less than about ULN.
- the ALP level is reduced by at least 1 , 2, 3, 4, 5, 6, 7, 8, 9, 10, 15, 20, 25, 30, 40, or 50 fold compared to a baseline value.
- the ALP level after treatment with an obeticholic acid composition described herein can be reduced by 1 , 1,2, 1,4, 1.6, 1.8, or 2 fold, including intervening values therein, compared to a baseline value.
- the ALP level can be reduced by 2, 2.2, 2.4, 2.6, 2.8, or 3 fold, including intervening values therein, compared to a baseline value.
- the ALP level can be reduced 3, 4, or 5 fold, including intervening values therein, compared to a baseline value.
- the ALP level can be reduced 5, 7, 9, or 10 fold, including intervening values therein, compared to a baseline value. In another example, the ALP level can be reduced 10, 12, 15, or 20 fold, including intervening values therein, compared to a baseline value.
- Treatment of a disease or condition described herein (e.g. , PBC) with an obeticholic acid composition described herein can reduce the level of bilirubin by 2, 4, 5, 6, 8, 9, 10, 12, 15, 18, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 35, 4-, 45, 50, 55, 60, 65, 70, 75, 80, 85, 88, 90, 92, 94, 96, 97, 98, 99, 99.2, 99.4, 99.6, 99.7, 99.8, 99.9, or 100%.
- the level of bilirubin can be reduced by at least 100%, at least 125%, at least 150%, at least 175%, at least 200%, at least 225%, at least 250% or at least 300%.
- the level of bilirubin can be reduced by about 5% to about 50%; about 10% to about 55%; about 10% to about 45%; about 10% to about 40%; about 10% to about 33%, about 10% to about 30%; about 15% to about 30%; about 15% to about 25%; about 20% to about 50%, about 20% to about 40%; about 20% to about 35%; about 20% to about 30%; 20% to about 27%; or about 20% to about 27%.
- the level of bilirubin can be reduced by at least 50%.
- the level of bilirubin can be reduced by at least 40%.
- the level of bilirubin can be reduced by at least 35%.
- the level of bilirubin can be reduced by at least 30%.
- the level of bilirubin can be reduced by at least 27%.
- the level of bilirubin can be reduced by at least 25%.
- the level of bilirubin can be reduced by at least 20%.
- the reduction of bilirubin levels can be represented by the fold change over ULN.
- treatment with an obeticholic acid described herein can reduce the bilirubin level of a patient described herein to less than about 5 x ULN; less than about 4 x ULN, less than about 3 x ULN, less than about 2 x ULN, less than about 1.7 x ULN, less than about 1.5 x ULN, less than about 1.25 x ULN, or less than about ULN.
- the bilirubin level is reduced by at least 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 15, 20, 25, 30, 40, or 50 fold compared to a baseline value.
- the bilirubin level after treatment with an obeticholic acid composition described herein can be reduced by 1, 1,2, 1,4, 1.6, 1.8, or 2 fold, including intervening values therein, compared to a baseline value.
- the bilirubin level can be reduced by 2, 2.2, 2.4, 2.6, 2.8, or 3 fold, including intervening values therein, compared to a baseline value.
- the bilirubin level can be reduced 3, 4, or 5 fold, including intervening values therein, compared to a baseline value.
- the bilirubin level can be reduced 5, 7, 9, or 10 fold, including intervening values therein, compared to a baseline value. In another example, the bilirubin level can be reduced 10, 12, 15, or 20 fold, including intervening values therein, compared to a baseline value.
- one or more biomarkers can stratify a patient population undergoing or who will undergo treatment with an obeticholic acid composition described herein.
- a PBC patient can be stratified for the risk of hepatocellular carcinoma (HCC).
- HCC hepatocellular carcinoma
- liver biomarkers useful for detection can include metabolites and bile acids.
- assessing, monitoring, measuring, or otherwise detecting levels of glycine and taurine conjugates of obeticholic acid can be useful for measuring efficacy of a treatment regimen described herein.
- assessing, monitoring, measuring, or otherwise detecting levels or detecting plasma levels of bile acids including cholic acid, chenodeoxycholic acid, deoxycholic acid, lithocholic acid, and urosodeoxycholic acid, including glycine and taurine conjugates thereof, and optionally comparing the levels to a control can be useful for measuring efficacy of a treatment regimen described herein.
- calculating an AST to platelet index can be useful for assessing, monitoring, measuring, or otherwise detecting liver function (including changes thereof).
- the obeticholic acid compositions described herein can reduce the APR! of a patient described herein.
- monitoring or measuring the APR! can be used to determine efficacy of treatment with an obeticholic acid composition described herein.
- a reduction in APRI is observed in a patient (e.g., a PBC or NASH patient) after administration of an obeticholic acid composition described herein.
- the APRI may be reduced by about 5 % to about 50 % in patients treated with obeticholic acid relative to baseline levels measured before dose administration.
- the reduction may be up to about 5%, 10%, 15%, 20%, 25%, 30%, 35%, 40%, 45% or 50%.
- the method includes assessing liver function of the patient before, during, and after said titration period by either calculating an APRI score for said patient; or by measuring the level of one or more liver biomarker selected from ALP, bilirubin, AST, ALT, glycine conjugated obeticholic acid, taurine conjugated obeticholic acid, a bile acid, a bile acid glycine conjugate, or a bile acid taurine conjugate, where a reduced APRI score compared to a control or a reduced level of the one or more liver biomarkers compared to a control indicates non-impaired liver function.
- the method further includes assessing tolerance of the patient to the starting dose by grading the severity of one or more adverse effects, if present, and administering an adjusted dose of the obeticholic acid composition, where the adjusted dose includes an amount equal to or greater than an amount of the starting dose.
- the starting dose, adjusted dose, and titration period are as described below.
- the starting dose can be about 5 to about 50 mg (e.g. , 5 mg) and the adjusted dose can be about 5 to about 50 mg (e.g. , 5 mg, 10 mg, or 25 mg) and the titration period can be a time of about 1 to about 6 months, e.g. , 1 month, 2 months, 3 months, 4 months, 5 months, or 6 months.
- administration of an obeticholic acid composition described herein reduces expression or levels of ALP and/or bilirubin.
- administration of an obeticholic acid composition described herein reduces ALP and bilirubin levels, thereby reducing transplant complications or rejection.
- administration of an effective amount of an obeticholic acid composition described herein increases posttransplantation survival rate of a liver transplantee.
- obeticholic acid may mediate its action primarily via FXR agonism, wherein FGF-19 released from gut enterocytes (in response to FXR agonist) into portal circulation down regulates endogenous bile acid synthesis in the liver.
- FXR agonism FGF-19 released from gut enterocytes (in response to FXR agonist) into portal circulation down regulates endogenous bile acid synthesis in the liver.
- the present disclosure comprehends a method of measuring FXR agonist activity by, for example, measuring release of FGF-19 into the bloodstream or circulation of a patient administered with OCA. Levels of FGF- 19 may be measured by methods known in the art, such as those described herein.
- Obeticholic acid administration may lead to a significant and a dose-dependent increase in the levels of FGF-19 and in some embodiments, a decrease in the levels of endogenous bile acids and C4 (a bile acid precursor).
- a significant increase in FGF-19 levels may be observed from baseline to month 3, month 6 and month 12 after dose administration.
- the FGF-19 levels may increase from about 5% to about 200 %. In specific embodiments, the levels may increase by about 5%, 10%, 15%, 20%, 25%, 30%, 35%, 40%, 45%, 50%, 55%, 60%, 65%, 70%, 75%, 80%, 85%, 90%, 95% or 100%.
- the plasma levels of FGF-19, a marker of FXR activation are determined using a qualified method and a validated method using an enzyme-linked immunosorbent assay (ELISA) method.
- the plasma concentrations of FGF-19 may be quantitated at predose and after administration of dose.
- a monoclonal antibody specific for FGF-19 is pre-coated onto a microplate.
- Standards, quality controls and samples are pipetted into the wells and any FGF-19 present is bound by the immobilized antibody.
- an enzyme-linked polyclonal antibody specific for FGF-19 is added to the wells.
- a substrate solution is added to the wells and color develops in the proportion to the amount of FGF-19 bound in the initial step. The color development is stopped and the intensity of the color is measured.
- the calibration range of the method is 15.625 pg/ml to 1000 pg/ml for FGF-19 using a 100 ⁇ aliquot of standard curve, quality control and sample. In some embodiments, no minimum required dilution is used. In other embodiments, samples may be subjected to a 3x minimum required dilution.
- administration of an obeticholic acid composition described herein reduces expression or levels of ALP and/or bilirubin.
- administration of an obeticholic acid composition described herein reduces ALP and bilirubin levels, thereby reducing transplant complications or rejection.
- administration of an effective amount of an obeticholic acid composition described herein increases post-transplantation survival rate of a liver transplantee.
- a method of treating a solid-tumor cancer by administering an effective amount of an obeticholic acid composition as described herein include treating hepatocellular carcinoma (HCC), colorectal cancer, gastric cancer, liver cancer, breast cancer, renal cancer, or pancreatic cancer by administering an obeticholic acid composition as described herein.
- HCC hepatocellular carcinoma
- colorectal cancer gastric cancer
- liver cancer breast cancer
- renal cancer or pancreatic cancer
- pancreatic cancer by administering an obeticholic acid composition as described herein.
- HCC hepatocellular carcinoma
- colorectal cancer by administering an effective amount of an obeticholic acid composition as described herein.
- in another embodiment is a method of treating gastric cancer by administering an effective amount of an obeticholic acid composition as described herein.
- a method of treating liver cancer by administering an effective amount of an obeticholic acid composition as described herein.
- a method of treating renal cancer by administering an effective amount of an obeticholic acid composition as described herein.
- a method of treating pancreatic cancer by administering an effective amount of an obeticholic acid composition as described herein. It is understood that the treatment of a cancer described herein can be performed by administering an effective amount of an obeticholic acid composition described herein in combination with one or more anticancer agents, such as those described herein. In some embodiments, the effective amount administered is a starting dose as described herein.
- the autoimmune disease is selected from multiple sclerosis, rheumatoid arthritis, and type I diabetes.
- a method of treating type I diabetes by administering an effective amount of an obeticholic acid composition as described herein.
- the treatment of the autoimmune disease includes further administering another active agent useful for the treatment, such as without limitation, non-steroidal anti-inflammatory agents (NSAIDs) such as ibuprofen, naproxen, corticosteroids, disease-modifying anti-rheumatic drugs such as methotrexate (Trexall, Otrexup, Rasuvo), lefiunomide (Arava),
- NSAIDs non-steroidal anti-inflammatory agents
- ibuprofen such as ibuprofen, naproxen, corticosteroids
- disease-modifying anti-rheumatic drugs such as methotrexate (Trexall, Otrexup, Rasuvo), lefiunomide (Arava)
- hydroxychloroquine and sulfasalazine (Azulfidine), biologic agents such as abatacept (Orencia), adalimumab (Humira), anakinra (Kineret), certolizumab (Cimzia), etanercept (Enbrel), golimumab (Simponi), infliximab (Remicade), rituximab (Rituxan), tocilizumab (Actemra) and tofacitinib (Xeljanz), interferons, such as interferon alpha, interferon beta, interferon gamma, and PEGylated versions thereof, glatiramer acetate (also known in the art as Copaxone), dimethyl fumarate (also known in the art as Tecfidera), fingolimod (also known in the art as Gilenya), teriflunomide (also known in
- an obeticholic acid composition described herein can be administered in combination with metformin, insulin, insulin mimetic, or any other known anti-diabetic or anti-glycemic agent for treatment of diabetes.
- the effective amount administered is a starting dose as described herein.
- the present disclosure also provides a method for inhibiting or reversing fibrosis, comprising administering a therapeutically effective amount of the composition of the present disclosure to a subject in need thereof.
- the subject is not suffering from a cholestatic condition.
- the subject is suffering from a cholestatic condition.
- the subject is not suffering from a cholestatic condition associated with a disease or condition selected from the group consisting of cancers, such as, e.g. , cancers as described herein, including primary liver and biliary cancer, metastatic cancer, sepsis, chronic total parenteral nutrition, cystic fibrosis, and granulomatous liver disease.
- cancers such as, e.g. , cancers as described herein, including primary liver and biliary cancer, metastatic cancer, sepsis, chronic total parenteral nutrition, cystic fibrosis, and granulomatous liver disease.
- the fibrosis to be inhibited occurs in an organ where FXR is expressed.
- a cholestatic condition is defined as having an abnormally elevated serum level of alkaline phosphatase, 7-glutamyl transpeptidase (GGT), and/or 5 ' nucleotidase.
- a cholestatic condition is further defined as presenting with at least one clinical symptom.
- the symptom is itching (pruritus).
- a cholestatic condition is selected from the group consisting of primary biliary cirrhosis (PBC), primary sclerosing cholangitis (PBS), biliary atresia, drug-induced cholestasis, hereditary cholestasis, and intrahepatic cholestasis of pregnancy.
- PBC primary biliary cirrhosis
- PBS primary sclerosing cholangitis
- biliary atresia drug-induced cholestasis
- hereditary cholestasis hereditary cholestasis
- intrahepatic cholestasis of pregnancy intrahepatic cholestasis
- the fibrosis is selected from the group consisting of liver fibrosis, kidney fibrosis, and intestinal fibrosis.
- the subject has liver fibrosis associated with a disease selected from the group consisting of hepatitis B; hepatitis C; parasitic liver diseases; post- transplant bacterial, viral and fungal infections; alcoholic liver disease (ALD); non-alcoholic fatty liver disease (NAFLD); non-alcoholic steatohepatitis (NASH); liver diseases induced by methotrexate, isoniazid, oxyphenistatin, methyldopa, chlorpromazine, tolbutamide, or amiodarone; autoimmune hepatitis; sarcoidosis; Wilson's disease; hemochromatosis; Gaucher' s disease; types III, IV, VI, IX and X glycogen storage diseases; ai-antitrypsin deficiency; Zellweger syndrome; tyrosinemia; fructosemia; galactosemia; vascular derangement associated with Budd-Chiari syndrome, veno-occlusive disease, or portal vein
- a disease selected from
- the subject has intestinal fibrosis associated with a disease selected from the group consisting of Crohn's disease, ulcerative colitis, post-radiation colitis, and microscopic colitis.
- the subject has renal fibrosis associated with a disease selected from the group consisting of diabetic nephropathy, hypertensive nephrosclerosis, chronic glomerulonephritis, chronic transplant glomerulopathy, chronic interstitial nephritis, and polycystic kidney disease.
- a disease selected from the group consisting of diabetic nephropathy, hypertensive nephrosclerosis, chronic glomerulonephritis, chronic transplant glomerulopathy, chronic interstitial nephritis, and polycystic kidney disease.
- the present disclosure also provides a method for treating or preventing all forms of conditions related to elevated lipid levels.
- the condition is hyperlipidemia where it is associated with a condition selected from resistant primary biliary cirrhosis; primary biliary cirrhosis where there is associated liver function test elevation and hyperlipidemia, primary sclerosing cholangitis, non-alcohol-induced steatohepatitis; and chronic liver disease associated with hepatitis B, C or alcohol.
- the present disclosure provides a method for treating or preventing
- hyperlipidemia where the hyperlipidemia is primary hyperlipidemia with or without a genetic component, or hyperlipidemia associated with coronary artery disease,
- cerebrovascular arterial disease cerebrovascular arterial disease, peripheral vascular disease, aortic aneurisms, or carotid atherosclerosis.
- the present disclosure provides a method for treating or preventing primary sclerosing cholangitis for similar biochemical abnormalities, as well as chronic hepatitis caused by hepatitis B, C or by alcohol. In one aspect, the present disclosure provides a method for treating or preventing other arterial disorders associated with hyperlipidemia. In one aspect, the present disclosure provides a method for treating or preventing
- Therapies with FXR agonists may produce various side effects, one of which is pruritus.
- Pruritus or itch is defined as an unpleasant sensation of the skin that provokes the urge to scratch. It is a characteristic feature of many skin diseases and an unusual sign of some systemic diseases. Pruritus may be localized or generalized and can occur as an acute or chronic condition. Itching lasting more than 6 weeks is termed chronic pruritus. Itching can be intractable and incapacitating, as well as a diagnostic and therapeutic challenge.
- compositions of the present disclosure includes a decrease in the incidence and/or severity of pruritus in subjects treated with the compositions and according to the methods of the present disclosure.
- the incidence of pruritus decreases by at least 5%, 10%, 15%, 20%, 25%, 30%, 35%, 40%, 45%, or 50% in subjects treated with the compositions of the present disclosure. In a further embodiment, the incidence of pruritus decreases by at least 20%, 25%, 30%, 35%, 40%, 45%, or 50% in subjects treated with the compositions of the present disclosure. In a further embodiment, the incidence of pruritus decreases by at least 5%, 10%, 15%, 20%, 25%, 30%, 35%, 40%, 45%, or 50% in subjects treated with the compositions of the present disclosure during the first one month, two months, three months, four months, five months, or six months after the beginning of the treatment.
- the incidence of pruritus decreases by at least 20%, 25%, 30%, 35%, 40%, 45%, or 50% in subjects treated with the compositions of the present disclosure during the first one month, two months, three months, four months, five months, or six months after the beginning of the treatment.
- the severity of the pruritus decreases by at least 5%, 10%, 15%, 20%, 25%, 30%, 35%, 40%, 45%, or 50% in subjects treated with the compositions of the present disclosure. In a further embodiment, the severity of pruritus decreases by at least 20%, 25%, 30%, 35%, 40%, 45%, or 50% in subjects treated with the compositions of the present disclosure. In a further embodiment, the severity of pruritus decreases by at least 5%, 10%, 15%, 20%, 25%, 30%, 35%, 40%, 45%, or 50% in subjects treated with the compositions of the present disclosure during the first one month, two months, three months, four months, five months, or six months after the beginning of the treatment.
- the severity of pruritus decreases by at least 20%, 25%, 30%, 35%, 40%, 45%, or 50% in subjects treated with the compositions of the present disclosure during the first one month, two months, three months, four months, five months, or six months after the beginning of the treatment.
- Obeticholic acid compositions described herein can be administered to a patient in an amount of between about: 1 mg to about 50 mg; 1 to about 40 mg; 1 to about 30 mg; 1 to about 25 mg; 1 to about 20 mg; 1 mg to about 10 mg; or 1 mg to about 5 mg.
- the obeticholic acid composition can be administered to a patient in an amount of about: 5 to about 50 mg; 5 to about 40 mg; 5 to about 30 mg; 5 to about 25 mg; 5 to about 20 mg; or 5 to about 10 mg.
- the obeticholic acid composition can be administered in an amount of about 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 1 1, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 30, 35, 40, 45, or 50 mg.
- the obeticholic acid composition described herein can be administered at an amount of about 5 mg, 10 mg, 15 mg, 25 mg, or 50 mg.
- an effective amount of a obeticholic acid composition described herein can be about 5 mg, 10 mg, 25 mg, or 50 mg.
- the amount of a starting dose of an obeticholic acid composition described herein can be about 5 mg, 10 mg, 25 mg, or 50 mg.
- the amount of an adjusted dose or re-adjusted dose of an obeticholic acid composition described herein can be about 5 mg, 10 mg, 25 mg, or 50 mg. It is to be understood the amount of an obeticholic acid composition described herein as administered to a patient described herein refers to the amount of obeticholic acid in the composition.
- the amount of an obeticholic acid composition as provided above can refer to an effective amount as described herein.
- an effective amount of the obeticholic acid composition administered to a patient described herein can be 5 mg.
- an effective amount of the obeticholic acid composition administered to a patient described herein can be 10 mg.
- an effective amount of the obeticholic acid composition administered to a patient described herein can be 25 mg.
- administered to a patient described herein can be 50 mg.
- the amount of an obeticholic acid composition as provided above can optionally refer to a starting dose administered during a titration period as described herein.
- a starting dose of the obeticholic acid composition administered to a patient described herein can be 5 mg.
- a starting dose of the obeticholic acid composition administered to a patient described herein can be 10 mg.
- a starting dose of the obeticholic acid composition administered to a patient described herein can be 25 mg.
- a starting dose of the obeticholic acid composition administered to a patient described herein can be 50 mg.
- the amount of an obeticholic acid composition as provided above can refer to an adjusted dose administered after a titration period as described herein.
- an adjusted dose of the obeticholic acid composition administered to a patient described herein can be 5 mg. In another embodiment, an adjusted dose of the obeticholic acid composition administered to a patient described herein can be 10 mg. In still another embodiment, an adjusted dose of the obeticholic acid composition administered to a patient described herein can be 25 mg. In yet another embodiment, an adjusted dose of the obeticholic acid composition administered to a patient described herein can be 50 mg.
- the amount of an obeticholic acid composition as provided above can refer to a re-adjusted dose administered after a titration period as described herein.
- a re-adjusted dose of the obeticholic acid composition administered to a patient described herein can be 5 mg.
- a re-adjusted dose of the obeticholic acid composition administered to a patient described herein can be 10 mg.
- a re-adjusted dose of the obeticholic acid composition administered to a patient described herein can be 25 mg.
- a re-adjusted dose of the obeticholic acid composition administered to a patient described herein can be 50 mg.
- obeticholic acid is usually administered in the form of pharmaceutical formulations comprising a pharmaceutically acceptable excipient and obeticholic acid. These formulations can be administered by a variety of routes including oral, buccal, rectal, intranasal, transdermal, subcutaneous, intravenous, intramuscular, and intranasal. Oral formulation of obeticholic acid are described further herein under the section entitled "Oral Formulation and Administration”.
- obeticholic acid can be administered transdermally.
- a transdermal delivery device (“patch") is needed.
- Such transdermal patches may be used to provide continuous or discontinuous infusion of a compound of the present disclosure in controlled amounts.
- the construction and use of transdermal patches for the delivery of pharmaceutical agents is well known in the art. See, e.g. , U.S. Patent No. 5,023,252.
- Such patches may be constructed for continuous, pulsatile, or on demand delivery of pharmaceutical agents.
- compositions suitable for injectable use include sterile aqueous solutions (where water soluble) or dispersions and sterile powders for the extemporaneous preparation of sterile injectable solutions or dispersion.
- suitable carriers include physiological saline, bacteriostatic water, Cremophor ELTM (BASF, Parsippany, N.J.) or phosphate buffered saline (PBS).
- the composition must be sterile and should be fluid to the extent that easy syringeability exists. It must be stable under the conditions of manufacture and storage and must be preserved against the contaminating action of microorganisms such as bacteria and fungi.
- the carrier can be a solvent or dispersion medium containing, for example, water, ethanol, polyol (for example, glycerol, propylene glycol, and liquid polyethylene glycol, and the like), and suitable mixtures thereof.
- the proper fluidity can be maintained, for example, by the use of a coating such as lecithin, by the maintenance of the required particle size in the case of dispersion and by the use of surfactants.
- Prevention of the action of microorganisms can be achieved by various antibacterial and antifungal agents, for example, parabens, chlorobutanol, phenol, ascorbic acid, thimerosal, and the like.
- isotonic agents for example, sugars, polyalcohols such as mannitol, sorbitol, sodium chloride in the composition.
- Prolonged absorption of the injectable compositions can be brought about by including in the composition an agent which delays absorption, for example, aluminum monostearate and gelatin.
- Sterile injectable solutions can be prepared by incorporating the active compound, obeticholic acid or obeticholic acid particles, in the required amount in an appropriate solvent with one or a combination of ingredients enumerated herein, as required, followed by filtered sterilization.
- dispersions are prepared by incorporating the obeticholic acid into a sterile vehicle that contains a basic dispersion medium and the required other ingredients from those enumerated above.
- methods of preparation are vacuum drying and freeze-drying that yields a powder of the obeticholic acid or obeticholic acid particles, plus any additional desired ingredient from a previously sterile-filtered solution thereof.
- Oral compositions generally include an inert diluent or an edible pharmaceutically acceptable carrier. They can be enclosed in gelatin capsules or compressed into tablets. For the purpose of oral therapeutic administration, the active compound, obeticholic acid or obeticholic acid particles, can be incorporated with excipients and used in the form of tablets, troches, or capsules. Oral compositions can also be prepared using a fluid carrier for use as a mouthwash, wherein the obeticholic acid or obeticholic acid particles in the fluid carrier is applied orally and swished and expectorated or swallowed.
- compositions can contain any of the following ingredients, or compounds of a similar nature: a binder such as microcrystalline cellulose, gum tragacanth or gelatin; an excipient such as sodium starch glycolate, starch or lactose, a diluent such as microcrystalline cellulose, a disintegrating agent such as alginic acid, Primogel, or corn starch; a lubricant such as magnesium stearate or Sterotes; a glidant such as colloidal silicon dioxide; a sweetening agent such as sucrose or saccharin; or a flavoring agent such as peppermint, methyl salicylate, or orange flavoring.
- a binder such as microcrystalline cellulose, gum tragacanth or gelatin
- an excipient such as sodium starch glycolate, starch or lactose, a diluent such as microcrystalline cellulose, a disintegrating agent such as alginic acid, Primogel, or corn starch
- a lubricant such as magnesium
- the obeticholic acid or obeticholic acid particles is delivered in the form of an aerosol spray from pressured container or dispenser, which contains a suitable propellant, e.g., a gas such as carbon dioxide, or a nebulizer.
- a suitable propellant e.g., a gas such as carbon dioxide, or a nebulizer.
- Systemic administration can also be by transmucosal or transdermal means.
- penetrants appropriate to the barrier to be permeated are used in the formulation.
- penetrants are generally known in the art, and include, for example, for transmucosal administration, detergents, bile salts, and fusidic acid derivatives.
- Transmucosal administration can be accomplished through the use of nasal sprays or suppositories.
- the obeticholic acid or obeticholic acid particles is formulated into ointments, salves, gels, or creams as generally known in the art.
- the obeticholic acid or obeticholic acid particles can be prepared with pharmaceutically acceptable carriers that will protect the compound against rapid elimination from the body, such as a controlled release formulation, including implants and
- Biodegradable, biocompatible polymers can be used, such as ethylene vinyl acetate, polyanhydrides, polyglycolic acid, collagen, polyorthoesters, and polylactic acid. Methods for preparation of such formulations will be apparent to those skilled in the art. The materials can also be obtained commercially from Alza Corporation and Nova Pharmaceuticals, Inc. Liposomal suspensions (including liposomes targeted to infected cells with monoclonal antibodies to viral antigens) can also be used as
- Dosage unit form refers to physically discrete units suited as unitary dosages for the subject to be treated; each unit containing a predetermined quantity of obeticholic acid or obeticholic acid particles calculated to produce the desired therapeutic effect in association with the required pharmaceutical carrier.
- the specification for the dosage unit forms of the disclosure are dictated by and directly dependent on the unique characteristics of the obeticholic acid or obeticholic acid particles and the particular therapeutic effect to be achieved.
- a pharmaceutical formulation comprising at least obeticholic acid as described above in a formulation adapted for buccal and/or sublingual, or nasal administration.
- obeticholic acid in a manner that avoids gastric complications, such as first pass metabolism by the gastric system and/or through the liver. This administration route may also reduce adsorption times, providing more rapid onset of therapeutic benefit.
- the compounds of the present disclosure may provide particularly favorable solubility profiles to facilitate sublingual/buccal formulations. Such formulations typically require relatively high concentrations of active ingredients to deliver sufficient amounts of active ingredients to the limited surface area of the sublingual/buccal mucosa for the relatively short durations the formulation is in contact with the surface area, to allow the absorption of the active ingredient. Thus, the very high activity of obeticholic acid, combined with its high solubility, facilitates its suitability for sublingual/buccal formulation.
- Obeticholic acid is preferably formulated in a unit dosage form, each dosage containing from about 0.05 mg to about 1500 mg.
- the formulation comprises about 0.05 mg to about 100 mg.
- the formulation comprises about 1 mg to about 100 mg.
- the formulation comprises about 0.05 mg to about 50 mg.
- the formulation comprises about 0.05 mg to about 30 mg.
- the formulation comprises about 0.05 mg to about 20 mg.
- the formulation comprises about 0.5 mg to about 30 mg.
- the formulation comprises about 0.5 mg to about 25 mg.
- the formulation comprises about 1 mg to about 25 mg.
- the formulation comprises about 4 mg to about 26 mg.
- the formulation comprises about 5 mg to about 25 mg. In yet another embodiment, the formulation comprises about 0.05 mg to about 2 mg. In another embodiment, the formulation comprises about 1 mg to about 2 mg. In one embodiment, the formulation comprises about 1.2 mg to about 1.8 mg. In one embodiment, the formulation comprises about 1.3 mg to about 1.7 mg. In one embodiment, the formulation comprises about 1.5 mg. In one embodiment, the formulation comprises about 0.05 mg to about 0.5 mg. In another embodiment, the formulation comprises about 0.08 mg to about 0.8 mg. In yet another embodiment, the formulation comprises about 0.1 mg to about 0.5 mg. In another embodiment, the formulation comprises about 0.25 mg.
- Obeticholic acid is generally effective over a wide dosage range.
- dosages per day normally fall within the range of about 0.0001 to about 30 mg/kg of body weight.
- the range of about 0.1 to about 15 mg/kg/day, in single or divided dose is especially preferred.
- the formulation comprises about 0.05 mg to about 1500 mg.
- the formulation comprises about 0.05 mg to about 100 mg.
- the formulation comprises about 1 mg to about 100 mg.
- the formulation comprises about 0.05 mg to about 50 mg.
- the formulation comprises about 0.05 mg to about 30 mg.
- the formulation comprises about 0.05 mg to about 20 mg.
- the formulation comprises about 0.05 mg to about 10 mg.
- the formulation comprises about 3 mg to about 30 mg. In another embodiment, the formulation comprises about 0.05 mg to about 25 mg. In another embodiment, the formulation comprises about 4 mg to about 25 mg. In another embodiment, the formulation comprises about 5 mg to about 25 mg. In another embodiment, the formulation comprises about 5 mg to about 10 mg. In one embodiment, the formulation comprises about 1 mg to about 2 mg. In one embodiment, the formulation comprises about 1.2 mg to about 1.8 mg. In one embodiment, the formulation comprises about 1.3 mg to about 1.7 mg. In one embodiment, the formulation comprises about 0.05 mg to about 0.5 mg. In another embodiment, the formulation comprises about 0.08 mg to about 0.8 mg. In yet another embodiment, the formulation comprises about 0.1 mg to about 0.5 mg. In another embodiment, the formulation comprises about 25 mg.
- the formulation comprises about 10 mg. In one embodiment, the formulation comprises about 5 mg. In another embodiment, the formulation comprises about 0.25 mg.
- the amount of obeticholic acid actually administered will be determined by a physician, in the light of the relevant circumstances, including the condition to be treated, the chosen route of administration, the form of obeticholic acid administered, the age, weight, and response of the individual patient, and the severity of the patient's symptoms, and therefore the above dosage ranges are not intended to limit the scope of the disclosure in any way. In some instances dosage levels below the lower limit of the aforesaid range may be more than adequate, while in other cases still larger doses may be employed without causing any harmful side effect, provided that such larger doses are first divided into several smaller doses for administration throughout the day.
- the tablet of the present disclosure can comprise an intra-granular portion and an extra-granular portion.
- the intra-granular portion can contain obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, and one or more pharmaceutical excipients.
- the extra-granular portion can contain obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, and one or more pharmaceutical excipients.
- the intra-granular portion and the extra- granular portion of the tablet contain obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, and one or more pharmaceutical excipients.
- the intra-granular portion contains obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof and/or the extra-granular portion does not contain obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof.
- microcrystalline cellulose in the intra-granular portion and/or the extra-granular portion of a tablet comprising obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, can affect the properties of the tablet.
- tablets of moderate hardness when microcrystalline cellulose is added to only the intra-granular portion of the tablet, tablets of tolerable hardness may be produced.
- addition of microcrystalline cellulose to both the intra-granular and extra-granular portions can provide tablets having superior tablet hardness and an improved dissolution profile.
- microcrystalline cellulose is added to the intra-granular portion of the tablet.
- microcrystalline cellulose is added to both the intra-granular portion and extra-granular portion of the tablet.
- microcrystalline cellulose When the microcrystalline cellulose is present in the intra-granular portion it can be present in a ratio of microcrystalline cellulose to obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, between about 20: 1 to about 1 :5. In one embodiment, the ratio of microcrystalline cellulose to obeticholic acid, or a
- pharmaceutically acceptable salt, ester, or amino acid conjugate thereof may be, e.g., between about 19:1 to about 1 :5, between about 19: 1 to about 1 :4, between about 19: 1 to about 1 :3, between about 19: 1 to about 1 :2, between about 18: 1 to about 1 :5, between about 18:1 to about 1 :4, between about 18:1 to about 1 :3, between about 18:1 to about 1 :2, between about 17:1 to about 1:5, between about 17:1 to about 1:4, between about 17:1 to about 1:3, between about 17:1 to about 1:2, between about 16:1 to about 1:5, between about 16:1 to about 1:4, between about 16:1 to about 1:3, between about 16:1 to about 1:2, between about 15:1 to about 1:5, between about 15:1 to about 1:4, between about 15:1 to about 1:3, between about 15:1 to about 1:2, between about 14:1 to about 1:5, between about 14:1 to about 1:4, between about 14:1 to
- the ratio of microcrystalline cellulose to obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is between about 10:1 to about 1 :5, between about 10:1 to about 1 :4, between about 10:1 to about 1 :3, or between about 10:1 to about 1:2.
- the ratio of microcrystalline cellulose to obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is between about 9:1 to about 1:4, between about 9:1 to about 1:3, between about 9:1 to about 1:2, or between about 9:1 to about 1:1.
- the ratio of microcrystalline cellulose to obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is between about 8:1 to about 1 :3, between about 8:1 to about 1:2, or between about 8:1 to about 1:1.
- the ratio of microcrystalline cellulose to obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is between about 7:1 to about 1:2 or between about 7:1 to about 1:1.
- the ratio of microcrystalline cellulose to obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is between about 6: 1 to about 1:1.
- the ratio of microcrystalline cellulose to obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is between about 20:1 to about 1:1, between about 19:1 to about 1:1, between about 18:1 to about 1:1, between about 17:1 to about 1:1, between about 16:1 to about 1:1, between about 15:1 to about 1:1, between about 14:1 to about 1:1, between about 13:1 to about 1:1, between about 12: 1 to about 1 : 1 , or between about 11:1 to about 1:1.
- the ratio of microcrystalline cellulose to obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is between about 20:1 to about 2:1, between about 20:1 to about 3:1, between about 20: 1 to about 4:1, between about 20: 1 to about 5:1, between about 20:1 to about 6:1, between about 20:1 to about 7:1, between about 20:1 to about 8:1, between about 20:1 to about 9: 1, between about 20:1 to about 10:1, between about 20:1 to about 11 : 1, between about 19:1 to about 2:1, between about 19:1 to about 3:1, between about 19:1 to about 4:1, between about 19:1 to about 5:1, between about 19:1 to about 6:1, between about 19:1 to about 7:1, between about 19:1 to about 8:1, between about 19:1 to about 9:1, between about 19:1 to about 10:1, between about 19:1 to about 11 : 1, between about 18: 1 to about 2: 1, between about 18:1 to about 3:1, between
- the ratio of microcrystalline cellulose to obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof may be between about 20: 1 to about 5 : 1, between about 16: 1 to about 6:1 , or between about 16: 1 to about 11 :1 , or any of the above-mentioned ratio ranges between about 20:1 to about 5 : 1.
- the ratio of microcrystalline cellulose to obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is about 16: 1.
- the ratio of microcrystalline cellulose to obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is about 11 : 1.
- the ratio of microcrystalline cellulose to obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is about 6: 1. In yet another embodiment, the ratio of microcrystalline cellulose to obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, is between about 10: 1 to about 1 : 1. In another embodiment, the ratio of microcrystalline cellulose to obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, is between about 5: 1 to about 1 : 1. In yet another embodiment, the ratio of microcrystalline cellulose to obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, is between about 3: 1 to about 1 : 1.
- the ratio of microcrystalline cellulose to obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is between about 2: 1 to about 1 :1. In another embodiment, the ratio of microcrystalline cellulose to obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, is between about 4: 1 to about 2: 1. In yet another embodiment, the ratio of microcrystalline cellulose to obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, is between about 3:1 to about 2: 1. In another embodiment, the ratio of microcrystalline cellulose to obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, is about 4: 1.
- the ratio of microcrystalline cellulose to obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is about 3: 1. In yet another embodiment, the ratio of microcrystalline cellulose to obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, is about 2:1. In another embodiment, the ratio of microcrystalline cellulose to obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, is about 1 : 1.
- the tablet hardness of an obeticholic acid containing tablet can be between about 6 kilopascals (kP) to about 14 kP. In one embodiment, the tablet hardness is between about 7 kP to about 12 kP. In another embodiment, the tablet hardness is between about 8 kP to about 12 kP. In yet another, the tablet hardness is between about 8 kP to about 11 kP. In another embodiment, the tablet hardness is between about 9 kP to about 11 kP. In yet another embodiment, the tablet hardness is between about 10 kP to about 11 kP.
- the tablets of the present disclosure comprising obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, microcrystalline cellulose and optionally one or more additional pharmaceutical excipients in the intra-granular portion, and one or more pharmaceutical excipients in the extra-granular portion possess increased hardness.
- the tablets of the present disclosure comprising obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, microcrystalline cellulose and optionally one or more additional pharmaceutical excipients in the intra-granular portion, and microcrystalline cellulose and optionally one or more additional pharmaceutical excipients in the extra-granular portion possess increased hardness.
- the tablets of the present disclosure comprising microcrystalline cellulose in both the intra-granular portion and extra-granular portion possess increased hardness, for example, as compared with tablets comprising
- the hardness is increased at least about 5%, at least about 10%, at least about 20%, at least about 30%, at least about 40%, at least about 50%, at least about 60%, or at least about 70%, for example, as compared with tablets comprising microcrystalline cellulose in only the intra-granular portion. In one embodiment, the hardness is increased at least about 20%, at least about 30%, at least about 40%, or at least about 50%, for example, as compared with tablets comprising microcrystalline cellulose in only the intra-granular portion.
- the hardness is increased between about 5% and about 45%, between about 10% and about 40%, between about 15% and about 35%, between about 20% and about 30%, between about 25% and about 35%, between about 25% and about 40%, between about 25% and about 50%, or between about 30% and about 50%, for example, as compared with tablets comprising microcrystalline cellulose in only the intra-granular portion.
- the tablets of the present disclosure comprising obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, microcrystalline cellulose and optionally one or more additional pharmaceutical excipients in the intra-granular portion, and one or more pharmaceutical excipients in the extra-granular portion possess increased hardness.
- the tablets of the present disclosure comprising obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, microcrystalline cellulose, and optionally one or more additional pharmaceutical excipients in the intra-granular portion, and microcrystalline cellulose and optionally one or more additional pharmaceutical excipients in the extra-granular portion possess improved dissolution of obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof.
- the tablets of the present disclosure comprising microcrystalline cellulose in both the intra-granular portion and extra-granular portion possess improved dissolution of obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, for example, as compared with tablets comprising microcrystalline cellulose in only the intra-granular portion.
- obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof in the tablets of the present disclosure dissolves (e.g.
- Disodium Hydrogen Phosphate Buffer in a Disodium Hydrogen Phosphate Buffer at a rate that is at least 2%, 3%, 4%, 5%, 6%, 7%, 8%, 9%, 10%, 15%, 20%, 30%, 40%, 50%, 80%, or 100% faster than, for example, as compared with the dissolution rate tablets comprising microcrystalline cellulose in only the intra-granular portion.
- obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof in the tablet of the present disclosure is dissolved within about 15 minutes, or about 65% to about 95% is dissolved within about 30 minutes, or about 80% to about 95% is dissolved within about 45 minutes, or about 87% to about 97% is dissolved within about 60 minutes, or about 87% to about 99% is dissolved within about 75 minutes.
- obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof in the tablet of the present disclosure is dissolved within about 15 minutes, or about 75% to about 91 % is dissolved within about 30 minutes, or about 85% to about 93% is dissolved within about 45 minutes, or about 90% to about 96% is dissolved within about 60 minutes, or about 90% to about 97% is dissolved within about 75 minutes.
- obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof in the tablet of the present disclosure is dissolved within about 15 minutes, or about 80% to about 90% is dissolved within about 30 minutes, or about 87% to about 94% is dissolved within about 45 minutes, or about 92% to about 96% is dissolved within about 60 minutes, or about 91 % to about 97% is dissolved within about 75 minutes.
- obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof in the tablet of the present disclosure is dissolved within about 15 minutes, or about 70% to about 90% is dissolved within about 30 minutes, or about 85% to about 92% is dissolved within about 45 minutes, or about 89% to about 96% is dissolved within about 60 minutes, or about 90% to about 96% is dissolved within about 75 minutes.
- at least about 60% obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof in the tablet of the present disclosure is dissolved within about 15 minutes, or at least about 90% is dissolved within about 60 minutes.
- obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof in the tablet of the present disclosure has an in vitro dissolution profile of about 51 % dissolved within about 15 minutes, or about 66% dissolved within about 30 minutes, or about 79% dissolved within about 45 minutes, or about 85% dissolved within about 60 minutes.
- Obeticholic acid tablets can be manufactured via a manufacturing process comprising dry granulation by roller compaction followed by tablet compression and coating.
- the process steps used to manufacture OCA tablets include: pre-blending, dry granulation, final blending, compression, coating, and packaging.
- Obeticholic acid drug substance and one or more pharmaceutical excipients are added and further optionally blended to produce a premix.
- OCA and microcrystalline cellulose is blended to produce a premix.
- the premix is blended, passed through a screen and then again blended.
- the one or more pharmaceutical excipients are added in small portions and blended between each addition.
- the one or more pharmaceutical excipients are added sequentially.
- the one or more pharmaceutical excipients are added together.
- the premix is then granulated and optionally milled to reduce particle size.
- the premix is roller compacted.
- the premix is further milled.
- the premix can be milled using various methods.
- the premix is milled using a comil.
- the premix is milled using a comil followed by an oscillating bar screen mill.
- a final blending of the obeticholic acid tablet formulation is performed.
- one or more pharmaceutical excipients i. e. , microcrystalline cellulose, sodium starch glycolate, and/or magnesium stearate
- microcrystalline cellulose is added during the final blending.
- the one or more pharmaceutical excipients are added sequentially. In another embodiment, the one or more pharmaceutical excipients are added together.
- the final blend is then compressed to form the tablet.
- the compression parameters can be adjusted to produce tablets of the desired weight, hardness, thickness, and friability.
- the tablet press speed and feeder speed can also be adjusted to help reduce tablet weight variation.
- the obeticholic acid tablets are then coated with a coating material (i.e. , Opadry® II white, Opadry® II green, or Opadry® II yellow) using a coating solution.
- Obeticholic acid compositions described herein can be administered in accordance with a dosing regimen.
- a dosing regimen refers to continual and intermittent administration of a obeticholic acid composition described herein at one or more of the amounts described herein.
- a dosing regimen can include administration of a obeticholic acid composition described herein continually for any number of days, weeks, months, or years as set forth herein.
- a dosing regimen can include administration of a obeticholic acid composition described herein intermittently, where, for example, the composition is administered for one period of time followed by a rest period or off period where the obeticholic acid composition is not administered.
- Obeticholic acid compositions useful in the methods of treating described herein include administration of such compositions daily (QD), every other day (Q2D), once a week (QW), twice a week (BID), three times a week (TIW), once a month (QM), or twice a month (Q2M).
- a obeticholic acid composition described herein is administered QD.
- an effective amount of an obeticholic acid composition described herein can be administered QD to treat a disease or condition described herein.
- a starting dose described herein can be administered QD during the course of a titration period described herein to treat a disease or condition described herein.
- An adjusted dose described herein can be administered QD to treat a disease or condition described herein.
- an obeticholic acid composition described herein is administered Q2D.
- An effective amount of an obeticholic acid composition described herein can be administered Q2D to treat a disease or condition described herein.
- a starting dose described herein can be administered Q2D during the course of a titration period described herein to treat a disease or condition described herein.
- An adjusted dose described herein can be administered Q2D to treat a disease or condition described herein.
- an obeticholic acid composition is described herein administered QW.
- An effective amount of an obeticholic acid composition described herein can be administered QW to treat a disease or condition described herein.
- a starting dose described herein can be administered QW during the course of a titration period described herein to treat a disease or condition described herein.
- An adjusted dose described herein can be administered QW to treat a disease or condition described herein.
- an obeticholic acid composition is described herein administered BID.
- An effective amount of an obeticholic acid composition described herein can be administered BID to treat a disease or condition described herein.
- a starting dose described herein can be administered BID during the course of a titration period described herein to treat a disease or condition described herein.
- An adjusted dose described herein can be administered BID to treat a disease or condition described herein.
- an obeticholic acid composition is described herein administered TIW.
- An effective amount of an obeticholic acid composition described herein can be administered TIW to treat a disease or condition described herein.
- a starting dose described herein can be administered TIW during the course of a titration period described herein to treat a disease or condition described herein.
- An adjusted dose described herein can be administered TIW to treat a disease or condition described herein.
- an obeticholic acid composition is described herein administered QM.
- An effective amount of an obeticholic acid composition described herein can be administered QM to treat a disease or condition described herein.
- a starting dose described herein can be administered QM during the course of a titration period described herein to treat a disease or condition described herein.
- An adjusted dose described herein can be administered QM to treat a disease or condition described herein.
- an obeticholic acid composition is described herein administered Q2M.
- An effective amount of an obeticholic acid composition described herein can be administered Q2M to treat a disease or condition described herein.
- a starting dose described herein can be administered Q2M during the course of a titration period described herein to treat a disease or condition described herein.
- An adjusted dose described herein can be administered Q2M to treat a disease or condition described herein.
- the embodiments described above include administration at an amount described above.
- an obeticholic acid composition described herein can be administered in a frequency provided above in an amount of 5 mg, 10 mg, 25 mg, or 50 mg.
- Dosing regimens of the obeticholic acid compositions described herein useful for treating diseases and conditions described herein can include a titration period.
- a titration period typically includes a lower dosage of an obeticholic acid composition described herein for a period of time.
- administration using a titration period described herein can decrease or eliminate the onset of adverse effects.
- administration using a titration period described herein can permit increased dosages of obeticholic acid compositions described herein to an individual over the course of a treatment.
- a titration period can be a period of time of about: 1 month to about 24 months; 1 month to about 21 months; 1 month to about 18 months; 1 month to about 15 months; 1 month to about 12 months; 1 month to about 9 months; 1 month to about 6 months; or 1 month to about 3 months.
- a titration period includes a time of about: 3 months to about 24 months; 3 months to about 21 months; 3 months to about 18 months; 3 months to about 15 months; 3 months to about 12 months; 3 or months to about 6 months.
- a titration period includes a time of about: 6 months to about 24 months; 6 months to about 21 months; 6 months to about 18 months; 6 months to about 15 months; or 6 months to about 12 months.
- a titration period includes a time of about: 2 months to about 4 months; 2 months to about 7 months; 2 months to about 8 months; 4 months to about 8 months; 5 months to about 7 months; or 5 months to about 8 months.
- a titration period can be about 1 to about 6 months.
- a titration period can be about 3 to about 6 months.
- a titration period can include a time of about 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, or 24 months.
- a titration period includes a time of about 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, or 12 months.
- the titration period includes a time of about 1 , 2, 3, 4, 5, 6, 7, 8, or 9 months.
- the titration period includes a time of about 1, 2, 3, 4, 5, or 6 months.
- the titration period includes a time of about 1, 2, or 3 months.
- a titration period can be about 1 month.
- a titration period can be about 2 months.
- a titration period can be about 3 months. In still another example a titration period can be about 4 months. In yet another example a titration period can be about 5 months. In another example a titration period can be about 6 months. In one example a titration period is 3 months or 6 months. In another example a titration period can be about 7 months. In another example a titration period can be about 8 months. In another example a titration period can be about 9 months.
- the amounts of a obeticholic acid composition described herein, optionally administered in a titration period can be reduced compared to an adjusted amount as described herein.
- treatment regimens that include administering obeticholic acid compositions described herein for the treatment of a disease or condition described herein (e.g., PBC) wherein the starting dose administered during a titration period described above is lower than the amount of an adjusted dose administered after a titration period.
- treatment regimens that include administering obeticholic acid compositions described herein for the treatment of a disease or condition described herein (e.g., PBC) where the starting dose administered during a titration period described above is lower than the amount of an adjusted dose administered after a titration period and where the frequency of administration (e.g. , QD, Q2D, or QW) for the adjusted dose is greater than the frequency of administration of the starting dose.
- treatment regimens that include administering obeticholic acid compositions described herein for the treatment of a disease or condition described herein (e.g.
- the starting dose administered during a titration period described above is lower than the amount of an adjusted dose administered after a titration period and where the frequency of administration (e.g. , QD, Q2D, or QW) for the adjusted dose is less than the frequency of administration of the starting dose.
- Increases in the adjusted dose (or any readjusted dose) can be performed after the patient's liver function is assessed, monitored, or measured as described herein, where the liver function is considered not-impaired.
- the adjusted dose can be increased compared to the starting dose when the level of ALP is about equal to or is not reduced compared to a control as described herein. In embodiments, the adjusted can be increased compared to the starting dose when the level of bilirubin is about equal to or is not reduced compared to a control as described herein. In embodiments, the adjusted dose can be increased compared to the starting dose when the level of ALP and bilirubin are about equal to or are not reduced compared to a control as described herein. In certain instances, the adjusted dose can be increased compared to the starting dose where a patient described herein tolerates the starting dose amount. In certain embodiments, the starting dose can be 5 mg. In certain embodiments, the starting dose is 10 mg. In certain embodiments, the starting dose is 5 mg and the adjusted dose is greater than 5 mg (e.g. , about 6 mg to about 50 mg). In one embodiment, the starting dose is 5 mg and the adjusted dose is 10 mg.
- treatment regimens that include administering obeticholic acid compositions described herein for the treatment of a disease or condition described herein (e.g. , PBC) where the starting dose administered during a titration period described above is equal to the amount of an adjusted dose administered after a titration period.
- treatment regimens that include administering obeticholic acid compositions described herein for the treatment of a disease or condition described herein (e.g.
- treatment regimens that include administering obeticholic acid compositions described herein for the treatment of a disease or condition described herein (e.g. PBC) where the starting dose administered during a titration period described above is equal to the amount of an adjusted dose administered after a titration period and where the frequency of administration (e.g., QD, Q2D, or QW) for the adjusted dose is greater than the frequency of administration of the starting dose.
- obeticholic acid compositions described herein for the treatment of a disease or condition described herein e.g. PBC
- the starting dose administered during a titration period described above is equal to the amount of an adjusted dose administered after a titration period and where the frequency of administration (e.g. , QD, Q2D, or QW) for the adjusted dose is greater than the frequency of administration of the starting dose.
- treatment regimens that include administering obeticholic acid compositions described herein for the treatment of a disease or condition described herein (e.g. , PBC) where the starting dose administered during a titration period described above is equal to the amount of an adjusted dose administered after a titration period and where the frequency of administration (e.g. , QD, Q2D, or QW) for the adjusted dose is less than the frequency of administration of the starting dose.
- the adjusted dose (or any re-adjusted dose) can be equal to the starting dose where the patient's liver function is assessed, monitored, or measured as described herein, where the liver function is considered not-impaired.
- the adjusted dose can be equal to the starting dose when the level of ALP is reduced compared to a control as described herein. In embodiments, the adjusted dose can be equal to the starting dose when the level of bilirubin is reduced compared to a control as described herein. In embodiments, the adjusted dose can be equal to the starting dose when the level of ALP and bilirubin are reduced compared to a control as described herein. In certain instances, the adjusted dose can be equal to the starting dose where a patient described herein tolerates or poorly tolerates (e.g. , has onset of adverse effects described herein) the starting dose amount. In certain embodiments, the starting dose can be 5 mg. In certain embodiments, the starting dose is 10 mg. In certain embodiments, the starting dose is 5 mg and the adjusted dose is 5 mg. In one embodiment, the starting dose is 10 mg and the adjusted dose is 10 mg.
- treatment regimens that optionally include a starting dose and an adjusted dose as provided in the regimens above, where the adjusted dose is further reduced during the course of treatment.
- the adjusted dose is reduced to a new re-adjusted dose having a decreased amount of an obeticholic acid composition described herein.
- the adjusted dose is reduced to a new re- adjusted dose having the same amount of an obeticholic acid composition described herein but a decreased frequency of administration (e.g. , from QD to Q2D or QW).
- the adjusted dose is modified such that the re-adjusted dose includes a decreased amount of an obeticholic acid composition described herein and is administered at a decreased frequency compared to the adjusted dose.
- the obeticholic acid composition described herein can be administered for any number of days, weeks, months, or years, including indefinitely, provided that the dosage remains efficacious for the patient and the patient tolerates the dosage (e.g., an adjusted or readjusted dose as described herein).
- an obeticholic acid composition described herein is administered to a patient described herein until loss of efficacy, or until development of unacceptable toxicity or undesired adverse effects, such as, for example, those described herein.
- Daily dosing of an obeticholic acid composition described herein can be dependent upon patient tolerance to the dosage, composition, or frequency of
- daily dosing can be administered to a patient described herein where the patient tolerates a daily dosage amount (e.g. , 5 mg, 10 mg, 25 mg, or 50 mg).
- the daily dosing can be modified to increase or reduce the amount of an obeticholic acid composition described herein as provided above where the patient is tolerant or is intolerant to the dose, respectively.
- modification of the adjusted dose can be performed after the patient's liver function is assessed, monitored, or measured as described herein.
- the adjusted dose (or re-adjusted dose) is increased or maintained (e.g., equivalent to a starting dose) where the liver function is not-impaired.
- the adjusted dose (or re-adjusted dose) is decreased or maintained (e.g., equivalent to a starting dose) where the patient's liver function is impaired.
- the amount of an obeticholic acid described herein administered to a patient described herein can be modified as a result of intolerability or development of one or more adverse effects such as those described herein.
- the amount of an obeticholic acid composition described herein administered to a patient can be changed from a QD dosage to a Q2D dosage.
- the dosage of an obeticholic acid described herein is modified from a QD to Q2D dosage upon development of an adverse effect described herein (e.g. , severe pruritus).
- administration of an obeticholic acid composition described herein at 5 mg QD can be modified to a 5 mg Q2D dosage.
- Such a modification can reduce or eliminate undesired adverse effects while maintaining the desired efficacy.
- administration of an obeticholic acid composition described herein at 10 mg QD can be reduced to 5 mg QD.
- exemplary dosing regimens described herein can be combined.
- a reduced dosage of an obeticholic acid composition described herein from 10 mg to 5 mg QD could be further reduced to a 5 mg Q2D dosage where undesired adverse effects remain.
- dosing of the obeticholic acid composition can be temporarily suspended (e.g., an off period) for about 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, or 14 days, or 1, 2, 3, or 4 weeks.
- a PBC patient is administered an obeticholic acid composition described herein where: the starting dose of the obeticholic acid composition described herein is administered QD to a patient described herein at an amount of 5 mg and the obeticholic acid composition is administered QD to the patient in an adjusted dose of 5 mg.
- the exemplary dosing regimen can include a titration period of about 1 to about 6 months.
- a PBC patient is administered an obeticholic acid composition described herein where: the starting dose of the obeticholic acid composition described herein is administered QD to a patient described herein at an amount of 5 mg in a titration period of about 3 months or about 6 months and the obeticholic acid composition is administered QD to the patient in an adjusted dose of 5 mg.
- a PBC patient is administered an obeticholic acid composition described herein where: the starting dose of the obeticholic acid composition described herein is administered QD to a patient in a titration period of about 3 months or about 6 months and the obeticholic acid composition is administered QD to the patient in an adjusted dose of 10 mg.
- a PBC patient is administered an obeticholic acid composition described herein where: the starting dose of the obeticholic acid composition described herein is administered QD to a patient in a titration period of about 3 months or about 6 months and the obeticholic acid composition is administered QD to the patient in an adjusted dose of 5 mg, where the adjusted dose is modified to a 5 mg Q2D readjusted dose upon development of an adverse effect (e.g. , pruritus or severe pruritus).
- an adverse effect e.g. , pruritus or severe pruritus
- a PBC patient is administered a obeticholic acid composition described herein, where the starting dose of the obeticholic acid composition described herein is administered QD to a patient in a titration period of about 3 months or about 6 months and the obeticholic acid composition is administered QD to the patient in an adjusted dose of 10 mg, where the adjusted dose is subsequently modified to a 5 mg QD re-adjusted dose upon development of an adverse effect (e.g. , pruritus or severe pruritus).
- an adverse effect e.g. , pruritus or severe pruritus
- the amount of an obeticholic acid composition described herein administered to a patient can be determined by the existence of any preexisting conditions in the patient. For example, where a patient described herein has or has had hepatic impairment, the dosage of the obeticholic acid composition described herein can be modified. In certain instances, the hepatic impairment is a Child-Pugh Class B or Class C hepatic impairment. In one embodiment, the hepatic impairment is Child-Pugh Class C. In such instances, the amount of an obeticholic acid composition described herein can be administered in a decreased amount during and after a titration period when compared to administration of the same obeticholic acid composition to a patient who does not have hepatic impairment.
- a patient having hepatic impairment is administered an obeticholic acid composition described herein at an amount of about 1 mg to about 5 mg, where the composition is administered at least once weekly (QW).
- the obeticholic acid composition described herein is administered at an amount of about 5 mg once weekly to a patient diagnosed with hepatic impairment (e.g. , Child-Pugh Class B or C).
- the dosing regimen can include administering an obeticholic acid composition described herein to a patient having hepatic impairment, where the obeticholic acid composition is administered at a starting dose of 5 mg QW for a titration period of 3 or 6 months and administered at an adjusted dose of 5 mg QW.
- the patient's liver function can be assessed, monitored, or measured as described herein. Where the patient's liver function is not impaired, the adjusted dose can be increased to a re-adjusted dose of 5 mg administered BIW or 5 mg QD.
- a patient can develop liver impairment during the course of administration. It is understood, using the disclosure provided herein, that the adjusted dose can be decreased in amount or frequency to avoid progression of liver impairment.
- the patient tolerance, liver function, and/or lowered efficacy indicate end of a titration period and administration of an adjusted dose of 5 mg QD.
- an obeticholic acid composition described herein can be metabolized to a obeticholic acid conjugate, such as for example, a glycine, taurine, or sarcosine conjugate of obeticholic acid.
- a obeticholic acid conjugate such as for example, a glycine, taurine, or sarcosine conjugate of obeticholic acid.
- Such metabolites can be useful in treating a disease or condition provided herein.
- production of conjugates can be assessed, monitored, measured, or detected, as described herein during the course of a treatment.
- increased levels of obeticholic acid conjugates can result in adjusted dosages of an obeticholic acid composition described herein.
- ursodeoxycholic acid is commonly used as a parenteral advant.
- UDCA ursodeoxycholic acid
- the obeticholic acid compositions described herein can be administered as described herein (e.g. , according to one or more dosing regimens provided above) in combination with UDCA.
- the UDCA is administered at an amount of about 10 to 15 mg/kg/day.
- the UDCA is administered at an amount of about 300, 600, 900, or 1200 mg/day.
- Administration of UDCA can include a rest or off period of 1 , 2, 3, or 4 weeks.
- an obeticholic acid composition described herein is administered as described herein in combination with UDCA, where the UDCA is administered at an amount provided above or in accordance with a package insert.
- package insert refers to instructions customarily included in commercial packages of medicaments approved by the FDA or a similar regulatory agency of a country other than the USA, which contains information about, for example, the usage, dosage, administration, contraindications, and/or warnings concerning the use of such medicaments.
- the active agent is a peroxisome proliferator-activated receptor alpha (PPARa) agonist, a peroxisome proliferator-activated receptor delta (PPAR5) agonist, a dual PPARa/ ⁇ agonist, a dual PPARa/ ⁇ agonist, or pan-PPAR agonist, an HMG CoA reductase inhibitor, a GLP1 agonist, insulin, insulin mimetic, metformin, a GTP4 agonist, an HST2 inhibitor, a DPP-IV inhibitor, an SGLT2 inhibitor or a hydroxysteroid dehydrogenase (HSD) inhibitor, such as an ⁇ ⁇ ⁇ -HSDl inhibitor, an ASK1 inhibitor, an ACC1 inhibitor, a NOXl and/or NOX4 inhibitor, an inhibitor or antagonist of one or more chemokine receptors, such as, for example, CCR2 and CCR5.
- PPARa peroxisome proliferator-activated receptor alpha
- PPAR5 peroxisome
- compositions described herein can be co-administered with one or more cancer agents.
- the anti-cancer agent useful in methods of treating solid-tumor cancers provided herein can include any known class of anti-cancer agents such as, for example, radiation therapy, operations, alkylating agents, antimetabolites, anthracyclines, campothecins, vinca alkaloids, taxanes or platinums, as well as other antineoplastic agents known in the art.
- anti-cancer agent and antineoplastic agent classifications are known in the art and used in accordance with their plain and ordinary meaning.
- anti-cancer agents include but are not limited to: ABRAXANE;
- abiraterone ace-11 ; aclarubicin; acivicin; acodazole hydrochloride; acronine; actinomycin; acylfulvene; adecypenol; adozelesin; adriamycin; aldesleukin; all trans-retinoic acid (ATRA); altretamine; ambamustine; ambomycin; ametantrone acetate; amidox; amifostine;
- aminoglutethimide aminolevulinic acid; amrubicin; amsacrine; anagrelide; anastrozole; andrographolide; antarelix; anthramycin; aphidicolin glycinate; apurinic acid; ara-CDP-DL-
- PTBA arginine deaminase
- ARRY-162 ARRY-300
- ARRY-142266 ARRY-142266
- AS703026 AS703026
- axinastatin 2 axinastatin 3 ; azasetron; azatoxin; azatyrosine; azacitidine; AZD8330; azetepa; azotomycin; balanol; batimastat; BAY 11-7082; BAY 43-9006; BAY 869766; bendamustine; benzochlorins; benzodepa; benzoylstaurosporine; beta-alethine; betaclamycin B; betulinic acid; b-FGF inhibitor; bicalutamide; bisantrene; bisaziridinylspermine; bisnafide; bisnafide dimesylate; bistratene A; bisantrene hydrochloride; bleomycin; bleomycin sulfate; busulfan; bizelesin; breflate; bortezomib; brequinar sodium; bropirimine; budotitan
- CARN 700 caracemide; carbetimer; carboplatin; carmustine; carubicin hydrochloride;
- chloroquinoxaline sulfonamide cicaprost; chlorambucil; Chlorofusin; cirolemycin; cisplatin;
- CI-1040 cis-porphyrin; cladribine; clomifene analogues; clotrimazole; collismycin A;
- collismycin B combretastatin A4; combretastatin analogue; conagenin; crambescidin 816; crisnatol; crisnatol mesylate; cryptophycin 8; cryptophycin A derivatives; curacin A;
- cyclopentanthraquinones cycloplatam; cypemycin; cyclophosphamide; cytarabine;
- cytarabine ocfosfate; cytolytic factor; cytostatin; dacarbazine; dactinomycin; daunorubicin; daunorubicin hydrochloride; decarbazine; dacliximab; dasatinib; decitabine;
- dehydrodidemnin B deslorelin; dexamethasone; dexifosfamide; dexrazoxane; dexverapamil; dexormaplatin; dezaguanine; dezaguanine mesylate; diaziquone; didemnin B; didox;
- diethylnorspermine dihydro 5 azacytidine; dihydrotaxol; 9-dioxamycin; diphenyl spiromustine; docosanol; dolasetron; docetaxel; doxorubicin; doxorubicin hydrochloride; doxifluridine; droloxifene; droloxifene citrate; dromostanolone propionate; dronabinol;
- duazomycin duocarmycin SA; ebselen; ecomustine; edelfosine; edrecolomab; edatrexate; eflornithine hydrochloride; eflornithine; elemene; emitefur; elsamitrucin; enloplatin;
- eribulin esorubicin hydrochloride
- estramustine estramustine phosphate sodium
- etanidazole etoposide; etoposide phosphate; etoprine; exemestane; fadrozole; fadrozole hydrochloride; trasrabine; fenretinide; filgrastim; finasteride; flavopiridol; flezelastine; fluasterone; floxuridine; fludarabine phosphate; fludarabine; fluorodaunorubicin
- hydrochloride forfenimex; formestane; fluorouracil; floxouridine; flurocitabine; fosquidone; fostriecin sodium; fostriecin; fotemustine; gadolinium texaphyrin; gallium nitrate;
- BBI 201 iobenguane; iododoxorubicin; ipomeanol; irinotecan; irinotecan hydrochloride; irsogladine; isobengazole; isohomohalicondrin B; itasetron; iimofosine; interleukin IL-2 (including recombinant interleukin II; or rlL.sub.2); interferon alfa-2a; interferon alfa-2b; interferon alfa-nl ; interferon alfa-n3; interferon beta- l a; interferon gamma- lb;
- jasplakinolide kahalalide F; lamellarin N triacetate; lanreotide; leinamycin; lenograstim; lentinan sulfate; leptolstatin; letrozole; leuprorelin; levamisole; lenalidomide; lenvatinib; liarozole; lissoclinamide 7; lobaplatin; lombricine; lometrexol; lonidamine; losoxantrone; lovastatin; loxoribine; lurtotecan; lutetium texaphyrin; lysofylline; lanreotide acetate;
- miltefosine miltefosine; mirimostim; mitoguazone; mitolactol; mitonafide; mitoxantrone; mofarotene; molgramostim; mopidamol; mycaperoxide B; myriaporone; maytansine; mechlorethamine hydrochloride; megestrol acetate; melengestrol acetate; melphalan; mercaptopurine;
- methotrexate methotrexate sodium; metoprine; meturedepa; mitindomide; mitocarcin; mitocromin; mitogillin; mitomalcin; mitomycin; mitosper; mitotane; mitoxantrone hydrochloride; mycophenolic acid; nafarelin; nagrestip; napavin; naphterpin; nartograstim; nedaplatin; nemorubicin; neridronic acid; nilutamide; nisamycin; nitric oxide modulators; nitroxide antioxidant; nitrullyn; nocodazole; nogalamycin; oblimersen (GENASENSE); octreotide; okicenone; olaparib (LYNPARZA); oligonucleotides; onapristone; ondansetron; oracin; oral cytokine inducer; ormaplatin; oxisur
- PD318026 PD98059; peliomycin; pentamustine; peplomycin sulfate; PKC412; pipobroman; piposulfan; piroxantrone hydrochloride; plicamycin; plomestane; podophyllotoxin;
- polyphenol E polyphenol E; porfimer sodium; porfiromycin; prednimustine; procarbazine; procarbazine hydrochloride; puromycin; puromycin hydrochloride; pyrazofurin; raltitrexed; ramosetron; retelliptine demethylated; rhizoxin; rituximab; RII retinamide; rogletimide; rohitukine;
- romurtide roquinimex; rubiginone Bl ; ruboxyl; riboprine; romidepsin; rucaparib; safingol; safingol hydrochloride; saintopin; sarcophytol A; sargramostim; semustine; sizofiran;
- sobuzoxane sodium borocaptate; sodium phenylacetate; solverol; sonermin; sorafenib;
- sunitinib sparfosic acid
- spicamycin D spiromustine
- splenopentin spongistatin 1 ;
- Spongistatin 2 Spongistatin 3; Spongistatin 4; Spongistatin 5; Spongistatin 6; Spongistatin 7;
- Spongistatin 8 and Spongistatin 9; squalamine; stipiamide; stromelysin inhibitors;
- tauromustine tauromustine; tazarotene; tecogalan sodium; tegafur; tellurapyrylium; temoporfin; temozolomide; teniposide; tetrachlorodecaoxide; tetrazomine; thaliblastine; thiocoraline; thrombopoietin; thymalfasin; thymopoietin receptor agonist; thymotrinan; tirapazamine; titanocene bichloride; topsentin; toremifene; tretinoin; triacetyluridine; triciribine;
- Erbulozole e.g., R-55104
- Dolastatin 10 e.g. , DLS-10 and NSC-376128
- Mivobulin isethionate e.g. , CI-980
- NSC-639829 e.g.
- NVP-XX-A-296 NVP-XX-A-296
- ABT-751 Abbott; e.g., E-7010
- Altorhyrtin A Altorhyrtin C
- Cemadotin hydrochloride e.g., LU-103793 and NSC-D-669356
- CEP 9722 Epothilone A; Epothilone B; Epothilone C; Epothilone D; Epothilone E; Epothilone F;
- LS-4577 LS-4578
- LS-4578 Pulsacia; e.g., LS-477- P
- LS-4477 Pulsacia
- LS-4559 Pulsacia
- RPR-112378 Aventis
- DZ-3358 Disiichi
- FR-182877 Frisawa; e.g., WS-9265B
- GS-164 Takeda
- GS-198 Takeda
- KAR-2 Hungarian Academy of Sciences
- BSF-223651 BASF; e.g.
- AVE-8063A and CS-39.HC1 AC-7700 (Ajinomoto; e.g., AVE-8062; AVE-8062A; CS-39-L-Ser.HCl; and RPR-258062A);
- DDE-261 and WHI-261 H10 (Kansas State University); H16 (Kansas State University); Oncocidin Al (e.g., BTO-9
- D-62638 Asta Medica
- D-62636 Asta Medica
- Myoseverin B D-43411 (Zentaris; e.g. , D-81862)
- A-289099 Abbott
- A-318315 Abbott
- HTI-286 e.g.
- a method for treating patients with colorectal cancer by administering an obeticholic acid composition described herein in combination with capecitabine and/or PLX4032 (Plexxikon).
- colorectal cancer (optionally refractory) by administering an obeticholic acid composition described herein in combination with capecitabine, xeloda, and/or CPT-11.
- colorectal cancer (optionally refractory) by administering an obeticholic acid composition described herein in combination with capecitabine, xeloda, and/or CPT-11.
- [00293] in another aspect is a method for treating patients with unresectable or metastatic hepatocellular carcinoma by administering an obeticholic acid composition described herein in combination with interferon alpha or capecitabin.
- Patients described herein include a patients having a disease or condition described herein.
- a patient can be described or referred to by the condition treated.
- a patient having PBC can be referred to herein as a PBC patient.
- a patient described herein can have a preexisting condition (e.g., a condition other than the disease or condition treated by the obeticholic acid composition described herein that existed at the time of first administration).
- a patient described herein has hepatic impairment.
- a patient described herein has renal impairment.
- the patient is an elderly/geriatric patient or a pregnant patient.
- the patient is an pediatric patient.
- administration of an obeticholic acid composition described herein together with certain contra-active agents can result in (1) decreased efficacy of the obeticholic acid composition and/or (2) development of toxicity or adverse effects described herein.
- administration of an obeticholic acid composition described herein with blood clotting and anti-coagulation agents can result in decreased International Normalized Ratio (INR).
- INR International Normalized Ratio
- coagulation and anti-coagulation agents can be administered in combination with an obeticholic acid composition described herein by monitoring fluctuations of the INR of the patient and adjusting dosages as understood in the art to maintain proper INR.
- an obeticholic acid composition described herein in combination with a bile acid binding resin can result in decreased efficacy of the obeticholic acid composition at a lower dosage of the composition (e.g., 1 to 5 mg).
- a bile acid binding resin is administered in combination with an obeticholic acid composition described herein at least about 4 to 6 hours before or after the dosage of the obeticholic acid composition.
- compositions described herein reduce adverse effects associated with other formulations (e.g. , larger particle sized obeticholic acid).
- an obeticholic acid composition described herein when administered to a patient described herein for a condition or disease described herein can reduce one or more adverse effects selected from Hepatic encephalopathy, ascites, variceal bleeding, skin eruptions, prurigo, pruritus (including generalized, eye, anal, vulvovaginal and rash), fatigue, asthenia, abdominal pain (including upper and lower pain and tenderness), abdominal discomfort, gastrointestinal pain, dizziness, urticaria (including cholinergic), rashes (including macular, popular, maculo-papular, and heat rashes), arthralgia, oropharyngeal pain, cough, constipation, edemal peripheral, palpitations, pyrexia, eczema, and procedural pain.
- the one or more adverse effects that are reduced include pruritus. It was discovered, inter alia, that titration of an obeticholic acid composition described herein can reduce the incidence of or mean time until onset of severe pruritus. [00299] In another embodiment, the obeticholic acid compositions described herein include reduced levels of impurities commonly found in the synthesis of obeticholic acid.
- 6 ⁇ - ethylursodeoxycholic acid (6-EUDCA), 3 ⁇ -hydroxy-6 ⁇ -ethyl-7-keto-5 ⁇ -cholan-24-oic acid, 6 -ethylchenodeoxycholic acid; 3 ⁇ ,7 ⁇ -dihydroxy- 6 ⁇ -ethyl-5 ⁇ -cholan-24-oic acid, 3 ⁇ ,7 ⁇ - dihydroxy-6-ethyliden-5 -cholan-24-oic acid, Chenodeoxycholic acid (CDCA); 3 ⁇ ,7 ⁇ - dihydroxy-5 ⁇ -cholan-24-oic acid, Dimer of OCA, 3 ⁇ -(3 ⁇ ,7 ⁇ -dihydroxy-6 ⁇ -ethyl-5 ⁇ -cholan- 24-oyloxy)-7 ⁇ -hydroxy-6 ⁇ -ethyl-5 ⁇ -cholan-24-oic acid, or 3 ⁇ -0-Acetyl-6 ⁇ - ethyl chenodeoxycholic acid; 3 ⁇ -0-acetyl-7 ⁇ -hydroxy-6 ⁇ -ethyl-5 ⁇ -
- Embodiment 1 A method of treating primary biliary cirrhosis (PBC) in a patient in need thereof, the method comprising administering a composition comprising obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, wherein obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is in the form of particles, and wherein at least 50% of the particles have a diameter of 200 ⁇ or less.
- PBC primary biliary cirrhosis
- Embodiment 2 A method of treating primary sclerosing cholangitis (PSC), chronic liver disease, nonalcoholic fatty liver disease (NAFLD), nonalcoholic steatohepatitis (NASH), hepatitis C infection, alcoholic liver disease, liver damage due to progressive fibrosis, or liver fibrosis in a patient in need thereof, the method comprising administering a composition comprising obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, wherein obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is in the form of particles, and wherein at least 50% of the particles have a diameter of 200 ⁇ or less.
- Embodiment 3 The method of embodiment 2, wherein the method comprises treating NASH.
- Embodiment 4 A method of treating a solid-tumor cancer in a patient in need thereof, the method comprising administering an effective amount of a composition comprising obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, wherein obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is in the form of particles, and wherein at least 50% of the particles have a diameter of 200 ⁇ m or less.
- Embodiment 5 The method of embodiment 1 , 2 or 4, wherein the effective amount comprises a starting dose.
- Embodiment 6 The method of embodiment 5, wherein the starting dose is administered in a titration period.
- Embodiment 7 The method of any one of embodiments 4 to 6, wherein the cancer comprises hepatocellular carcinoma (HCC), colorectal cancer, gastric cancer, liver cancer, kidney cancer, or pancreatic cancer.
- Embodiment 8 A method of treating an autoimmune disease in a patient in need thereof, the method comprising administering an effective amount of a composition comprising obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, wherein obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is in the form of particles, and wherein at least 50% of the particles have a diameter of 200 ⁇ m or less.
- HCC hepatocellular carcinoma
- Embodiment 8 A method of treating an autoimmune disease in a patient in need thereof, the method comprising administering an effective amount of a composition comprising obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, wherein obeticholic acid or a pharmaceutical
- Embodiment 9 The method of embodiment 7, wherein the effective amount comprises a starting dose.
- Embodiment 10 The method of embodiment 8, wherein the starting dose is administered in a titration period.
- Embodiment 1 1 The method of embodiment 7 or 8, wherein the autoimmune disease is selected from the group consisting of: PBC, multiple sclerosis, rheumatoid arthritis, and type-I diabetes.
- Embodiment 12 The method of any one of embodiments 1 -2, 6 or 9, wherein the titration period comprises 1 to 6 months.
- Embodiment 13 The method of embodiment 11, wherein the titration period is 3 months.
- Embodiment 14 The method of embodiment 11, wherein the titration period is 6 months.
- Embodiment 15 The method of any one of embodiments 12 to 15, wherein the starting dose is administered to the patient once daily.
- Embodiment 16 The method of any one of embodiments 11 to 14, wherein the starting dose is administered to the patient once daily.
- Embodiment 17 The method of any one of embodiments 11 to 14, wherein the starting dose is administered to the patient once weekly.
- Embodiment 18 The method of any one of embodiments 11 to 14, wherein the starting dose is administered to the patient once every other day.
- Embodiment 19 The method of any one of embodiments 11 to 17, wherein the starting dose comprises about 1 mg to 50 mg.
- Embodiment 20 The method of any one of embodiments 11 to 17, wherein the starting dose comprises about 1 mg to 25 mg.
- Embodiment 21 The method of any one of embodiments 11 to 17, wherein the starting dose comprises about 1 mg to 10 mg.
- Embodiment 22 The method of any one of embodiments 11 to 17, wherein the starting dose comprises about 1 mg to 5 mg.
- Embodiment 23 The method of any one of embodiments 11 to 17, wherein the starting dose comprises about 5 mg.
- Embodiment 24 The method of any one of embodiments 11 to 17, wherein the starting dose comprises about 10 mg.
- Embodiment 25 The method of any one of embodiments 11 to 17, wherein the starting dose comprises about 25 mg.
- Embodiment 26 The method of any one of embodiments 11 to 17, wherein the starting dose comprises about 50 mg.
- Embodiment 27 The method of any one of embodiments 1 to 26, further comprising assessing or monitoring liver function before, during, or after the titration period.
- Embodiment 28 The method of embodiment 27, wherein the assessing or monitoring comprises measuring a level of one or more liver biomarkers compared to a control.
- Embodiment 29 The method of embodiment 28, wherein the liver biomarker is selected from the group consisting of: AST, ALT, alkaline phosphatase (ALP), bilirubin, glycine conjugated obeticholic acid, taurine conjugated obeticholic acid, a bile acid, a bile acid glycine conjugate, or a bile acid taurine conjugate.
- the liver biomarker is selected from the group consisting of: AST, ALT, alkaline phosphatase (ALP), bilirubin, glycine conjugated obeticholic acid, taurine conjugated obeticholic acid, a bile acid, a bile acid glycine conjugate, or a bile acid taurine conjugate.
- Embodiment 30 The method of embodiment 29, comprising detecting a level of ALP in the patient.
- Embodiment 31 The method of embodiment 29 or 30, comprising detecting a level of bilirubin in the patient.
- Embodiment 32 The method of any one of embodiments 27 to 31, further comprising calculating a AST to platelet ratio (APR! for the patient.
- APR AST to platelet ratio
- Embodiment 33 The method of any one of embodiments 12 to 32, wherein the obeticholic acid composition is administered to the patient as an adjusted dose after the titration period.
- Embodiment 34 The method of embodiment 33, wherein the adjusted dose is equal to the titrated dose.
- Embodiment 35 The method of embodiment 33, wherein the adjusted dose is equal to the starting dose when the level of ALP is reduced compared to a control.
- Embodiment 36 The method of embodiment 33, wherein the adjusted dose is greater than the titrated dose.
- Embodiment 37 The method of any one of embodiments 33 to 36, wherein the adjusted dose is administered more frequently than the titrated dose.
- Embodiment 38 The method of any one of embodiments 33 to 36, wherein the adjusted dose is administered less frequently than the titrated dose.
- Embodiment 39 The method of any one of embodiments 33 to 38, wherein the adjusted dose of the obeticholic acid composition is administered to the patient once daily.
- Embodiment 40 The method of any one of embodiments 33 to 38, wherein the adjusted dose of the obeticholic acid composition is administered to the patient once daily.
- Embodiment 41 The method of any one of embodiments 33 to 38, wherein the adjusted dose of the obeticholic acid composition is administered to the patient once daily.
- Embodiment 42 The method of any one of embodiments 33 to 38, wherein the adjusted dose of the obeticholic acid composition is administered to the patient once weekly.
- Embodiment 43 The method of any one of embodiments 33 to 38, wherein the adjusted dose of the obeticholic acid composition is administered to the patient once every other day.
- Embodiment 44 The method of any one of embodiments 33 to 38, wherein the adjusted dose of the obeticholic acid composition is administered to the patient twice a week.
- Embodiment 45 The method of any one of embodiments 33 to 44, wherein the adjusted dose comprises about 1 mg to 50 mg.
- Embodiment 46 The method of any one of embodiments 33 to 44, wherein the adjusted dose comprises about 1 mg to 25 mg.
- Embodiment 47 The method of any one of embodiments 33 to 44, wherein the adjusted dose comprises about 1 mg to 10 mg.
- Embodiment 48 The method of any one of embodiments 33 to 44, wherein the adjusted dose comprises about 1 mg to 5 mg.
- Embodiment 49 The method of any one of embodiments 33 to 44, wherein the adjusted dose comprises about 5 mg.
- Embodiment 50 The method of any one of embodiments 33 to 44, wherein the adjusted dose comprises about 10 mg.
- Embodiment 51 The method of any one of embodiments 33 to 44, wherein the adjusted dose comprises about 25 mg.
- Embodiment 52 The method of any one of embodiments 33 to 44, wherein the adjusted dose comprises about 50 mg.
- Embodiment 53 The method of any one of embodiments 1 to 52, wherein the method further comprises administering one or more active agents, or combinations thereof.
- Embodiment 54 The method of embodiment 53, wherein the active agent is ursodeoxycholic acid (UDCA).
- UDCA ursodeoxycholic acid
- Embodiment 55 The method of embodiment 53, wherein the active agent is a peroxisome proliferator-activated receptor alpha (PPARa) agonist, a peroxisome proliferator- activated receptor delta (PPAR5) agonist, a dual PPARa/ ⁇ agonist, a dual PPARa/ ⁇ agonist, or pan-PPAR agonist, an HMG Co A reductase inhibitor, a GLP1 agonist, insulin, insulin mimetic, metformin, a GTP4 agonist, an HST2 inhibitor, a DPP-IV inhibitor, an SGLT2 inhibitor or a hydroxysteroid dehydrogenase (HSD) inhibitor, such as an ⁇ ⁇ -HSDl inhibitor, an ASK1 inhibitor, an ACC1 inhibitor, a NOXl and/or NOX4 inhibitor, an inhibitor or antagonist of one or more chemokine receptors, such as, for example, CCR2 and CCR5.
- PPARa peroxisome proliferator-activated receptor
- Embodiment 56 The method of any one of embodiments 1 to 55, wherein the obeticholic acid composition is administered as a first line therapy for the treatment of PBC.
- Embodiment 57 The method of any one of embodiments 1 to 56, wherein the patient is has renal impairment or hepatic impairment.
- Embodiment 58 A method for treating primary biliary cirrhosis (PBC) in a patient in need thereof, the method comprising:
- obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof
- a starting dose of a composition comprising obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, in a titration period, wherein obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is in the form of particles, and wherein at least 50% of the particles have a diameter of 200 um or less;
- APR AST to platelet ratio
- liver biomarker selected from ALP, bilirubin, AST, ALT, glycine conjugated obeticholic acid, taurine conjugated obeticholic acid, a bile acid, a bile acid glycine conjugate, or a bile acid taurine conjugate;
- a reduced APR! score compared to a control or a reduced level of the one or more liver biomarkers compared to a control indicates non-impaired liver function
- Embodiment 59 The method of embodiment 58, wherein the adjusted dose is administered at an amount equal to an amount of the starting dose.
- Embodiment 60 The method of embodiment 58, wherein the adjusted dose is administered at an amount greater than an amount of the starting dose.
- Embodiment 61 The method of embodiment 58, wherein the adjusted dose of the obeticholic acid composition is administered at the same frequency as the starting dose.
- Embodiment 62 The method of embodiment 58, wherein the adjusted dose of the obeticholic acid composition is administered at a decreased frequency than the starting dose.
- Embodiment 63 The method of embodiment 58, wherein the effective amount of the obeticholic acid composition is administered at an increased frequency than the starting dose.
- Embodiment 64 The method of any one of embodiments 58 to 63, wherein the starting dose is 5 mg.
- Embodiment 65 The method of any one of embodiments 58 to 64, wherein the starting dose is administered QD.
- Embodiment 66 The method of any one of embodiments 58 to 64, wherein the adjusted dose is 5 mg.
- Embodiment 67 The method of any one of embodiments 58 to 64, wherein the adjusted dose is 10 mg.
- Embodiment 68 The method of any one of embodiments 58 to 67, wherein the adjusted dose is administered QD or Q2D.
- Embodiment 69 The method of any one of embodiments 58 to 68, further comprising assessing the patient for tolerance to the adjusted dose.
- Embodiment 70 The method of embodiment 69, wherein the adjusted dose is modified to a re-adjusted dose when the patient.
- Embodiment 71 The method of embodiment 70, wherein the re-adjusted dose comprises an equal amount compared to the adjusted dose and administration at a reduced frequency.
- Embodiment 72 The method of embodiment 71 , wherein the re-adjusted dose comprises a reduced amount compared to the adjusted dose and administration at an equal frequency.
- Embodiment 73 The method of embodiment 58, wherein the patient has hepatic impairment.
- Embodiment 74 The method of embodiment 73, wherein the starting dose is administered QW.
- Embodiment 75 The method of embodiment 74, wherein the starting dose is 5 mg.
- Embodiment 75 The method of any one of embodiments 58 to 75, wherein the adjusted dose is equivalent to the starting dose when the level of ALP is reduced compared to a control.
- Embodiment 76 The method of any one of embodiments 58 to 75, wherein the adjusted dose comprises an amount equal to the starting dose and wherein the adjusted dose is administered at a greater frequency than the starting dose.
- Embodiment 77 A composition comprising obeticholic acid, or a
- obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is in the form of particles, and wherein at least 50% of the particles have a diameter of 200 ⁇ or less, for use in treating primary biliary cirrhosis (PBC) in a patient in need thereof.
- PBC primary biliary cirrhosis
- Embodiment 78 A composition comprising obeticholic acid, or a
- obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is in the form of particles, and wherein at least 50% of the particles have a diameter of 200 ⁇ or less, for use in treating primary biliary cirrhosis (PBC) in a patient in need thereof.
- PBC primary biliary cirrhosis
- Embodiment 79 A composition comprising obeticholic acid, or a
- obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is in the form of particles, and wherein at least 50% of the particles have a diameter of 200 ⁇ or less, for use in treating primary sclerosing cholangitis (PSC), chronic liver disease, nonalcoholic fatty liver disease (NAFLD), nonalcoholic steatohepatitis (NASH), hepatitis C infection, alcoholic liver disease, liver damage due to progressive fibrosis, or liver fibrosis in a patient in need thereof in a patient in need thereof.
- PSC primary sclerosing cholangitis
- NAFLD nonalcoholic fatty liver disease
- NASH nonalcoholic steatohepatitis
- hepatitis C infection alcoholic liver disease
- liver damage due to progressive fibrosis or liver fibrosis in a patient in need thereof in a patient in need thereof.
- Embodiment 80 The composition of embodiment 79, for use in treating NASH.
- Embodiment 81 A composition comprising obeticholic acid, or a
- obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is in the form of particles, and wherein at least 50% of the particles have a diameter of 200 ⁇ or less, for use in treating a solid-tumor cancer in a patient in need thereof.
- Embodiment 82 The composition of embodiments 77, 79 or 81, wherein said composition further comprises said obeticholic acid composition as a starting dose.
- Embodiment 83 The composition of embodiment 82, wherein said starting dose is prepared to be administered in a titration period.
- Embodiment 84 The composition of any one of embodiments 81 to 83, for use in treating hepatocellular carcinoma (HCC), colorectal cancer, gastric cancer, liver cancer, kidney cancer, or pancreatic cancer.
- HCC hepatocellular carcinoma
- colorectal cancer gastric cancer
- liver cancer liver cancer
- kidney cancer or pancreatic cancer.
- Embodiment 85 A composition comprising obeticholic acid, or a
- obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is in the form of particles, and wherein at least 50% of the particles have a diameter of 200 ⁇ or less, for use in treating an autoimmune disease in a patient in need thereof.
- Embodiment 86 The composition of embodiment 85, wherein said composition further comprises said obeticholic acid composition as a starting dose.
- Embodiment 87 The composition of embodiment 86, wherein said starting dose is prepared to be administered in a titration period.
- Embodiment 88 The composition of embodiment 85 or 86, for use in treating multiple sclerosis, rheumatoid arthritis, or type-I diabetes.
- Embodiment 89 The composition of any one of embodiments 78-79, 83 or 87, wherein said titration period comprises 1 to 6 months.
- Embodiment 90 The composition of embodiment 89, wherein said titration period is 3 months.
- Embodiment 91 The composition of embodiment 89, wherein said titration period is 6 months.
- Embodiment 92 The composition of any one of embodiments 89 to 91, wherein said starting dose is prepared to be administered to said patient once daily.
- Embodiment 93 The composition of any one of embodiments 89 to 92, wherein said starting dose is prepared to be administered to said patient once daily.
- Embodiment 94 The composition of any one of embodiments 89 to 92, wherein said starting dose is prepared to be administered to said patient once weekly.
- Embodiment 95 The composition of any one of embodiments 89 to 92, wherein said starting dose is prepared to be administered to said patient once every other day.
- Embodiment 96 The composition of any one of embodiments 89 to 95, wherein said starting dose comprises about 1 mg to 50 mg.
- Embodiment 97 The composition of any one of embodiments 89 to 95, wherein said starting dose comprises about 1 mg to 25 mg.
- Embodiment 98 The composition of any one of embodiments 89 to 95, wherein said starting dose comprises about 1 mg to 10 mg.
- Embodiment 99 The composition of any one of embodiments 89 to 95, wherein said starting dose comprises about 1 mg to 5 mg.
- Embodiment 100 The composition of any one of embodiments 89 to 95, wherein said starting dose comprises about 5 mg.
- Embodiment 101 The composition of any one of embodiments 89 to 95, wherein said starting dose comprises about 10 mg.
- Embodiment 102 The composition of any one of embodiments 89 to 95, wherein said starting dose comprises about 25 mg.
- Embodiment 103 The composition of any one of embodiments 89 to 95, wherein said starting dose comprises about 50 mg.
- Embodiment 104 The composition of any one of embodiments 78 to 103, wherein said patient liver function assessed or monitored before, during, or after said titration period.
- Embodiment 105 The composition of embodiment 104, wherein said assessing or monitoring comprises measuring a level of one or more liver biomarkers compared to a control.
- Embodiment 106 The composition of embodiment 105, wherein said liver biomarker is selected from the group consisting of: AST, ALT, alkaline phosphatase (ALP), bilirubin, glycine conjugated obeticholic acid, taurine conjugated obeticholic acid, a bile acid, a bile acid glycine conjugate, or a bile acid taurine conjugate.
- said liver biomarker is selected from the group consisting of: AST, ALT, alkaline phosphatase (ALP), bilirubin, glycine conjugated obeticholic acid, taurine conjugated obeticholic acid, a bile acid, a bile acid glycine conjugate, or a bile acid taurine conjugate.
- Embodiment 107 The composition of embodiment 106, wherein said liver biomarker is ALP.
- Embodiment 108 The composition of embodiment 106 or 107, wherein said liver biomarker is bilirubin.
- Embodiment 109 The composition of any one of embodiments 104 to 108, further comprising calculating an AST to platelet ratio (APR! for said patient.
- APR AST to platelet ratio
- Embodiment 1 10. The composition of any one of embodiments 89 to 109, wherein said obeticholic acid composition is prepared to be administered to said patient as an adjusted dose after said titration period.
- Embodiment 1 11. The composition of embodiment 110, wherein said adjusted dose is equal to said titrated dose.
- Embodiment 1 12. The composition of embodiment 110, wherein said adjusted dose is equal to said starting dose when a level of ALP is reduced compared to a control.
- Embodiment 1 13 The composition of embodiment 110, wherein said adjusted dose is greater than said titrated dose.
- Embodiment 1 14. The composition of any one of embodiments 110 to 113, wherein said adjusted dose is prepared to be administered more frequently than said titrated dose.
- Embodiment 1 15. The composition of any one of embodiments 110 to 113, wherein said adjusted dose is prepared to be administered less frequently than said titrated dose. [00418] Embodiment 1 16. The composition of any one of embodiments 110 to 115, wherein said adjusted dose of said obeticholic acid composition is prepared to be administered to said patient once daily.
- Embodiment 1 17. The composition of any one of embodiments 110 to 115, wherein said adjusted dose of said obeticholic acid composition is prepared to be administered to said patient once daily.
- Embodiment 1 18. The composition of any one of embodiments 110 to 115, wherein said adjusted dose of said obeticholic acid composition is prepared to be administered to said patient once daily.
- Embodiment 1 19. The composition of any one of embodiments 110 to 115, wherein said adjusted dose of said obeticholic acid composition is prepared to be administered to said patient once weekly.
- Embodiment 120 The composition of any one of embodiments 110 to 115, wherein said adjusted dose of said obeticholic acid composition is prepared to be administered to said patient once every other day.
- Embodiment 121 The composition of any one of embodiments 110 to 115, wherein said adjusted dose of said obeticholic acid composition is prepared to be administered to said patient twice a week.
- Embodiment 122 The composition of any one of embodiments 110 to 121 , wherein said adjusted dose comprises about 1 mg to 50 mg.
- Embodiment 123 The composition of any one of embodiments 110 to 121 , wherein said adjusted dose comprises about 1 mg to 25 mg.
- Embodiment 124 The composition of any one of embodiments 110 to 121 , wherein said adjusted dose comprises about 1 mg to 10 mg.
- Embodiment 125 The composition of any one of embodiments 110 to 121 , wherein said adjusted dose comprises about 1 mg to 5 mg.
- Embodiment 126 The composition of any one of embodiments 110 to 121 , wherein said adjusted dose comprises about 5 mg.
- Embodiment 127 The composition of any one of embodiments 110 to 121 , wherein said adjusted dose comprises about 10 mg.
- Embodiment 128 The composition of any one of embodiments 110 to 121 , wherein said adjusted dose comprises about 25 mg.
- Embodiment 129 The composition of any one of embodiments 110 to 121 , wherein said adjusted dose comprises about 50 mg.
- Embodiment 130 The composition of any one of embodiments 78 to 129, wherein said obeticholic acid composition is prepared to be co-administered one or more active agents, or combinations thereof.
- Embodiment 131 The composition of embodiment 130, wherein said active agent is ursodeoxycholic acid (UDCA).
- UDCA ursodeoxycholic acid
- Embodiment 132 The composition of embodiment 130, wherein the active agent is a peroxisome proliferator-activated receptor alpha (PPARa) agonist, a peroxisome proliferator-activated receptor delta (PPAR5) agonist, a dual PPARa/ ⁇ agonist, a dual PPARa/ ⁇ agonist, or pan-PPAR agonist, an HMG CoA reductase inhibitor, a GLP1 agonist, insulin, insulin mimetic, metformin, a GTP4 agonist, an HST2 inhibitor, a DPP-IV inhibitor, an SGLT2 inhibitor or a hydroxysteroid dehydrogenase (HSD) inhibitor, such as an 11 ⁇ - HSD1 inhibitor, an ASK1 inhibitor, an ACC1 inhibitor, a NOXl and/or NOX4 inhibitor, an inhibitor or antagonist of one or more chemokine receptors, such as, for example, CCR2 and CCR5.
- PPARa peroxisome proliferator-activated receptor
- Embodiment 133 The composition of any one of embodiments 78 to 132, wherein said obeticholic acid composition is prepared to be administered as a first line therapy for the treatment of PBC.
- Embodiment 134 The composition of any one of embodiments 78 to 133, wherein said patient is has renal impairment or hepatic impairment.
- Embodiment 135. A composition comprising a starting dose of obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, wherein obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is in the form of particles, and wherein at least 50% of the particles have a diameter of 200 ⁇ or less for use in treating primary biliary cirrhosis (PBC) in a patient in need thereof wherein the composition is prepared to be administered in a titration period wherein
- PBC primary biliary cirrhosis
- the liver function of the patient is assessed before, during, and after said titration period by calculating an AST to platelet ratio (APR! score for said patient or by measuring the level of one or more liver biomarker selected from ALP, bilirubin, AST, ALT, glycine conjugated obeticholic acid, taurine conjugated obeticholic acid, a bile acid, a bile acid glycine conjugate, or a bile acid taurine conjugate, wherein a reduced APR! score compared to a control or a reduced level of said one or more liver biomarkers compared to a control indicates non-impaired liver function; and
- the tolerance of the patient to said starting dose is assessed by grading the severity of one or more adverse effects, if present; and the obeticholic acid composition is prepared to be administered as an adjusted dose, wherein said adjusted dose comprises an amount equal to or greater than an amount of said starting dose.
- Embodiment 136 The composition of embodiment 135, wherein said adjusted dose is prepared to be administered at an amount equal to an amount of said starting dose.
- Embodiment 137 The composition of embodiment 135, wherein said adjusted dose is prepared to be administered at an amount greater than an amount of said starting dose.
- Embodiment 138 The composition of embodiment 135, wherein said adjusted dose of said obeticholic acid composition is prepared to be administered at the same frequency as said starting dose.
- Embodiment 139 The composition of embodiment 135, wherein said adjusted dose of said obeticholic acid composition is prepared to be administered at a decreased frequency than said starting dose.
- Embodiment 140 The composition of embodiment 135, wherein said effective amount of said obeticholic acid composition is prepared to be administered at an increased frequency than said starting dose.
- Embodiment 141 The composition of any one of embodiments 135 to 140, wherein said starting dose is 5 mg.
- Embodiment 142 The composition of any one of embodiments 135 to 141 , wherein said starting dose is prepared to be administered QD.
- Embodiment 143 The composition of any one of embodiments 135 to 141 , wherein said adjusted dose is 5 mg.
- Embodiment 144 The composition of any one of embodiments 135 to 141 , wherein said adjusted dose is 10 mg.
- Embodiment 145 The composition of any one of embodiments 135 to 144, wherein said adjusted dose is prepared to be administered QD or Q2D.
- Embodiment 146 The composition of any one of embodiments 135 to 145, wherein said patient is assessed for tolerance to said adjusted dose.
- Embodiment 147 The composition of embodiment 146, wherein said adjusted dose is modified to a re-adjusted dose.
- Embodiment 148 The composition of embodiment 147, wherein said re-adjusted dose comprises an equal amount compared to said adjusted dose and is prepared to be administrated at a reduced frequency.
- Embodiment 149 The composition of embodiment 148, wherein said re-adjusted dose comprises a reduced amount compared to said adjusted dose and is prepared to be administrated at an equal frequency.
- Embodiment 150 The composition of embodiment 135, wherein said patient has hepatic impairment.
- Embodiment 151 The composition of embodiment 150, wherein said starting dose is prepared to be administered QW.
- Embodiment 152 The composition of embodiment 151 , wherein said starting dose is 5 mg.
- Embodiment 153 The composition of any one of embodiments 135 to 152, wherein said adjusted dose is equivalent to said starting dose when said level of ALP is reduced compared to a control.
- Embodiment 154 The composition of any one of embodiments 135 to 152, wherein said adjusted dose comprises an amount equal to said starting dose and wherein said adjusted dose is prepared to be administered at a greater frequency than said starting dose.
- Embodiment 155 Use of a composition comprising obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, wherein obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is in the form of particles, and wherein at least 50% of the particles have a diameter of 200 ⁇ or less, for the manufacture of a medicament for use in treating primary biliary cirrhosis (PBC) in a patient in need thereof.
- PBC primary biliary cirrhosis
- compositions comprising obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, wherein obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is in the form of particles, and wherein at least 50% of the particles have a diameter of 200 ⁇ or less, for the manufacture of a medicament for use in treating primary sclerosing cholangitis (PSC), chronic liver disease, nonalcoholic fatty liver disease (NAFLD), nonalcoholic steatohepatitis (NASH), hepatitis C infection, alcoholic liver disease, liver damage due to progressive fibrosis, or liver fibrosis in a patient in need thereof in a patient in need thereof.
- PSC primary sclerosing cholangitis
- NAFLD nonalcoholic fatty liver disease
- NASH nonalcoholic steatohepatitis
- hepatitis C infection alcoholic liver disease, liver damage due to progressive fibrosis, or liver fibrosis in a patient
- Embodiment 157 The use of embodiment 156, for use in treating NASH.
- Embodiment 158 Use of a composition comprising obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, wherein obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is in the form of particles, and wherein at least 50% of the particles have a diameter of 200 ⁇ or less, for the manufacture of a medicament for use in treating a solid-tumor cancer in a patient in need thereof.
- Embodiment 159 The use of embodiments 155, 156 or 158, wherein said composition further comprises said obeticholic acid composition as a starting dose.
- Embodiment 160 The use of embodiment 159, wherein said starting dose is prepared to be administered in a titration period.
- Embodiment 161 The use of any one of embodiments 158 to 160, wherein said cancer is hepatocellular carcinoma (HCC), colorectal cancer, gastric cancer, liver cancer, kidney cancer, or pancreatic cancer.
- HCC hepatocellular carcinoma
- colorectal cancer gastric cancer
- liver cancer liver cancer
- kidney cancer or pancreatic cancer.
- Embodiment 162 Use of a composition comprising obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, wherein obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is in the form of particles, and wherein at least 50% of the particles have a diameter of 200 ⁇ or less, for the manufacture of a medicament for use in treating an autoimmune disease in a patient in need thereof.
- Embodiment 163 The use of embodiment 162, wherein said said obeticholic acid composition is prepared to be administered as a starting dose.
- Embodiment 164 The use of embodiment 163, wherein said starting dose is prepared to be administered in a titration period.
- Embodiment 165 The use of embodiment 162 or 163, wherein said autoimmune disease is multiple sclerosis, rheumatoid arthritis, or type-I diabetes.
- Embodiment 166 The use of any one of embodiments 155-156, 160 or 164, wherein said titration period comprises 1 to 6 months.
- Embodiment 167 The use of embodiment 166, wherein said titration period is 3 months.
- Embodiment 168 The use of embodiment 166, wherein said titration period is 6 months.
- Embodiment 169 The use of any one of embodiments 166 to 168, wherein said starting dose is prepared to be administered to said patient once daily.
- Embodiment 170 The use of any one of embodiments 166 to 169, wherein said starting dose is prepared to be administered to said patient once daily.
- Embodiment 171 The use of any one of embodiments 166 to 169, wherein said starting dose is prepared to be administered to said patient once weekly.
- Embodiment 172 The use of any one of embodiments 166 to 169, wherein said starting dose is prepared to be administered to said patient once every other day.
- Embodiment 173 The use of any one of embodiments 166 to 172, wherein said starting dose comprises about 1 mg to 50 mg.
- Embodiment 174 The use of any one of embodiments 166 to 172, wherein said starting dose comprises about 1 mg to 25 mg.
- Embodiment 175. The use of any one of embodiments 166 to 172, wherein said starting dose comprises about 1 mg to 10 mg.
- Embodiment 176 The use of any one of embodiments 166 to 172, wherein said starting dose comprises about 1 mg to 5 mg.
- Embodiment 177 The use of any one of embodiments 166 to 172, wherein said starting dose comprises about 5 mg.
- Embodiment 178 The use of any one of embodiments 166 to 172, wherein said starting dose comprises about 10 mg.
- Embodiment 179 The use of any one of embodiments 166 to 172, wherein said starting dose comprises about 25 mg.
- Embodiment 180 The use of any one of embodiments 166 to 172, wherein said starting dose comprises about 50 mg.
- Embodiment 18 The use of any one of embodiments 155 to 180, wherein liver function of said patient is assessed or monitored before, during, or after said titration period.
- Embodiment 182 The use of embodiment 181, wherein said assessing or monitoring comprises measuring a level of one or more liver biomarkers compared to a control.
- Embodiment 183 The use of embodiment 182, wherein said liver biomarker is selected from the group consisting of: AST, ALT, alkaline phosphatase (ALP), bilirubin, glycine conjugated obeticholic acid, taurine conjugated obeticholic acid, a bile acid, a bile acid glycine conjugate, or a bile acid taurine conjugate.
- said liver biomarker is selected from the group consisting of: AST, ALT, alkaline phosphatase (ALP), bilirubin, glycine conjugated obeticholic acid, taurine conjugated obeticholic acid, a bile acid, a bile acid glycine conjugate, or a bile acid taurine conjugate.
- Embodiment 184 The use of embodiment 183, wherein said liver biomarker is ALP.
- Embodiment 185 The use of embodiment 183 or 184, wherein said liver biomarker is bilirubin.
- Embodiment 186 The use of any one of embodiments 181 to 185, further comprising calculating an AST to platelet ratio (APR! for said patient.
- APR AST to platelet ratio
- Embodiment 187 The use of any one of embodiments 166 to 186, wherein said obeticholic acid composition is prepared to be administered to said patient as an adjusted dose after said titration period.
- Embodiment 188 The use of embodiment 187, wherein said adjusted dose is equal to said titrated dose.
- Embodiment 189 The use of embodiment 187, wherein said adjusted dose is equal to said starting dose when a level of ALP is reduced compared to a control.
- Embodiment 190 The use of embodiment 187, wherein said adjusted dose is greater than said titrated dose.
- Embodiment 191. The use of any one of embodiments 187 to 190, wherein said adjusted dose is prepared to be administered more frequently than said titrated dose.
- Embodiment 192 The use of any one of embodiments 187 to 190, wherein said adjusted dose is prepared to be administered less frequently than said titrated dose.
- Embodiment 193 The use of any one of embodiments 187 to 192, wherein said adjusted dose of said obeticholic acid composition is prepared to be administered to said patient once daily.
- Embodiment 194 The use of any one of embodiments 187 to 192, wherein said adjusted dose of said obeticholic acid composition is prepared to be administered to said patient once daily.
- Embodiment 195 The use of any one of embodiments 187 to 192, wherein said adjusted dose of said obeticholic acid composition is prepared to be administered to said patient once daily.
- Embodiment 196 The use of any one of embodiments 187 to 192, wherein said adjusted dose of said obeticholic acid composition is prepared to be administered to said patient once weekly.
- Embodiment 197 The use of any one of embodiments 187 to 192, wherein said adjusted dose of said obeticholic acid composition is prepared to be administered to said patient once every other day.
- Embodiment 198 The use of any one of embodiments 187 to 192, wherein said adjusted dose of said obeticholic acid composition is prepared to be administered to said patient twice a week.
- Embodiment 199 The use of any one of embodiments 187 to 198, wherein said adjusted dose comprises about 1 mg to 50 mg.
- Embodiment 200 The use of any one of embodiments 187 to 198, wherein said adjusted dose comprises about 1 mg to 25 mg.
- Embodiment 201 The use of any one of embodiments 187 to 198, wherein said adjusted dose comprises about 1 mg to 10 mg.
- Embodiment 202 The use of any one of embodiments 187 to 198, wherein said adjusted dose comprises about 1 mg to 5 mg.
- Embodiment 203 The use of any one of embodiments 187 to 198, wherein said adjusted dose comprises about 5 mg.
- Embodiment 204 The use of any one of embodiments 187 to 198, wherein said adjusted dose comprises about 10 mg.
- Embodiment 205 The use of any one of embodiments 187 to 198, wherein said adjusted dose comprises about 25 mg.
- Embodiment 206 The use of any one of embodiments 187 to 198, wherein said adjusted dose comprises about 50 mg.
- Embodiment 207 The use of any one of embodiments 155 to 206, wherein said obeticholic acid composition is prepared to be administered in combination with one or more active agents, or combinations thereof.
- Embodiment 208 The use of embodiment 207, wherein said active agent is ursodeoxycholic acid (UDCA).
- UDCA ursodeoxycholic acid
- Embodiment 209 The use of embodiment 207, wherein the active agent is a peroxisome proliferator-activated receptor alpha (PPARa) agonist, a peroxisome proliferator- activated receptor delta (PPAR5) agonist, a dual PPARa/ ⁇ agonist, a dual PPARa/ ⁇ agonist, or pan-PPAR agonist, an HMG Co A reductase inhibitor, a GLP1 agonist, insulin, insulin mimetic, metformin, a GTP4 agonist, an HST2 inhibitor, a DPP-IV inhibitor, an SGLT2 inhibitor or a hydroxysteroid dehydrogenase (HSD) inhibitor, such as an ⁇ ⁇ -HSDl inhibitor, an ASK1 inhibitor, an ACC1 inhibitor, a NOXl and/or NOX4 inhibitor, an inhibitor or antagonist of one or more chemokine receptors, such as, for example, CCR2 and CCR5.
- PPARa peroxisome proliferator-activ
- Embodiment 210 The use of any one of embodiments 155 to 209, wherein said obeticholic acid composition is prepared to be administered as a first line therapy for the treatment of PBC.
- Embodiment 211 The use of any one of embodiments 155 to 210, wherein said patient is has renal impairment or hepatic impairment.
- Embodiment 212 The use of a composition comprising a starting dose of obeticholic acid, or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof, wherein obeticholic acid or a pharmaceutically acceptable salt, ester, or amino acid conjugate thereof is in the form of particles, and wherein at least 50% of the particles have a diameter of 200 ⁇ or less for use in treating primary biliary cirrhosis (PBC) in a patient in need thereof wherein the composition is prepared to be administered in a titration period wherein:
- PBC primary biliary cirrhosis
- the liver function of the patient is assessed before, during, and after said titration period by calculating an AST to platelet ratio (APRI) score for said patient or by measuring the level of one or more liver biomarker selected from ALP, bilirubin, AST, ALT, glycine conjugated obeticholic acid, taurine conjugated obeticholic acid, a bile acid, a bile acid glycine conjugate, or a bile acid taurine conjugate, wherein a reduced APRI score compared to a control or a reduced level of said one or more liver biomarkers compared to a control indicates non-impaired liver function; and
- the tolerance of the patient to said starting dose is assessed by grading the severity of one or more adverse effects, if present; and the obeticholic acid composition is prepared to be administered as an adjusted dose, wherein said adjusted dose comprises an amount equal to or greater than an amount of said starting dose.
- Embodiment 213. The use of embodiment 212, wherein said adjusted dose is prepared to be administered at an amount equal to an amount of said starting dose.
- Embodiment 214 The use of embodiment 212, wherein said adjusted dose is prepared to be administered at an amount greater than an amount of said starting dose.
- Embodiment 215. The use of embodiment 212, wherein said adjusted dose of said obeticholic acid composition is prepared to be administered at the same frequency as said starting dose.
- Embodiment 216 The use of embodiment 212, wherein said adjusted dose of said obeticholic acid composition is prepared to be administered at a decreased frequency than said starting dose.
- Embodiment 217 The use of embodiment 212, wherein said effective amount of said obeticholic acid composition is prepared to be administered at an increased frequency than said starting dose.
- Embodiment 218 The use of any one of embodiments 212 to 217, wherein said starting dose is 5 mg.
- Embodiment 219. The use of any one of embodiments 212 to 218, wherein said starting dose is prepared to be administered QD.
- Embodiment 220 The use of any one of embodiments 212 to 218, wherein said adjusted dose is 5 mg.
- Embodiment 221. The use of any one of embodiments 212 to 218, wherein said adjusted dose is 10 mg.
- Embodiment 222 The use of any one of embodiments 212 to 221, wherein said adjusted dose is prepared to be administered QD or Q2D.
- Embodiment 223. The use of any one of embodiments 212 to 222, wherein said patient is assessed for tolerance to said adjusted dose.
- Embodiment 224 The use of embodiment 223, wherein said adjusted dose is modified to a re-adjusted dose.
- Embodiment 225 The use of embodiment 224, wherein said re-adjusted dose comprises an equal amount compared to said adjusted dose and is prepared to be
- Embodiment 226 The use of embodiment 225, wherein said re-adjusted dose comprises a reduced amount compared to said adjusted dose and is prepared to be administrated at an equal frequency.
- Embodiment 227 The use of embodiment 212, wherein said patient has hepatic impairment.
- Embodiment 228 The use of embodiment 227, wherein said starting dose is prepared to be administered QW.
- Embodiment 229. The use of embodiment 228, wherein said starting dose is 5 mg.
- Embodiment 230 The use of any one of embodiments 212 to 229, wherein said adjusted dose is equivalent to said starting dose when said level of ALP is reduced compared to a control.
- Embodiment 23 The use of any one of embodiments 212 to 229, wherein said adjusted dose comprises an amount equal to said starting dose and wherein said adjusted dose is prepared to be administered at a greater frequency than said starting dose.
- Particle size distribution was assessed using a dry dispersion method analyzed by laser diffraction using a Sympatec Laser Helos/KF-Magic F71000 with Rodos Dispersing Unit.
- the OCA sample 0.5 g sample was tested as a dry powder.
- the parameters for the validated particle size analysis method are described below:
- Apparatus Sympatec Laser Helos/KF-Magic F71000 with Rodos Dispersing Unit, Vibri sampling unit with Sniffer rotation, Nilfisk exhaustion or equivalent.
- Deionization apparatus Sartorius or equivalent.
- Feed rate 80%.
- Feed height 2 mm.
- Trigger conditions Time base: 100 ms; Start: Ka.28>l %; Stop: 1 s c.opt ⁇ l%.
- Jet milling studies were performed using a Hosokawa AFG 100 jet mill. The results showed a significant reduction in the particle size distribution (PSD). Jet milling was carried out with various classifier speeds to determine the optimum set of jet mill parameters.
- PSD particle size distribution
- Nozzle diameter/number 1.9 ⁇ x 3
- Rotor rotation speed 4000 rpm
- Current rating of motor 4.2 Amp
- TABLE 2 Particle size distribution of unmilled and jet milled obeticholic acid.
- Jet milling using spiral jet mill Jet milling studies were performed using a spiral jet mill. The results showed a significant reduction in the particle size distribution (PSD). Jet milling was carried out with various a range of parameters to determine the optimal settings. The jet mill parameters used in the spiral jet mill are provided below:
- Spiral jet mill parameters controlling the final PSD are:
- Feed rate Product amount fed into the milling chamber per unit time
- Pressure Fluid pressure through the nozzle section which influences the speed at which the particles collide
- FIG. 1 and FIG. 2 illustrate the typical particle size distribution of unmilled and jet-milled API, respectively.
- OCA obeticholic acid
- Microcrystalline cellulose was added to the intra-granular portion of the tablet mixture which produced tablets of moderate hardness. Modification to the manufacturing process to add microcrystalline cellulose to both the intra-granular and extra-granular portions of the tablet for both the 5 mg and 10 mg tablet generated more robust tablets (harder tablets). The compression challenges observed were overcome by redistributing a portion of microcrystalline cellulose in the 5 mg and 10 mg OCA formulation blends. This change in the manufacturing process impacted the quality attributes, specifically the dissolution profile, of the OCA tablets.
- OCA drug substance and excipients were added in specific quantities and order during pre- and final blending. Prior to manufacture, the materials were dispensed in the appropriate portions as shown in Table 6. Microcrystalline cellulose (MCC) and sodium starch glycolate (SSG) were sieved with a 1.0 mm aperture sieve before use. Magnesium stearate was sieved using a 0.5 mm aperture sieve immediately before use.
- MMC Microcrystalline cellulose
- SSG sodium starch glycolate
- MCC Microciystalline cellulose
- SSG Sodium starch glycolate
- a OCA drug substance amount assumes the drug substance content is 100%; actual amount added is adjusted for based on the potency of the drug substance lot used; the amount of microciystalline cellulose is correspondingly decreased.
- the amount of coating material prepared during the process is 150% of target. Excess coating material is discarded.
- Preblending Process To an appropriately sized blender drum was added OCA and a microciystalline cellulose (MCC) for premix (MCC-for-Premix: a portion of the total MCC added to the tablet formulation) to produce OCA premix. The resulting mixture was blended 90 to 120 revolutions (approximately for 3 minutes at a blender speed of about 30 rpm) and discharged. For the 5 mg tablets, OCA was pre-mixed with approximately 3 parts MCC (to 1 part OCA). For the 10 mg tablets, OCA was pre-mixed with approximately 2 parts MCC (to 1 part OCA).
- MCC microciystalline cellulose
- An appropriately sized bin was then charged with the following components: approximately 1 ⁇ 4 (one-fourth) of MCC-1, 1 ⁇ 2 (half) of OCA Premix, MCC drum rinse (MCC Rinse), 1 ⁇ 2 of OCA Premix, and 1 ⁇ 4 of MCC-1 in the order specified.
- the resulting mixture was then blended for 300 to 360 revolutions (about 20 minutes for 5 mg tablets, about 10 minutes for 10 mg tablets) in a Pharmatech MB400 drum blender or a Tumblemix drum blender or V- blender.
- the SSG-1 and the remaining 1 ⁇ 2 of MCC-1 was added to the bin and the mixture was then blended for 300 to 360 revolutions (about 10 to 20 minutes).
- Magnesium stearate-1 was then added to the bin via a 0.5 mm aperture sieve and the mixture was blended for 70 to 90 revolutions (about 3 minutes).
- silicon dioxide was added via a 0.5 mm aperture sieve together with SSG-1 and the remaining 1 ⁇ 2 of MCC-1 to the bin and the mixture was then blended for 300 to 360 revolutions (about 10 to 20 minutes).
- the blender revolutions for the various preblending steps provide homogeneity of the pre-blend formulation.
- the pre-blend was transferred from the bin blender to the roller compactor hopper.
- the pre-blend was roller compacted to provide flakes which were milled into granules through an in-line dual screen milling system.
- the granules were then collected in a suitable container.
- Roller compaction parameters used in the commercial production are shown in Table 7. This process provided the roller compacted active granules (intra-granular portion) for use in the final blending step.
- Roll pressure (compaction force), roll gap, and screen size (lower mill) are meaningful process parameters in the roller compaction process.
- the roll pressure, roll gap, and screen size provided granules with consistent physical characteristics and particle-size distribution.
- Tablet Coating The 5 mg and 10 mg OCA tablets were coated with a nonfunctional immediate release coating material. Tablet cores were coated with Opadry® II coating material using a perforated pan coater and a 48-inch pan. A 20% w/w coating solution was prepared by mixing Opadry® II with purified water. An excess of coating solution was prepared to ensure sufficient coating material is available for the coating process.
- pan rotation speed (about 12 rpm) was monitored and maintained in the appropriate range to ensure the tablet cores flowed consistently throughout the coating process.
- Pan speed is a meaningful process parameter, as this can affect tablet appearance (too high a pan speed can damage the tablets).
- Tablet bed temperature is a meaningful process parameter, as this can affect tablet water content and protects the tablets from over-wetting (which causes tablet appearance defects).
- Exhaust air temperature is linked to tablet bed temperature and is a meaningful process parameter if tablet bed temperature is not recorded.
- Packaging Tablets were packaged in the commercial primary packaging configuration using a standard automated bottling operation.
- the primary packaging configuration utilized a white high-density polyethylene bottle (40 cc) and child resistant cap with an induction seal.
- the commercial bottle will contain 30 OCA tablets. Tablet quantity, induction seal, cap torque, print quality, and appearance control testing was conducted at specific intervals throughout the packaging process. Induction sealing is a meaningful process parameter in the packaging process providing a completely sealed bottle.
- the in-process testing parameters for the packaging process is provided in Table 10 below.
- Tablet dissolution for both the 5 mg and 10 mg tablets was conducted in 900 mL of 50 mM Disodium Hydrogen Phosphate Buffer (Na 2 HP0 4 ), pH 6.8 at 37 °C using USP II paddle apparatus at a paddle speed of 75 rpm.
- Samples were assayed undiluted by filtering through a 0.2 ⁇ PVDF syringe filter using a gradient RP-HPLC method with CAD detection. This method utilized an Agilent Zorbax SB-C18 4.6 mm x 150 mm, 3.5 ⁇ HPLC column.
- a 50 sample was separated by a 20 minute gradient program, at a temperature of 40 °C and a flow rate of 1.5 mL per minute.
- TABLE 12 Parameters for the obeticholic acid 5 mg and 10 mg tablet dissolution method.
- HPLC high performance liquid chromatography
- rpm revolutions per minute
- USP United States
- Obeticholic acid was comilled with a 0.61 mm screen or jet-milled as described above to reduce the particle size of the material. Jet-milling (i.e., micronization) resulted in material that had a smaller, more uniform particle size and increased surface area, leading to faster drug release from tablets containing jet-milled OCA.
- the dissolution release rate of tablets containing comilled and jet-milled OCA is shown below in Table 13.
- Table 13 shows that reduction in particle size of the OCA drug product improves elution properties.
- the particle size distribution of the OCA impacted the drug dissolution rate, even in media where OCA is freely soluble (pH 6.8). It is therefore possible that differences in particle size could impact OCA bioavailability if dissolution becomes rate-limiting for absorption. For this reason, the particle size distribution of the active is considered a critical process parameter.
- Table 14 show the content uniformity data for tablets containing comilled and jet-milled OCA. Tablets containing comilled OCA showed a higher variability in content uniformity. The smaller particle size of the jet-milled material provides better content uniformity of the OCA tablets.
- Obeticholic acid and formulations of obeticholic acid were tested for stability.
- An unknown impurity at relative retention time (RRT) 1.75 was observed during stability studies of the tablets containing different batches of the 5 mg and 25 mg tablet formulation.
- the stability test using uncoated tablets showed an increase of a new impurity at about 0.05% with the test conducted at 25 °C, 60% RH for 4 weeks, and about 0.2% with the test conducted at 40°C, 75% RH for 4 weeks.
- a study was conducted to identify the structure of the impurity, clarify the origin for the generation of the impurity, and adopt measures to ensure that quality was not compromised during storage of the tablet.
- the structure of OCA and the identified structure of the impurity are respectively shown below:
- the impurity is an ethyl ester of obeticholic acid (OCA).
- OCA ethyl ester of obeticholic acid
- an authentic sample of the ethyl ester was synthesized by dissolving obeticholic acid in ethanol, adding concentrated sulfuric acid and heating the mixture.
- the retention time and mass spectrometry of the authentic sample matched those of the impurity and thus the structure of the impurity was confirmed as an ethyl ester of obeticholic acid (FIG. 7A and FIG. 7B). Comparison of the retention time and the mass spectrum of the ethy ester impurity and authentic sample is shown in FIG. 7A and FIG. 7B
- this impurity was an ester produced by a reaction between a PEG4000 hydroxyl group and the OCA carboxylic acid.
- the structure of OCA and PEG ester impurity are shown below:
- Example 6 Solubility Studies of OCA in Various Buffers and Biological Media.
- Dissolution media 50 mM sodium phosphate dibasic buffer, pH 6.8
- OCA drug substance was observed to precipitate out of solution in those acidic buffers in the pH range 1.2 to 3.0. Solutions at pH 4.1 to 6.0 also had some precipitation resulting in a cloudy solution. Solutions at pH 6.8 to 10 produced clear solutions. The recovery of OCA steadily diminishes at pH higher than 8.0, indicating basic decomposition of the drug substance.
- the nominal concentration for dissolved 5 mg and 10 mg tablets in the typical dissolution volume of 900 mL is approximately 0.006 & 0.01 mg/mL, respectively. Above pH 6.8 the solubility is well above 0.01 mg/mL, the minimum concentration required to dissolve a 5 mg or 10 mg tablet in 900 mL of dissolution medium (i.e. , sink conditions).
- solubility of OCA increases as a function of increasing pH, plateauing just above approximately pH 7.
- the dramatic increase in solubility observed between approximately pH 4 and pH 7 indicates that this pH region is less-than- ideal for use in the dissolution media.
- OCA is freely soluble at pH 6.8 and that this pH is physiologically relevant to the site of absorption, it was selected for use in diligent pursuit of a discriminating and relevant dissolution method.
- Solubility Studies of OCA in Biological Media A solubility study was performed in physiologically relevant dissolution media at 37°C and pH of 1.2, 4.5, and 6.8 along with fasted state simulated gastric fluid (FaSSGF, pH 1.2), fed state simulated intestinal fluid
- aFaSSGF is de-ionized water containing sodium taurocholate (80 ⁇ ) and NaCl (34.2 mM), pH 1.6.
- bFeSSIF is de-ionized water containing sodium taurocholate (15 mM) and lecithin (3.75 mM) with an osmolarity of
- TaSSIF is de-ionized water containing sodium taurocholate (3 mM) and lecithin (0.75 mM) with an osmolarity of 270 ⁇ 10 mOsmol, pH 6.5.
- e Surfactant is polysorbate 80 (Tween 80®)
- taurocholic acid and lecithin are typically present in the gastric and intestinal milieu.
- ursodeoxycholic acid UDCA
- colchicine methotrexate
- azathioprine or systemic corticosteroids
- HIV primary sclerosing cholangitis, alcoholic liver disease, definite autoimmune liver disease or biopsy proven nonalcoholic steatohepatitis (NASH).
- NASH nonalcoholic steatohepatitis
- the percent change (%) in serum ALP from Baseline to End of Study (EOS) was monitored.
- the baseline value was the mean of the pretreatment screening and day 0 evaluations.
- the EOS value was Day 85/ET or the last observed ALP value on treatment.
- Absolute changes in serum ALP levels were monitored from Baseline to Day 15, Day 29, Day 57, Day 85/ET and Follow-Up (Day 99). The percentage of patients was calculated who met the definition of PBC responder criteria applying the Paris I, Toronto I, Toronto II, Toronto III, Toronto IV, Mayo II, and Barcelona disease prognostic risk criteria at Day 85/ET. Each patient was tested for absolute and percent change in serum aspartate aminotransferase (AST), alanine aminotransferase (ALT), gamma-glutamyl transferase (GGT), and conjugated (direct) bilirubin values from Baseline to Day 15, Day 29, Day 57, Day 85/ET and Follow-Up (Day 99). Efficacy results are shown in Table 20 below.
- Table 20 Percent Change in ALP from Baseline - ITT population.
- GGT levels decreased, relative to placebo, at all-time points from day 15 to Day 85/ET in both the OCA 10 mg and OCA 50 mg groups.
- the mean (SD) GGT levels decreased from 653 (370) U/L at baseline to 184 (203) U/L at Day 85/ET in the OCA 10 mg group, and from 455 (418) U/L at baseline to 202 (300) U/L at day 85/ET in the OCA 50 mg group.
- Placebo GGT levels were 466 (321) U/L at Baseline and 502 (383) U/L at Day 85/ET.
- ALT levels decreased, relative to placebo, from baseline to Day 85/ET in both OCA 10 mg and OCA 50 mg groups.
- the mean (SD) ALT levels decreased from 86 (44) U/L at baseline to 54 (41) U/L at Day 85/ET in the OCA 10 mg group, and similarly decreased from 71 (38) U/L at baseline to 49 (29) U/L at Day 85/ET in the OCA 50 mg group.
- AST levels at Day 85/ET were 54 (40) U/L and 56 (28) U/L in OCA 10 mg and OCA 50 mg groups compared to baseline levels of 67 (33) U/L and 66 (29) U/L, respectively. There was no change in the levels of AST in the placebo group from Baseline to Day 85/ET.
- This example describes a study conducted using an international, multi-center, randomized, double- blind, placebo-controlled, multi-dose, parallel group to determine efficacy and safety of obeticholic acid (OCA) in combination with ursodeoxycholic acid (UDCA) in subjects with primary biliary cirrhosis.
- OCA obeticholic acid
- UDCA ursodeoxycholic acid
- AMA Positive antimitochondrial antibody
- PBC-specific antinuclear antibodies antinuclear dot and nuclear rim positive
- hepatic decompensation e.g. , variceal bleeds, encephalopathy, or poorly controlled ascites
- ELF Enhanced liver fibrosis
- Bile acid analysis Absolute and percent changes in the levels of total bile acids and OCA plasma concentrations, and their conjugates, from Baseline to Day 85/ET.
- FGF-19 fibroblast growth factor-19
- the mITT Population for the sensitivity analysis included ALP assessments obtained up to 15 days after the last investigational product use (unlike 7 days for primary endpoint). The number of subjects was balanced across all groups in all analysis populations with the exception of the Completer Population due to the higher proportion of
- Example 9 This example describes a randomized, double-blind, placebo-controlled, parallel- group, 12-month trial evaluating OCA in patients with PBC as a monotherapy. The study was performed using a randomized, double-blind, placebo-controlled, parallel-group, in patients with PBC who either: (1) were on ursodeoxycholic acid (UDCA) for at least 12 months (and on stable dose for 3 ⁇ 4 months), or (2) were unable to tolerate UDCA, and did not receive UDCA for 5 ⁇ 3 months prior to Day 0.
- UDCA ursodeoxycholic acid
- pre-treatment ALP 3.0 X ULN and/or aspartate aminotransferase (AST) ⁇ 2.0 X ULN and/or TB ULN; ( 'no ' for all three conditions, 'yes ' to at least one of the three conditions)
- AMA o Positive anti-mitochondrial antibody
- PBC specific antibodies anti-GP210 and/or anti-SPlOO and/or antibodies against the major M2 components [PDC-E2, 2-oxo- glutaric acid dehydrogenase complex]
- liver transplantation current placement on a liver transplant list or current Model for End Stage Liver Disease (MELD) score ⁇ 15 o Cirrhosis with complications, including history or presence of: spontaneous bacterial peritonitis, hepatocellular carcinoma, bilirubin > 2x ULN o Hepatorenal syndrome (type I or II) or Screening serum creatinine >
- liver disease e.g., hepatitis C, active hepatitis B, nonalcoholic steatohepatitis (NASH), alcoholic liver disease (ALD), autoimmune hepatitis, primary sclerosing cholangitis, Gilbert's Syndrome
- One goal of the study was to demonstrate the efficacy of OCA, relative to placebo, based on its effects on ALP and TB.
- ALP and TB composite response criteria were measured; a patient was designated as a responder if all three of the following conditions were met:
- OCA unconjugated
- conjugates glyco-OCA and tauro-OCA
- total OCA the sum of OCA unconjugated, glyco-OCA, and tauro-OCA
- Bile acid sequestrant (BAS) concomitant exposure.
- ITT Information-to-Treat
- PK analysis set was utilized, which consisted of all patients who had at least 1 confirmed fasted analyzable sample at and who did not have any major protocol deviations that could potentially affect exposure levels.
- CMH Cochran-Mantel-Haenszel
- the PK population was used to summarize OCA and bile acid concentrations.
- the change from Baseline concentrations within each treatment group was compared using a paired t-test.
- Descriptive statistics of OCA plasma concentrations and the extent of BAS concomitant exposure were provided by treatment group.
- Initial evaluation of the effects of BAS on OCA, total bile acid concentrations, and ALP was performed using a correlation analysis.
- FIG. 11 presents ALP concentrations over time, organized by originally randomized treatment group.
- FIG. 12 illustrates TB concentrations over time, organized by originally randomized treatment group for the 193 ITT patients continuing on open-label OCA treatment during the LTSE period.
- Dose Titration A total of 69 of 70 ITT patients from the OCA titration group completed month 6. Of these, 36 (52%) remained at 5 mg for the duration of the treatment period and 33 (48%) who did not meet the primary composite endpoint at Month 6, but, because they tolerated the investigational product, were titrated to 10 mg. Thirteen (39%) of the patients who up-titrated met the composite endpoint suggesting that a benefit can be gained with titration of OCA from 5 mg to 10 mg in those patients who did not respond to the 5 mg dose.
- ALP and total bilirubin were evaluated in relation to age at baseline, age at time of diagnosis, and years since diagnosis.
- the effect of OCA was consistent independent of age at diagnosis, duration of PBC, or years since diagnosis. In general, the subgroups were consistent with the observed effect in the overall ITT population. Greater improvements were observed in OCA-treated subjects, compared with placebo subjects.
- This example describes clinical pharmacology and dosing of obeticholic acid (OCA - including obeticholic acid compositions described herein).
- OCA obeticholic acid
- the starting dosage of OCA is 5 mg orally once daily in adult patients who have failed to achieve an adequate reduction in alkaline phosphatase on a stable dose of UDCA for an adequate duration or who were intolerant to UDCA.
- OCA can be supplied as an oral tablet containing obeticholic acid in a formulation as described herein.
- the dose of OCA can be increased to 10 mg once daily.
- OCA may be taken with or without food. Food does not have a clinically relevant effect on the PK of 10 mg OCA.
- Bile acid binding resins may be taken at least 4 hours before or 4 hours after (or at as great an interval as possible) OCA.
- Bile acid binding resins such as cholestyramine, colestipol, or colesevelam affect bile acid absorption and may reduce the absorption, systemic exposure, and efficacy of OCA.
- Dose adjustment may be needed in patients with hepatic impairment. Dose adjustment may not be needed in patients with mild hepatic impairment (Child-Pugh Class A). In some examples, the starting dosage is 5 mg once weekly for patients with moderate or severe hepatic impairment (Child-Pugh Class B or C). If an adequate reduction in alkaline phosphatase has not been achieved after 3 months of OCA 5 mg once weekly, and the patient is tolerating the drug, the OCA dose should be increased to 5 mg twice weekly and then to 5 mg every day depending on response and tolerability.
- Obeticholic acid is absorbed with peak plasma concentrations (Cmax) occurring at a median time (tmax) of approximately 2 hours. Co-administration with food does not alter the extent of absorption of obeticholic acid. Following multiple-dose administration of 5, 10, and 25 mg once daily for 14 days, systemic exposures of obeticholic acid increase dose proportionally. Exposures to glyco-obeticholic acid and tauro-obeticholic acid, and total obeticholic acid increase more than proportionally with dose.
- Cmax concentrations of OCA occurring at a median time (Tmax) of approximately 1.5 hours.
- Median Tm a x for glyco-OCA and tauro-OCA is 10 hours.
- Obeticholic acid is conjugated with glycine or taurine in the liver and secreted into bile. These glycine and taurine conjugates of obeticholic acid are absorbed in the small intestine leading to enterohepatic recirculation. The conjugates can be deconjugated in the ileum and colon by intestinal microbiota, leading to the conversion to obeticholic acid that can be reabsorbed or excreted in feces, the principal route of elimination.
- obeticholic acid After daily administration of obeticholic acid, there is accumulation of the glycine and taurine conjugates of obeticholic acid which have in vitro pharmacological activities similar to the parent drug, obeticholic acid.
- the metabolite-to-parent ratios of the glycine and taurine conjugates of obeticholic acid were 13.8 and 12.3, respectively, after daily administration.
- An additional third obeticholic acid metabolite, 3-glucuronide is formed but is considered to have minimal pharmacologic activity.
- the effective half-life of OCA is about 24 hours.
- Population PK analysis dataset consisted of 301 female and 505 male subjects, age ranging from 18 to 71 years and had 10 Asian, 233 Black, 554 White and 9 Other subjects.
- Obeticholic acid is not an inhibitor of CYP2C8 and did not cause a significant change in the expression of CYP2B6, CYP2C8, CYP2D6, MRP2, MRP3, MRP4, MATE1 , and OATP2B1. Obeticholic acid showed either no or weak effects on these metabolizing enzymes and transporters.
- Table 26 Percentage of Patients Achieving Response. A
Landscapes
- Health & Medical Sciences (AREA)
- Chemical & Material Sciences (AREA)
- Life Sciences & Earth Sciences (AREA)
- General Health & Medical Sciences (AREA)
- Veterinary Medicine (AREA)
- Public Health (AREA)
- Animal Behavior & Ethology (AREA)
- Medicinal Chemistry (AREA)
- Pharmacology & Pharmacy (AREA)
- Epidemiology (AREA)
- Engineering & Computer Science (AREA)
- Bioinformatics & Cheminformatics (AREA)
- Organic Chemistry (AREA)
- General Chemical & Material Sciences (AREA)
- Chemical Kinetics & Catalysis (AREA)
- Nuclear Medicine, Radiotherapy & Molecular Imaging (AREA)
- Molecular Biology (AREA)
- Virology (AREA)
- Biophysics (AREA)
- Gastroenterology & Hepatology (AREA)
- Oncology (AREA)
- Communicable Diseases (AREA)
- Pharmaceuticals Containing Other Organic And Inorganic Compounds (AREA)
- Medicinal Preparation (AREA)
- Acyclic And Carbocyclic Compounds In Medicinal Compositions (AREA)
- Organic Low-Molecular-Weight Compounds And Preparation Thereof (AREA)
- Steroid Compounds (AREA)
- Medicines That Contain Protein Lipid Enzymes And Other Medicines (AREA)
Abstract
Description










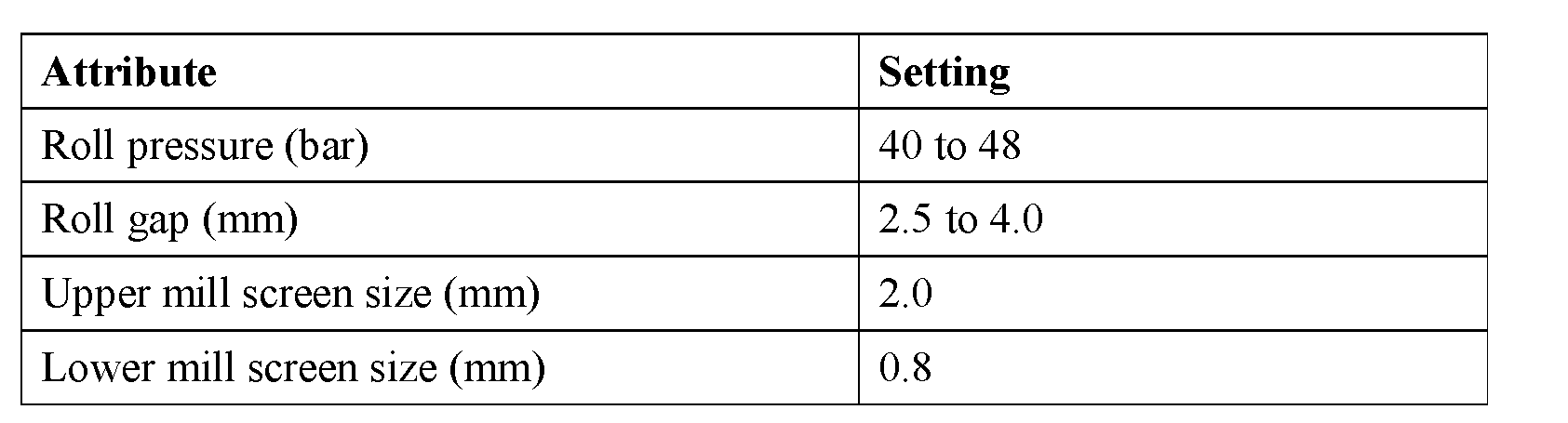












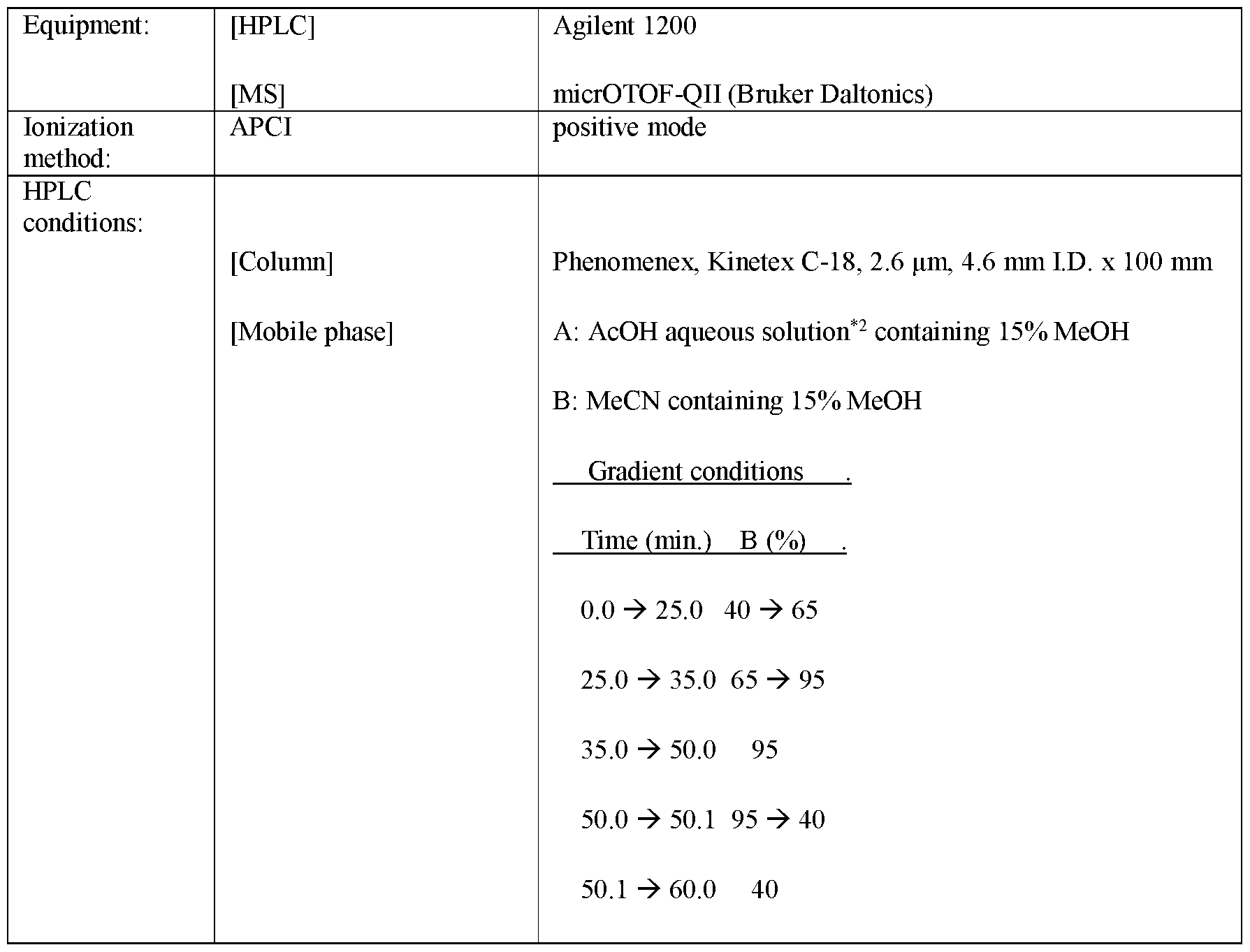


















Claims
Priority Applications (21)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| CR20170492A CR20170492A (en) | 2015-04-27 | 2016-04-26 | COMPOSITIONS OF OBETICOLIC ACID AND METHODS OF USE. |
| IL255269A IL255269B (en) | 2015-04-27 | 2016-04-26 | Compositions of obeticholic acid and methods of use |
| TNP/2017/000452A TN2017000452A1 (en) | 2015-04-27 | 2016-04-26 | Compositions of obeticholic acid and methods of use |
| KR1020177033948A KR20170140325A (en) | 2015-04-27 | 2016-04-26 | COMPOSITIONS AND METHODS OF OVETICOLICAN |
| JP2017555791A JP6941057B2 (en) | 2015-04-27 | 2016-04-26 | Composition and usage of obeticholic acid |
| SG11201708606VA SG11201708606VA (en) | 2015-04-27 | 2016-04-26 | Compositions of obeticholic acid and methods of use |
| EP21189718.6A EP3971199A1 (en) | 2015-04-27 | 2016-04-26 | Compositions of obeticholic acid and methods of use |
| CA2983609A CA2983609C (en) | 2015-04-27 | 2016-04-26 | Compositions of obeticholic acid and methods of use |
| BR112017023161-1A BR112017023161A2 (en) | 2015-04-27 | 2016-04-26 | obeticolic acid compositions and methods of use |
| EP16787000.5A EP3288958A4 (en) | 2015-04-27 | 2016-04-26 | Compositions of obeticholic acid and methods of use |
| EA201792354A EA201792354A1 (en) | 2015-04-27 | 2016-04-26 | BATCHOLEIC ACID COMPOSITIONS AND METHODS OF APPLICATION |
| MA41529A MA41529A1 (en) | 2015-04-27 | 2016-04-26 | Obeticholic acid compositions and methods of use |
| EP24154375.0A EP4371616A3 (en) | 2015-04-27 | 2016-04-26 | Compositions of obeticholic acid and methods of use |
| IL294575A IL294575A (en) | 2015-04-27 | 2016-04-26 | Compositions of obeticholic acid and methods of use |
| MX2017013805A MX2017013805A (en) | 2015-04-27 | 2016-04-26 | Compositions of obeticholic acid and methods of use. |
| AU2016255045A AU2016255045B2 (en) | 2015-04-27 | 2016-04-26 | Compositions of obeticholic acid and methods of use |
| CN201680023889.2A CN107531742A (en) | 2015-04-27 | 2016-04-26 | The composition and application method of shellfish cholic acid difficult to understand |
| PH12017501956A PH12017501956A1 (en) | 2015-04-27 | 2017-10-26 | Compositions of obeticholic acid and methods of use |
| CONC2017/0011535A CO2017011535A2 (en) | 2015-04-27 | 2017-11-10 | Compositions of obetolic acid and methods of use |
| ZA2017/07981A ZA201707981B (en) | 2015-04-27 | 2017-11-23 | Compositions of obeticholic acid and methods of use |
| AU2020205315A AU2020205315A1 (en) | 2015-04-27 | 2020-07-16 | Compositions of obeticholic acid and methods of use |
Applications Claiming Priority (4)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| US201562153040P | 2015-04-27 | 2015-04-27 | |
| US62/153,040 | 2015-04-27 | ||
| US201662317933P | 2016-04-04 | 2016-04-04 | |
| US62/317,933 | 2016-04-04 |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| WO2016176208A1 true WO2016176208A1 (en) | 2016-11-03 |
Family
ID=57198868
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| PCT/US2016/029369 WO2016176208A1 (en) | 2015-04-27 | 2016-04-26 | Compositions of obeticholic acid and methods of use |
Country Status (25)
| Country | Link |
|---|---|
| US (8) | US10052337B2 (en) |
| EP (3) | EP4371616A3 (en) |
| JP (2) | JP6941057B2 (en) |
| KR (1) | KR20170140325A (en) |
| CN (1) | CN107531742A (en) |
| AU (2) | AU2016255045B2 (en) |
| BR (1) | BR112017023161A2 (en) |
| CA (1) | CA2983609C (en) |
| CL (1) | CL2017002727A1 (en) |
| CO (1) | CO2017011535A2 (en) |
| CR (1) | CR20170492A (en) |
| EA (1) | EA201792354A1 (en) |
| EC (1) | ECSP17078433A (en) |
| IL (2) | IL294575A (en) |
| MA (1) | MA41999A (en) |
| MX (1) | MX2017013805A (en) |
| NI (1) | NI201700128A (en) |
| PE (1) | PE20180690A1 (en) |
| PH (1) | PH12017501956A1 (en) |
| SG (2) | SG11201708606VA (en) |
| SV (1) | SV2017005555A (en) |
| TN (1) | TN2017000452A1 (en) |
| TW (1) | TWI723017B (en) |
| WO (1) | WO2016176208A1 (en) |
| ZA (1) | ZA201707981B (en) |
Cited By (19)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| CN106645497A (en) * | 2017-01-03 | 2017-05-10 | 山东省药学科学院 | Obeticholic acid and detection method for related substances in preparation of obeticholic acid |
| WO2018085623A1 (en) * | 2016-11-04 | 2018-05-11 | Children's Hospital Medical Center | Compositions and methods of treating liver disease |
| CN108072729A (en) * | 2016-11-18 | 2018-05-25 | 华北制药集团新药研究开发有限责任公司 | A kind of method for measuring shellfish cholic acid piece dissolution rate difficult to understand |
| CN108614038A (en) * | 2016-12-13 | 2018-10-02 | 亚宝药业集团股份有限公司 | A method of measuring the related substance of shellfish cholic acid bulk pharmaceutical chemicals difficult to understand |
| US10174289B2 (en) | 2014-05-28 | 2019-01-08 | Children's Hospital Medical Center | Methods and systems for converting precursor cells into gastric tissues through directed differentiation |
| US20190216779A1 (en) * | 2016-06-29 | 2019-07-18 | Menlo Therapeutics Inc. | Use of neurokinin-1 antagonists to treat a variety of pruritic conditions |
| EP3437645A4 (en) * | 2016-03-31 | 2019-12-04 | Intercept Pharmaceuticals, Inc. | Film-coated tablet having high chemical stability of active ingredient |
| EP3442946A4 (en) * | 2016-04-13 | 2019-12-04 | Intercept Pharmaceuticals, Inc. | Methods of treating cancer |
| WO2020025942A1 (en) | 2018-07-30 | 2020-02-06 | NZP UK Limited | Fluorinated bile acid derivatives |
| JP2020510009A (en) * | 2017-03-07 | 2020-04-02 | インターセプト ファーマシューティカルズ, インコーポレイテッド | How to treat cancer |
| US10781425B2 (en) | 2010-05-06 | 2020-09-22 | Children's Hospital Medical Center | Methods and systems for converting precursor cells into intestinal tissues through directed differentiation |
| US11066650B2 (en) | 2016-05-05 | 2021-07-20 | Children's Hospital Medical Center | Methods for the in vitro manufacture of gastric fundus tissue and compositions related to same |
| CN113271951A (en) * | 2018-11-08 | 2021-08-17 | 英特塞普特医药品公司 | Methods of using obeticholic acid |
| US11584916B2 (en) | 2014-10-17 | 2023-02-21 | Children's Hospital Medical Center | Method of making in vivo human small intestine organoids from pluripotent stem cells |
| US11767515B2 (en) | 2016-12-05 | 2023-09-26 | Children's Hospital Medical Center | Colonic organoids and methods of making and using same |
| WO2023181077A1 (en) * | 2022-03-24 | 2023-09-28 | Zenvision Pharma Llp | Stable liquid composition comprising obeticholic acid or salts thereof |
| WO2024043842A1 (en) * | 2022-08-22 | 2024-02-29 | Pharmactive Ilac Sanayi Ve Ticaret A.S. | Pharmaceutical compositions comprising chenodeoxycholic acid (cdca) as active ingredient and other relevant excipients |
| EP4116710A4 (en) * | 2020-03-06 | 2024-04-24 | Mili Healthcare Trade DMCC, Limited Liability Company | Use of a group of markers for diagnosing and adjusting treatment of primary biliary cholangitis, pharmaceutical composition and solid dosage form for treating primary biliary cholangitis |
| WO2024104960A1 (en) | 2022-11-15 | 2024-05-23 | Synthon B.V. | Stable formulation comprising obeticholic acid |
Families Citing this family (18)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| PE20180690A1 (en) * | 2015-04-27 | 2018-04-23 | Intercept Pharmaceuticals Inc | OBETICOLIC ACID COMPOSITIONS AND METHODS OF USE |
| KR20200031145A (en) * | 2017-07-24 | 2020-03-23 | 인터셉트 파마슈티컬즈, 인크. | Isotopically labeled bile acid derivatives |
| WO2019106043A1 (en) * | 2017-11-29 | 2019-06-06 | Hexal Ag | Pharmaceutical composition comprising obeticholic acid |
| CN108572251B (en) * | 2018-05-31 | 2020-01-17 | 中国科学院昆明动物研究所 | Small molecule marker for early stage of cirrhosis and application thereof |
| US11524029B2 (en) | 2018-08-13 | 2022-12-13 | Viscera Labs, Inc. | Therapeutic composition and methods |
| US11590161B2 (en) | 2018-08-13 | 2023-02-28 | Viscera Labs, Inc. | Therapeutic composition and methods |
| CN109432431B (en) * | 2018-12-14 | 2020-06-30 | 中国药科大学 | Composition containing SUMO inhibitor and application |
| CN109655571B (en) * | 2019-01-08 | 2021-07-13 | 丽珠集团新北江制药股份有限公司 | High performance liquid chromatography analysis method of obeticholic acid |
| CN109620812B (en) * | 2019-01-16 | 2023-07-21 | 浙江华海药业股份有限公司 | Preparation method of obeticholic acid composition |
| CN113874023A (en) * | 2019-03-26 | 2021-12-31 | 英特塞普特医药品公司 | Methods of using obeticholic acid for diagnosis and treatment of liver disease |
| WO2020198576A1 (en) * | 2019-03-28 | 2020-10-01 | The Board Of Trustees Of The University Of Illinois | Methods of modulating regulatory t cells |
| CN111690731B (en) * | 2020-05-22 | 2021-09-28 | 河南大学 | Use of FXR agonists for the treatment of hepatic encephalopathy |
| CN111812264B (en) * | 2020-07-09 | 2021-06-15 | 苏州旭辉检测有限公司 | Biological sample analysis method of deoxycholic acid compound |
| WO2022051321A1 (en) | 2020-09-03 | 2022-03-10 | Coherus Biosciences, Inc. | Fixed dose combinations of chs-131 and a fxr agonist |
| WO2022076683A1 (en) * | 2020-10-07 | 2022-04-14 | Intercept Pharmaceuticals, Inc. | Methods of treating coronaviral infection with obeticholic acid |
| CN113143950B (en) * | 2021-05-17 | 2023-04-18 | 河北医科大学第二医院 | Pharmaceutical composition for treating liver diseases and application thereof |
| WO2023147141A1 (en) * | 2022-01-28 | 2023-08-03 | Intercept Pharmaceuticals, Inc. | Combination therapy |
| AU2023257308A1 (en) * | 2022-04-21 | 2024-10-10 | Intercept Pharmaceuticals, Inc. | Uses of farnesoid x receptor agonists |
Citations (6)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US20050101565A1 (en) * | 2002-07-03 | 2005-05-12 | Esperion Therapeutics, Inc. | Pharmaceutical compositions and methods for treating, preventing, and managing cholesterol, dyslipidemia, and related disorders |
| US7078376B1 (en) * | 2000-08-11 | 2006-07-18 | Baxter Healthcare S.A. | Therapeutic methods for treating subjects with a recombinant erythropoietin having high activity and reduced side effects |
| US20120071451A1 (en) * | 2009-03-17 | 2012-03-22 | Aptalis Pharma Canada Inc. | Method of treating nonalcoholic steatohepatitis with elevated doses of ursodeoxycholic acid |
| US20120160944A1 (en) * | 2009-04-24 | 2012-06-28 | Aaron Dodd | Method for the production of commercial nanoparticle and micro particle powders |
| US20130345188A1 (en) * | 2012-06-19 | 2013-12-26 | Intercept Pharmaceuticals, Inc. | Preparation and Uses of Obeticholic Acid |
| WO2015036442A1 (en) * | 2013-09-11 | 2015-03-19 | INSERM (Institut National de la Santé et de la Recherche Médicale) | Methods and pharmaceutical compositions for the treatment of hepatitis b virus infection |
Family Cites Families (18)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US4522811A (en) | 1982-07-08 | 1985-06-11 | Syntex (U.S.A.) Inc. | Serial injection of muramyldipeptides and liposomes enhances the anti-infective activity of muramyldipeptides |
| US5023252A (en) | 1985-12-04 | 1991-06-11 | Conrex Pharmaceutical Corporation | Transdermal and trans-membrane delivery of drugs |
| ZA876640B (en) * | 1986-09-26 | 1988-03-08 | Warner-Lambert Company | Treated lipid regulator |
| UA72207C2 (en) | 1998-04-07 | 2005-02-15 | Брістол- Майєрс Сквібб Фарма Компані | Pharmaceutical formulations of efavirenz and disintegrants providing for increasing dissolution rate and process of manufacturing such tablets or capsules |
| DK1392714T3 (en) | 2001-03-12 | 2006-01-09 | Intercept Pharmaceuticals Inc | Steroids as Agonists for FXR |
| KR100943309B1 (en) | 2001-06-14 | 2010-02-23 | 오츠카 세이야쿠 가부시키가이샤 | Medicinal compositions |
| US6933380B2 (en) | 2001-10-19 | 2005-08-23 | Yung-Zip Chemical Ind. Co., Ltd. | Excipients containing low residual solvent and method for producing the same |
| US20050101505A1 (en) * | 2003-11-06 | 2005-05-12 | Daniel Wood | Liquid laundry detergent composition having improved color-care properties |
| GB0402492D0 (en) | 2004-02-04 | 2004-03-10 | Pfizer Ltd | Pharmaceutically active compounds |
| GB0425758D0 (en) | 2004-11-23 | 2004-12-22 | Vectura Ltd | Preparation of pharmaceutical compositions |
| CA2614409C (en) | 2005-07-07 | 2014-05-20 | Nanotherapeutics, Inc | Process for milling and preparing powders and compositions produced thereby |
| DE102007009242A1 (en) | 2007-02-22 | 2008-09-18 | Evonik Röhm Gmbh | Pellets with enteric-coated matix |
| KR20130076818A (en) | 2010-04-20 | 2013-07-08 | 시플라 리미티드 | Pharmaceutical compositions |
| US9814733B2 (en) * | 2012-12-31 | 2017-11-14 | A,arin Pharmaceuticals Ireland Limited | Compositions comprising EPA and obeticholic acid and methods of use thereof |
| EP2968245B1 (en) | 2013-03-15 | 2021-05-05 | Mochida Pharmaceutical Co., Ltd. | Compositions and methods for treating non-alcoholic steatohepatitis |
| ES2847002T3 (en) | 2013-05-14 | 2021-07-30 | Intercept Pharmaceuticals Inc | 11-hydroxyl-6-substituted derivatives of bile acids and amino acid conjugates thereof as modulators of the farnesoid X receptor |
| CN105801653B (en) | 2014-12-30 | 2018-04-17 | 苏州晶云药物科技有限公司 | Crystal form A of shellfish cholic acid difficult to understand and preparation method thereof |
| PE20180690A1 (en) | 2015-04-27 | 2018-04-23 | Intercept Pharmaceuticals Inc | OBETICOLIC ACID COMPOSITIONS AND METHODS OF USE |
-
2016
- 2016-04-24 PE PE2017002334A patent/PE20180690A1/en unknown
- 2016-04-26 IL IL294575A patent/IL294575A/en unknown
- 2016-04-26 EP EP24154375.0A patent/EP4371616A3/en active Pending
- 2016-04-26 CA CA2983609A patent/CA2983609C/en active Active
- 2016-04-26 CR CR20170492A patent/CR20170492A/en unknown
- 2016-04-26 WO PCT/US2016/029369 patent/WO2016176208A1/en active Application Filing
- 2016-04-26 IL IL255269A patent/IL255269B/en unknown
- 2016-04-26 AU AU2016255045A patent/AU2016255045B2/en active Active
- 2016-04-26 EP EP16787000.5A patent/EP3288958A4/en not_active Withdrawn
- 2016-04-26 SG SG11201708606VA patent/SG11201708606VA/en unknown
- 2016-04-26 US US15/139,138 patent/US10052337B2/en active Active
- 2016-04-26 SG SG10202003110PA patent/SG10202003110PA/en unknown
- 2016-04-26 EP EP21189718.6A patent/EP3971199A1/en not_active Withdrawn
- 2016-04-26 BR BR112017023161-1A patent/BR112017023161A2/en not_active Application Discontinuation
- 2016-04-26 KR KR1020177033948A patent/KR20170140325A/en unknown
- 2016-04-26 EA EA201792354A patent/EA201792354A1/en unknown
- 2016-04-26 MA MA041999A patent/MA41999A/en unknown
- 2016-04-26 TN TNP/2017/000452A patent/TN2017000452A1/en unknown
- 2016-04-26 JP JP2017555791A patent/JP6941057B2/en active Active
- 2016-04-26 MX MX2017013805A patent/MX2017013805A/en unknown
- 2016-04-26 CN CN201680023889.2A patent/CN107531742A/en active Pending
- 2016-04-27 TW TW105113063A patent/TWI723017B/en active
-
2017
- 2017-10-26 CL CL2017002727A patent/CL2017002727A1/en unknown
- 2017-10-26 PH PH12017501956A patent/PH12017501956A1/en unknown
- 2017-10-26 NI NI201700128A patent/NI201700128A/en unknown
- 2017-10-27 SV SV2017005555A patent/SV2017005555A/en unknown
- 2017-11-10 CO CONC2017/0011535A patent/CO2017011535A2/en unknown
- 2017-11-23 ZA ZA2017/07981A patent/ZA201707981B/en unknown
- 2017-11-24 EC ECIEPI201778433A patent/ECSP17078433A/en unknown
-
2018
- 2018-07-09 US US16/030,141 patent/US10646499B2/en active Active
-
2019
- 2019-01-15 US US16/248,512 patent/US10751349B2/en active Active
- 2019-10-08 US US16/596,216 patent/US20200046735A1/en not_active Abandoned
- 2019-10-08 US US16/596,741 patent/US20200046736A1/en not_active Abandoned
- 2019-10-09 US US16/597,412 patent/US20200054650A1/en not_active Abandoned
-
2020
- 2020-02-11 US US16/787,796 patent/US10758549B2/en active Active
- 2020-07-16 AU AU2020205315A patent/AU2020205315A1/en not_active Abandoned
-
2021
- 2021-09-03 JP JP2021143835A patent/JP2021183651A/en active Pending
- 2021-12-06 US US17/542,923 patent/US20220133745A1/en active Pending
Patent Citations (6)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US7078376B1 (en) * | 2000-08-11 | 2006-07-18 | Baxter Healthcare S.A. | Therapeutic methods for treating subjects with a recombinant erythropoietin having high activity and reduced side effects |
| US20050101565A1 (en) * | 2002-07-03 | 2005-05-12 | Esperion Therapeutics, Inc. | Pharmaceutical compositions and methods for treating, preventing, and managing cholesterol, dyslipidemia, and related disorders |
| US20120071451A1 (en) * | 2009-03-17 | 2012-03-22 | Aptalis Pharma Canada Inc. | Method of treating nonalcoholic steatohepatitis with elevated doses of ursodeoxycholic acid |
| US20120160944A1 (en) * | 2009-04-24 | 2012-06-28 | Aaron Dodd | Method for the production of commercial nanoparticle and micro particle powders |
| US20130345188A1 (en) * | 2012-06-19 | 2013-12-26 | Intercept Pharmaceuticals, Inc. | Preparation and Uses of Obeticholic Acid |
| WO2015036442A1 (en) * | 2013-09-11 | 2015-03-19 | INSERM (Institut National de la Santé et de la Recherche Médicale) | Methods and pharmaceutical compositions for the treatment of hepatitis b virus infection |
Non-Patent Citations (1)
| Title |
|---|
| See also references of EP3288958A4 * |
Cited By (26)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US10781425B2 (en) | 2010-05-06 | 2020-09-22 | Children's Hospital Medical Center | Methods and systems for converting precursor cells into intestinal tissues through directed differentiation |
| US10174289B2 (en) | 2014-05-28 | 2019-01-08 | Children's Hospital Medical Center | Methods and systems for converting precursor cells into gastric tissues through directed differentiation |
| US11053477B2 (en) | 2014-05-28 | 2021-07-06 | Children's Hospital Medical Center | Methods and systems for converting precursor cells into gastric tissues through directed differentiation |
| US11584916B2 (en) | 2014-10-17 | 2023-02-21 | Children's Hospital Medical Center | Method of making in vivo human small intestine organoids from pluripotent stem cells |
| US11331273B2 (en) | 2016-03-31 | 2022-05-17 | Intercept Pharmaceuticals, Inc. | Film-coated tablet having high chemical stability of active ingredient |
| EP3437645A4 (en) * | 2016-03-31 | 2019-12-04 | Intercept Pharmaceuticals, Inc. | Film-coated tablet having high chemical stability of active ingredient |
| EP3442946A4 (en) * | 2016-04-13 | 2019-12-04 | Intercept Pharmaceuticals, Inc. | Methods of treating cancer |
| US11066650B2 (en) | 2016-05-05 | 2021-07-20 | Children's Hospital Medical Center | Methods for the in vitro manufacture of gastric fundus tissue and compositions related to same |
| US20190216779A1 (en) * | 2016-06-29 | 2019-07-18 | Menlo Therapeutics Inc. | Use of neurokinin-1 antagonists to treat a variety of pruritic conditions |
| CN110382012B (en) * | 2016-11-04 | 2023-08-25 | 儿童医院医学中心 | Liver organoid disease model and methods of making and using the same |
| WO2018085623A1 (en) * | 2016-11-04 | 2018-05-11 | Children's Hospital Medical Center | Compositions and methods of treating liver disease |
| US10668108B2 (en) | 2016-11-04 | 2020-06-02 | Children's Hospital Medical Center | Compositions and methods of treating liver disease |
| CN110382012A (en) * | 2016-11-04 | 2019-10-25 | 儿童医院医学中心 | Liver organoid disease model and its preparation and application |
| CN108072729A (en) * | 2016-11-18 | 2018-05-25 | 华北制药集团新药研究开发有限责任公司 | A kind of method for measuring shellfish cholic acid piece dissolution rate difficult to understand |
| US11767515B2 (en) | 2016-12-05 | 2023-09-26 | Children's Hospital Medical Center | Colonic organoids and methods of making and using same |
| CN108614038A (en) * | 2016-12-13 | 2018-10-02 | 亚宝药业集团股份有限公司 | A method of measuring the related substance of shellfish cholic acid bulk pharmaceutical chemicals difficult to understand |
| CN106645497A (en) * | 2017-01-03 | 2017-05-10 | 山东省药学科学院 | Obeticholic acid and detection method for related substances in preparation of obeticholic acid |
| JP7042836B2 (en) | 2017-03-07 | 2022-03-28 | インターセプト ファーマシューティカルズ, インコーポレイテッド | How to treat cancer |
| JP2020510009A (en) * | 2017-03-07 | 2020-04-02 | インターセプト ファーマシューティカルズ, インコーポレイテッド | How to treat cancer |
| EP3592357A4 (en) * | 2017-03-07 | 2021-01-13 | Intercept Pharmaceuticals, Inc. | Methods of treating cancer |
| WO2020025942A1 (en) | 2018-07-30 | 2020-02-06 | NZP UK Limited | Fluorinated bile acid derivatives |
| CN113271951A (en) * | 2018-11-08 | 2021-08-17 | 英特塞普特医药品公司 | Methods of using obeticholic acid |
| EP4116710A4 (en) * | 2020-03-06 | 2024-04-24 | Mili Healthcare Trade DMCC, Limited Liability Company | Use of a group of markers for diagnosing and adjusting treatment of primary biliary cholangitis, pharmaceutical composition and solid dosage form for treating primary biliary cholangitis |
| WO2023181077A1 (en) * | 2022-03-24 | 2023-09-28 | Zenvision Pharma Llp | Stable liquid composition comprising obeticholic acid or salts thereof |
| WO2024043842A1 (en) * | 2022-08-22 | 2024-02-29 | Pharmactive Ilac Sanayi Ve Ticaret A.S. | Pharmaceutical compositions comprising chenodeoxycholic acid (cdca) as active ingredient and other relevant excipients |
| WO2024104960A1 (en) | 2022-11-15 | 2024-05-23 | Synthon B.V. | Stable formulation comprising obeticholic acid |
Also Published As
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| US10758549B2 (en) | Compositions of obeticholic acid and methods of use | |
| AU2017249226B2 (en) | Methods of treating cancer | |
| US20220184099A1 (en) | Methods of using obeticholic acid | |
| US20180256600A1 (en) | Methods of treating cancer | |
| CA3055308A1 (en) | Methods of treating cancer |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| 121 | Ep: the epo has been informed by wipo that ep was designated in this application |
Ref document number: 16787000 Country of ref document: EP Kind code of ref document: A1 |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 11201708606V Country of ref document: SG |
|
| ENP | Entry into the national phase |
Ref document number: 2983609 Country of ref document: CA |
|
| ENP | Entry into the national phase |
Ref document number: 2017555791 Country of ref document: JP Kind code of ref document: A |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 2017-000128 I Country of ref document: NI Ref document number: 255269 Country of ref document: IL Ref document number: MX/A/2017/013805 Country of ref document: MX |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 002334-2017 Country of ref document: PE Ref document number: CR2017-000492 Country of ref document: CR Ref document number: 12017501956 Country of ref document: PH |
|
| NENP | Non-entry into the national phase |
Ref country code: DE |
|
| REG | Reference to national code |
Ref country code: BR Ref legal event code: B01A Ref document number: 112017023161 Country of ref document: BR |
|
| ENP | Entry into the national phase |
Ref document number: 2016255045 Country of ref document: AU Date of ref document: 20160426 Kind code of ref document: A |
|
| WWE | Wipo information: entry into national phase |
Ref document number: NC2017/0011535 Country of ref document: CO |
|
| ENP | Entry into the national phase |
Ref document number: 20177033948 Country of ref document: KR Kind code of ref document: A |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 41529 Country of ref document: MA |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 201792354 Country of ref document: EA |
|
| WWE | Wipo information: entry into national phase |
Ref document number: A201710461 Country of ref document: UA |
|
| ENP | Entry into the national phase |
Ref document number: 112017023161 Country of ref document: BR Kind code of ref document: A2 Effective date: 20171026 |