WO2015006828A1 - A method for treating haemorrhage, shock and brain injury - Google Patents
A method for treating haemorrhage, shock and brain injury Download PDFInfo
- Publication number
- WO2015006828A1 WO2015006828A1 PCT/AU2014/050130 AU2014050130W WO2015006828A1 WO 2015006828 A1 WO2015006828 A1 WO 2015006828A1 AU 2014050130 W AU2014050130 W AU 2014050130W WO 2015006828 A1 WO2015006828 A1 WO 2015006828A1
- Authority
- WO
- WIPO (PCT)
- Prior art keywords
- composition
- adenosine
- blood
- bolus
- brain
- Prior art date
Links
- 238000000034 method Methods 0.000 title claims abstract description 114
- 230000035939 shock Effects 0.000 title claims abstract description 67
- 208000032843 Hemorrhage Diseases 0.000 title description 41
- 208000029028 brain injury Diseases 0.000 title description 32
- 239000000203 mixture Substances 0.000 claims abstract description 216
- 208000001953 Hypotension Diseases 0.000 claims abstract description 77
- 230000036772 blood pressure Effects 0.000 claims abstract description 64
- 150000001875 compounds Chemical class 0.000 claims abstract description 62
- 230000001603 reducing effect Effects 0.000 claims abstract description 52
- 239000003416 antiarrhythmic agent Substances 0.000 claims abstract description 48
- 230000001965 increasing effect Effects 0.000 claims abstract description 48
- 239000003379 purinergic P1 receptor agonist Substances 0.000 claims abstract description 47
- 208000021822 hypotensive Diseases 0.000 claims abstract description 44
- 230000001077 hypotensive effect Effects 0.000 claims abstract description 44
- 229940122614 Adenosine receptor agonist Drugs 0.000 claims abstract description 43
- 239000004036 potassium channel stimulating agent Substances 0.000 claims abstract description 41
- 230000003444 anaesthetic effect Effects 0.000 claims abstract description 40
- 230000036543 hypotension Effects 0.000 claims abstract description 33
- 229940122117 Potassium channel agonist Drugs 0.000 claims abstract description 28
- 206010002091 Anaesthesia Diseases 0.000 claims abstract description 23
- 230000037005 anaesthesia Effects 0.000 claims abstract description 23
- 238000001949 anaesthesia Methods 0.000 claims abstract description 15
- 208000002193 Pain Diseases 0.000 claims abstract description 14
- 230000036407 pain Effects 0.000 claims abstract description 14
- 230000000202 analgesic effect Effects 0.000 claims abstract description 11
- OIRDTQYFTABQOQ-KQYNXXCUSA-N adenosine group Chemical group [C@@H]1([C@H](O)[C@H](O)[C@@H](CO)O1)N1C=NC=2C(N)=NC=NC12 OIRDTQYFTABQOQ-KQYNXXCUSA-N 0.000 claims description 194
- 239000002126 C01EB10 - Adenosine Substances 0.000 claims description 96
- 229960005305 adenosine Drugs 0.000 claims description 96
- 238000001802 infusion Methods 0.000 claims description 87
- NNJVILVZKWQKPM-UHFFFAOYSA-N Lidocaine Chemical compound CCN(CC)CC(=O)NC1=C(C)C=CC=C1C NNJVILVZKWQKPM-UHFFFAOYSA-N 0.000 claims description 55
- 229960004194 lidocaine Drugs 0.000 claims description 55
- KRKNYBCHXYNGOX-UHFFFAOYSA-K Citrate Chemical compound [O-]C(=O)CC(O)(CC([O-])=O)C([O-])=O KRKNYBCHXYNGOX-UHFFFAOYSA-K 0.000 claims description 34
- 239000011777 magnesium Substances 0.000 claims description 32
- FYYHWMGAXLPEAU-UHFFFAOYSA-N Magnesium Chemical compound [Mg] FYYHWMGAXLPEAU-UHFFFAOYSA-N 0.000 claims description 29
- 229910052749 magnesium Inorganic materials 0.000 claims description 29
- 229940091250 magnesium supplement Drugs 0.000 claims description 29
- 239000003795 chemical substances by application Substances 0.000 claims description 20
- 239000003937 drug carrier Substances 0.000 claims description 16
- 239000000556 agonist Substances 0.000 claims description 14
- 230000001939 inductive effect Effects 0.000 claims description 14
- 150000003839 salts Chemical class 0.000 claims description 13
- 239000000872 buffer Substances 0.000 claims description 8
- RSGFPIWWSCWCFJ-VAXZQHAWSA-N 2-hydroxypropane-1,2,3-tricarboxylic acid;(2r,3s,4r,5r)-2,3,4,5,6-pentahydroxyhexanal;phosphoric acid Chemical group OP(O)(O)=O.OC[C@@H](O)[C@@H](O)[C@H](O)[C@@H](O)C=O.OC(=O)CC(O)(C(O)=O)CC(O)=O RSGFPIWWSCWCFJ-VAXZQHAWSA-N 0.000 claims description 5
- NLJMYIDDQXHKNR-UHFFFAOYSA-K sodium citrate Chemical compound O.O.[Na+].[Na+].[Na+].[O-]C(=O)CC(O)(CC([O-])=O)C([O-])=O NLJMYIDDQXHKNR-UHFFFAOYSA-K 0.000 claims description 4
- 239000001509 sodium citrate Substances 0.000 claims description 4
- DEIYFTQMQPDXOT-UHFFFAOYSA-N sildenafil citrate Chemical compound OC(=O)CC(O)(C(O)=O)CC(O)=O.CCCC1=NN(C)C(C(N2)=O)=C1N=C2C(C(=CC=1)OCC)=CC=1S(=O)(=O)N1CCN(C)CC1 DEIYFTQMQPDXOT-UHFFFAOYSA-N 0.000 claims description 3
- 229960002639 sildenafil citrate Drugs 0.000 claims description 3
- 239000004337 magnesium citrate Substances 0.000 claims description 2
- 229960005336 magnesium citrate Drugs 0.000 claims description 2
- 235000002538 magnesium citrate Nutrition 0.000 claims description 2
- 239000001508 potassium citrate Substances 0.000 claims description 2
- 229960002635 potassium citrate Drugs 0.000 claims description 2
- QEEAPRPFLLJWCF-UHFFFAOYSA-K potassium citrate (anhydrous) Chemical compound [K+].[K+].[K+].[O-]C(=O)CC(O)(CC([O-])=O)C([O-])=O QEEAPRPFLLJWCF-UHFFFAOYSA-K 0.000 claims description 2
- 235000011082 potassium citrates Nutrition 0.000 claims description 2
- 229960001790 sodium citrate Drugs 0.000 claims description 2
- 235000011083 sodium citrates Nutrition 0.000 claims description 2
- PLSARIKBYIPYPF-UHFFFAOYSA-H trimagnesium dicitrate Chemical compound [Mg+2].[Mg+2].[Mg+2].[O-]C(=O)CC(O)(CC([O-])=O)C([O-])=O.[O-]C(=O)CC(O)(CC([O-])=O)C([O-])=O PLSARIKBYIPYPF-UHFFFAOYSA-H 0.000 claims description 2
- 210000002216 heart Anatomy 0.000 description 133
- 210000004369 blood Anatomy 0.000 description 120
- 239000008280 blood Substances 0.000 description 120
- 210000001519 tissue Anatomy 0.000 description 92
- 208000014674 injury Diseases 0.000 description 91
- 230000006378 damage Effects 0.000 description 89
- 241001465754 Metazoa Species 0.000 description 79
- 210000004556 brain Anatomy 0.000 description 79
- 210000004027 cell Anatomy 0.000 description 78
- 230000000694 effects Effects 0.000 description 75
- FAPWRFPIFSIZLT-UHFFFAOYSA-M Sodium chloride Chemical compound [Na+].[Cl-] FAPWRFPIFSIZLT-UHFFFAOYSA-M 0.000 description 71
- 208000027418 Wounds and injury Diseases 0.000 description 68
- 238000011282 treatment Methods 0.000 description 68
- 210000000056 organ Anatomy 0.000 description 63
- 206010040047 Sepsis Diseases 0.000 description 55
- 208000015181 infectious disease Diseases 0.000 description 51
- 241000700159 Rattus Species 0.000 description 48
- 239000011780 sodium chloride Substances 0.000 description 46
- 238000001356 surgical procedure Methods 0.000 description 43
- 238000001990 intravenous administration Methods 0.000 description 41
- 239000000243 solution Substances 0.000 description 38
- 230000000747 cardiac effect Effects 0.000 description 36
- 230000004224 protection Effects 0.000 description 35
- 230000002503 metabolic effect Effects 0.000 description 34
- 208000030886 Traumatic Brain injury Diseases 0.000 description 33
- 206010061218 Inflammation Diseases 0.000 description 32
- 230000004054 inflammatory process Effects 0.000 description 32
- 230000009529 traumatic brain injury Effects 0.000 description 32
- XLYOFNOQVPJJNP-UHFFFAOYSA-N water Substances O XLYOFNOQVPJJNP-UHFFFAOYSA-N 0.000 description 32
- 239000000446 fuel Substances 0.000 description 30
- MWUXSHHQAYIFBG-UHFFFAOYSA-N Nitric oxide Chemical compound O=[N] MWUXSHHQAYIFBG-UHFFFAOYSA-N 0.000 description 28
- 229940127291 Calcium channel antagonist Drugs 0.000 description 27
- 239000002260 anti-inflammatory agent Substances 0.000 description 27
- 229940121363 anti-inflammatory agent Drugs 0.000 description 27
- 238000005345 coagulation Methods 0.000 description 27
- -1 heat Substances 0.000 description 27
- WHBMMWSBFZVSSR-UHFFFAOYSA-N 3-hydroxybutyric acid Chemical compound CC(O)CC(O)=O WHBMMWSBFZVSSR-UHFFFAOYSA-N 0.000 description 26
- 208000010496 Heart Arrest Diseases 0.000 description 26
- 230000015271 coagulation Effects 0.000 description 26
- 239000003814 drug Substances 0.000 description 26
- 206010053567 Coagulopathies Diseases 0.000 description 25
- 206010049771 Shock haemorrhagic Diseases 0.000 description 25
- 239000011575 calcium Substances 0.000 description 25
- 230000006870 function Effects 0.000 description 25
- 208000032456 Hemorrhagic Shock Diseases 0.000 description 23
- 229910052943 magnesium sulfate Inorganic materials 0.000 description 23
- OYPRJOBELJOOCE-UHFFFAOYSA-N Calcium Chemical compound [Ca] OYPRJOBELJOOCE-UHFFFAOYSA-N 0.000 description 22
- 208000034158 bleeding Diseases 0.000 description 22
- 230000000740 bleeding effect Effects 0.000 description 22
- 229910052791 calcium Inorganic materials 0.000 description 22
- NIJJYAXOARWZEE-UHFFFAOYSA-N di-n-propyl-acetic acid Natural products CCCC(C(O)=O)CCC NIJJYAXOARWZEE-UHFFFAOYSA-N 0.000 description 22
- 230000000004 hemodynamic effect Effects 0.000 description 22
- MSRILKIQRXUYCT-UHFFFAOYSA-M valproate semisodium Chemical compound [Na+].CCCC(C(O)=O)CCC.CCCC(C([O-])=O)CCC MSRILKIQRXUYCT-UHFFFAOYSA-M 0.000 description 22
- 229960000604 valproic acid Drugs 0.000 description 22
- 239000003112 inhibitor Substances 0.000 description 21
- DGAQECJNVWCQMB-PUAWFVPOSA-M Ilexoside XXIX Chemical compound C[C@@H]1CC[C@@]2(CC[C@@]3(C(=CC[C@H]4[C@]3(CC[C@@H]5[C@@]4(CC[C@@H](C5(C)C)OS(=O)(=O)[O-])C)C)[C@@H]2[C@]1(C)O)C)C(=O)O[C@H]6[C@@H]([C@H]([C@@H]([C@H](O6)CO)O)O)O.[Na+] DGAQECJNVWCQMB-PUAWFVPOSA-M 0.000 description 20
- 229940127315 Potassium Channel Openers Drugs 0.000 description 20
- QVGXLLKOCUKJST-UHFFFAOYSA-N atomic oxygen Chemical compound [O] QVGXLLKOCUKJST-UHFFFAOYSA-N 0.000 description 20
- 229940079593 drug Drugs 0.000 description 20
- 238000002474 experimental method Methods 0.000 description 20
- 230000007246 mechanism Effects 0.000 description 20
- 239000001301 oxygen Substances 0.000 description 20
- 229910052760 oxygen Inorganic materials 0.000 description 20
- 239000011734 sodium Substances 0.000 description 20
- 208000015294 blood coagulation disease Diseases 0.000 description 19
- 230000034994 death Effects 0.000 description 19
- 231100000517 death Toxicity 0.000 description 19
- 208000028867 ischemia Diseases 0.000 description 19
- 229910052708 sodium Inorganic materials 0.000 description 19
- 229940083542 sodium Drugs 0.000 description 19
- 230000008733 trauma Effects 0.000 description 19
- 206010040070 Septic Shock Diseases 0.000 description 18
- 208000006011 Stroke Diseases 0.000 description 18
- 230000009471 action Effects 0.000 description 18
- 230000004872 arterial blood pressure Effects 0.000 description 18
- 239000000480 calcium channel blocker Substances 0.000 description 18
- 230000002631 hypothermal effect Effects 0.000 description 18
- 230000001976 improved effect Effects 0.000 description 18
- 230000036303 septic shock Effects 0.000 description 18
- 239000000758 substrate Substances 0.000 description 18
- 241000282414 Homo sapiens Species 0.000 description 17
- 210000001105 femoral artery Anatomy 0.000 description 17
- WQZGKKKJIJFFOK-GASJEMHNSA-N Glucose Natural products OC[C@H]1OC(O)[C@H](O)[C@@H](O)[C@@H]1O WQZGKKKJIJFFOK-GASJEMHNSA-N 0.000 description 16
- WQZGKKKJIJFFOK-VFUOTHLCSA-N beta-D-glucose Chemical compound OC[C@H]1O[C@@H](O)[C@H](O)[C@@H](O)[C@@H]1O WQZGKKKJIJFFOK-VFUOTHLCSA-N 0.000 description 16
- 239000008103 glucose Substances 0.000 description 16
- NOESYZHRGYRDHS-UHFFFAOYSA-N insulin Chemical compound N1C(=O)C(NC(=O)C(CCC(N)=O)NC(=O)C(CCC(O)=O)NC(=O)C(C(C)C)NC(=O)C(NC(=O)CN)C(C)CC)CSSCC(C(NC(CO)C(=O)NC(CC(C)C)C(=O)NC(CC=2C=CC(O)=CC=2)C(=O)NC(CCC(N)=O)C(=O)NC(CC(C)C)C(=O)NC(CCC(O)=O)C(=O)NC(CC(N)=O)C(=O)NC(CC=2C=CC(O)=CC=2)C(=O)NC(CSSCC(NC(=O)C(C(C)C)NC(=O)C(CC(C)C)NC(=O)C(CC=2C=CC(O)=CC=2)NC(=O)C(CC(C)C)NC(=O)C(C)NC(=O)C(CCC(O)=O)NC(=O)C(C(C)C)NC(=O)C(CC(C)C)NC(=O)C(CC=2NC=NC=2)NC(=O)C(CO)NC(=O)CNC2=O)C(=O)NCC(=O)NC(CCC(O)=O)C(=O)NC(CCCNC(N)=N)C(=O)NCC(=O)NC(CC=3C=CC=CC=3)C(=O)NC(CC=3C=CC=CC=3)C(=O)NC(CC=3C=CC(O)=CC=3)C(=O)NC(C(C)O)C(=O)N3C(CCC3)C(=O)NC(CCCCN)C(=O)NC(C)C(O)=O)C(=O)NC(CC(N)=O)C(O)=O)=O)NC(=O)C(C(C)CC)NC(=O)C(CO)NC(=O)C(C(C)O)NC(=O)C1CSSCC2NC(=O)C(CC(C)C)NC(=O)C(NC(=O)C(CCC(N)=O)NC(=O)C(CC(N)=O)NC(=O)C(NC(=O)C(N)CC=1C=CC=CC=1)C(C)C)CC1=CN=CN1 NOESYZHRGYRDHS-UHFFFAOYSA-N 0.000 description 16
- 229940005483 opioid analgesics Drugs 0.000 description 16
- 206010021143 Hypoxia Diseases 0.000 description 15
- 150000002576 ketones Chemical class 0.000 description 15
- 230000010412 perfusion Effects 0.000 description 15
- 230000000472 traumatic effect Effects 0.000 description 15
- RWSOTUBLDIXVET-UHFFFAOYSA-N Dihydrogen sulfide Chemical class S RWSOTUBLDIXVET-UHFFFAOYSA-N 0.000 description 14
- JLVVSXFLKOJNIY-UHFFFAOYSA-N Magnesium ion Chemical compound [Mg+2] JLVVSXFLKOJNIY-UHFFFAOYSA-N 0.000 description 14
- 230000007423 decrease Effects 0.000 description 14
- 208000037265 diseases, disorders, signs and symptoms Diseases 0.000 description 14
- 230000002757 inflammatory effect Effects 0.000 description 14
- 229910001425 magnesium ion Inorganic materials 0.000 description 14
- 230000035488 systolic blood pressure Effects 0.000 description 14
- 238000002560 therapeutic procedure Methods 0.000 description 14
- 108091006146 Channels Proteins 0.000 description 13
- 206010009192 Circulatory collapse Diseases 0.000 description 13
- 238000004458 analytical method Methods 0.000 description 13
- 210000001367 artery Anatomy 0.000 description 13
- 230000033228 biological regulation Effects 0.000 description 13
- 238000007675 cardiac surgery Methods 0.000 description 13
- 230000003247 decreasing effect Effects 0.000 description 13
- 238000007912 intraperitoneal administration Methods 0.000 description 13
- 210000003975 mesenteric artery Anatomy 0.000 description 13
- 102000005962 receptors Human genes 0.000 description 13
- 108020003175 receptors Proteins 0.000 description 13
- 230000002829 reductive effect Effects 0.000 description 13
- ZLMJMSJWJFRBEC-UHFFFAOYSA-N Potassium Chemical compound [K] ZLMJMSJWJFRBEC-UHFFFAOYSA-N 0.000 description 12
- 230000004087 circulation Effects 0.000 description 12
- DDRJAANPRJIHGJ-UHFFFAOYSA-N creatinine Chemical compound CN1CC(=O)NC1=N DDRJAANPRJIHGJ-UHFFFAOYSA-N 0.000 description 12
- 201000010099 disease Diseases 0.000 description 12
- 210000003038 endothelium Anatomy 0.000 description 12
- 239000012071 phase Substances 0.000 description 12
- 239000011591 potassium Substances 0.000 description 12
- 229960003975 potassium Drugs 0.000 description 12
- 229910052700 potassium Inorganic materials 0.000 description 12
- 230000008569 process Effects 0.000 description 12
- 239000003963 antioxidant agent Substances 0.000 description 11
- 235000006708 antioxidants Nutrition 0.000 description 11
- 230000002567 autonomic effect Effects 0.000 description 11
- 210000000133 brain stem Anatomy 0.000 description 11
- 230000003185 calcium uptake Effects 0.000 description 11
- 230000035602 clotting Effects 0.000 description 11
- 239000012530 fluid Substances 0.000 description 11
- 230000007954 hypoxia Effects 0.000 description 11
- 239000007924 injection Substances 0.000 description 11
- 238000002347 injection Methods 0.000 description 11
- 208000010125 myocardial infarction Diseases 0.000 description 11
- 230000001734 parasympathetic effect Effects 0.000 description 11
- 230000037361 pathway Effects 0.000 description 11
- 210000002381 plasma Anatomy 0.000 description 11
- 230000008439 repair process Effects 0.000 description 11
- 206010040560 shock Diseases 0.000 description 11
- 230000035882 stress Effects 0.000 description 11
- 230000032258 transport Effects 0.000 description 11
- 230000001515 vagal effect Effects 0.000 description 11
- 208000028399 Critical Illness Diseases 0.000 description 10
- ZSLZBFCDCINBPY-ZSJPKINUSA-N acetyl-CoA Chemical compound O[C@@H]1[C@H](OP(O)(O)=O)[C@@H](COP(O)(=O)OP(O)(=O)OCC(C)(C)[C@@H](O)C(=O)NCCC(=O)NCCSC(=O)C)O[C@H]1N1C2=NC=NC(N)=C2N=C1 ZSLZBFCDCINBPY-ZSJPKINUSA-N 0.000 description 10
- 206010003119 arrhythmia Diseases 0.000 description 10
- 230000008901 benefit Effects 0.000 description 10
- 230000017531 blood circulation Effects 0.000 description 10
- 230000036760 body temperature Effects 0.000 description 10
- 230000006931 brain damage Effects 0.000 description 10
- 231100000874 brain damage Toxicity 0.000 description 10
- 230000002612 cardiopulmonary effect Effects 0.000 description 10
- 230000001413 cellular effect Effects 0.000 description 10
- 238000002618 extracorporeal membrane oxygenation Methods 0.000 description 10
- 210000001035 gastrointestinal tract Anatomy 0.000 description 10
- 230000002401 inhibitory effect Effects 0.000 description 10
- 210000004072 lung Anatomy 0.000 description 10
- 238000005259 measurement Methods 0.000 description 10
- 230000004060 metabolic process Effects 0.000 description 10
- 229960004134 propofol Drugs 0.000 description 10
- OLBCVFGFOZPWHH-UHFFFAOYSA-N propofol Chemical compound CC(C)C1=CC=CC(C(C)C)=C1O OLBCVFGFOZPWHH-UHFFFAOYSA-N 0.000 description 10
- 230000000241 respiratory effect Effects 0.000 description 10
- 230000006641 stabilisation Effects 0.000 description 10
- 238000011105 stabilization Methods 0.000 description 10
- 230000004083 survival effect Effects 0.000 description 10
- 230000008961 swelling Effects 0.000 description 10
- PEDCQBHIVMGVHV-UHFFFAOYSA-N Glycerine Chemical compound OCC(O)CO PEDCQBHIVMGVHV-UHFFFAOYSA-N 0.000 description 9
- KCWZGJVSDFYRIX-YFKPBYRVSA-N N(gamma)-nitro-L-arginine methyl ester Chemical compound COC(=O)[C@@H](N)CCCN=C(N)N[N+]([O-])=O KCWZGJVSDFYRIX-YFKPBYRVSA-N 0.000 description 9
- 102000004257 Potassium Channel Human genes 0.000 description 9
- 108060008682 Tumor Necrosis Factor Proteins 0.000 description 9
- 102000000852 Tumor Necrosis Factor-alpha Human genes 0.000 description 9
- 238000007792 addition Methods 0.000 description 9
- 230000003110 anti-inflammatory effect Effects 0.000 description 9
- 210000000748 cardiovascular system Anatomy 0.000 description 9
- 230000003788 cerebral perfusion Effects 0.000 description 9
- 210000000038 chest Anatomy 0.000 description 9
- 239000000084 colloidal system Substances 0.000 description 9
- 238000007906 compression Methods 0.000 description 9
- 230000006835 compression Effects 0.000 description 9
- 231100000673 dose–response relationship Toxicity 0.000 description 9
- 210000003734 kidney Anatomy 0.000 description 9
- 230000002980 postoperative effect Effects 0.000 description 9
- 108020001213 potassium channel Proteins 0.000 description 9
- 230000002633 protecting effect Effects 0.000 description 9
- 238000013222 sprague-dawley male rat Methods 0.000 description 9
- HTTJABKRGRZYRN-UHFFFAOYSA-N Heparin Chemical compound OC1C(NC(=O)C)C(O)OC(COS(O)(=O)=O)C1OC1C(OS(O)(=O)=O)C(O)C(OC2C(C(OS(O)(=O)=O)C(OC3C(C(O)C(O)C(O3)C(O)=O)OS(O)(=O)=O)C(CO)O2)NS(O)(=O)=O)C(C(O)=O)O1 HTTJABKRGRZYRN-UHFFFAOYSA-N 0.000 description 8
- 102000004877 Insulin Human genes 0.000 description 8
- 108090001061 Insulin Proteins 0.000 description 8
- 102000016924 KATP Channels Human genes 0.000 description 8
- 108010053914 KATP Channels Proteins 0.000 description 8
- CSNNHWWHGAXBCP-UHFFFAOYSA-L Magnesium sulfate Chemical compound [Mg+2].[O-][S+2]([O-])([O-])[O-] CSNNHWWHGAXBCP-UHFFFAOYSA-L 0.000 description 8
- 206010063837 Reperfusion injury Diseases 0.000 description 8
- 241000282898 Sus scrofa Species 0.000 description 8
- 102100040247 Tumor necrosis factor Human genes 0.000 description 8
- 210000002376 aorta thoracic Anatomy 0.000 description 8
- 230000006793 arrhythmia Effects 0.000 description 8
- 230000009286 beneficial effect Effects 0.000 description 8
- 230000002490 cerebral effect Effects 0.000 description 8
- 229940125396 insulin Drugs 0.000 description 8
- 210000003470 mitochondria Anatomy 0.000 description 8
- 230000001681 protective effect Effects 0.000 description 8
- 238000011552 rat model Methods 0.000 description 8
- 238000012360 testing method Methods 0.000 description 8
- AWLILQARPMWUHA-UHFFFAOYSA-M thiopental sodium Chemical compound [Na+].CCCC(C)C1(CC)C(=O)NC([S-])=NC1=O AWLILQARPMWUHA-UHFFFAOYSA-M 0.000 description 8
- 239000003981 vehicle Substances 0.000 description 8
- JWZZKOKVBUJMES-UHFFFAOYSA-N (+-)-Isoprenaline Chemical compound CC(C)NCC(O)C1=CC=C(O)C(O)=C1 JWZZKOKVBUJMES-UHFFFAOYSA-N 0.000 description 7
- SGTNSNPWRIOYBX-UHFFFAOYSA-N 2-(3,4-dimethoxyphenyl)-5-{[2-(3,4-dimethoxyphenyl)ethyl](methyl)amino}-2-(propan-2-yl)pentanenitrile Chemical compound C1=C(OC)C(OC)=CC=C1CCN(C)CCCC(C#N)(C(C)C)C1=CC=C(OC)C(OC)=C1 SGTNSNPWRIOYBX-UHFFFAOYSA-N 0.000 description 7
- 206010048962 Brain oedema Diseases 0.000 description 7
- 102000004127 Cytokines Human genes 0.000 description 7
- 108090000695 Cytokines Proteins 0.000 description 7
- 102000009123 Fibrin Human genes 0.000 description 7
- 108010073385 Fibrin Proteins 0.000 description 7
- BWGVNKXGVNDBDI-UHFFFAOYSA-N Fibrin monomer Chemical compound CNC(=O)CNC(=O)CN BWGVNKXGVNDBDI-UHFFFAOYSA-N 0.000 description 7
- 206010019280 Heart failures Diseases 0.000 description 7
- 206010028980 Neoplasm Diseases 0.000 description 7
- 208000018525 Postpartum Hemorrhage Diseases 0.000 description 7
- 206010058151 Pulseless electrical activity Diseases 0.000 description 7
- 108010000499 Thromboplastin Proteins 0.000 description 7
- 102000002262 Thromboplastin Human genes 0.000 description 7
- 230000005856 abnormality Effects 0.000 description 7
- 230000004913 activation Effects 0.000 description 7
- 208000006752 brain edema Diseases 0.000 description 7
- 206010007625 cardiogenic shock Diseases 0.000 description 7
- 230000001419 dependent effect Effects 0.000 description 7
- 229960004042 diazoxide Drugs 0.000 description 7
- 235000014113 dietary fatty acids Nutrition 0.000 description 7
- 230000002526 effect on cardiovascular system Effects 0.000 description 7
- 229930195729 fatty acid Natural products 0.000 description 7
- 239000000194 fatty acid Substances 0.000 description 7
- 150000004665 fatty acids Chemical class 0.000 description 7
- 229950003499 fibrin Drugs 0.000 description 7
- 229960002897 heparin Drugs 0.000 description 7
- 229920000669 heparin Polymers 0.000 description 7
- 229910052739 hydrogen Inorganic materials 0.000 description 7
- 210000002414 leg Anatomy 0.000 description 7
- 238000004519 manufacturing process Methods 0.000 description 7
- XONPDZSGENTBNJ-UHFFFAOYSA-N molecular hydrogen;sodium Chemical group [Na].[H][H] XONPDZSGENTBNJ-UHFFFAOYSA-N 0.000 description 7
- 238000012544 monitoring process Methods 0.000 description 7
- HYIMSNHJOBLJNT-UHFFFAOYSA-N nifedipine Chemical compound COC(=O)C1=C(C)NC(C)=C(C(=O)OC)C1C1=CC=CC=C1[N+]([O-])=O HYIMSNHJOBLJNT-UHFFFAOYSA-N 0.000 description 7
- 230000000144 pharmacologic effect Effects 0.000 description 7
- 238000011084 recovery Methods 0.000 description 7
- 230000010410 reperfusion Effects 0.000 description 7
- 239000000523 sample Substances 0.000 description 7
- 231100000611 venom Toxicity 0.000 description 7
- 230000002861 ventricular Effects 0.000 description 7
- MZOFCQQQCNRIBI-VMXHOPILSA-N (3s)-4-[[(2s)-1-[[(2s)-1-[[(1s)-1-carboxy-2-hydroxyethyl]amino]-4-methyl-1-oxopentan-2-yl]amino]-5-(diaminomethylideneamino)-1-oxopentan-2-yl]amino]-3-[[2-[[(2s)-2,6-diaminohexanoyl]amino]acetyl]amino]-4-oxobutanoic acid Chemical compound OC[C@@H](C(O)=O)NC(=O)[C@H](CC(C)C)NC(=O)[C@H](CCCN=C(N)N)NC(=O)[C@H](CC(O)=O)NC(=O)CNC(=O)[C@@H](N)CCCCN MZOFCQQQCNRIBI-VMXHOPILSA-N 0.000 description 6
- CIWBSHSKHKDKBQ-JLAZNSOCSA-N Ascorbic acid Chemical compound OC[C@H](O)[C@H]1OC(=O)C(O)=C1O CIWBSHSKHKDKBQ-JLAZNSOCSA-N 0.000 description 6
- 241000282412 Homo Species 0.000 description 6
- 102000004016 L-Type Calcium Channels Human genes 0.000 description 6
- 108090000420 L-Type Calcium Channels Proteins 0.000 description 6
- 102000003840 Opioid Receptors Human genes 0.000 description 6
- 108090000137 Opioid Receptors Proteins 0.000 description 6
- 230000001154 acute effect Effects 0.000 description 6
- 239000005557 antagonist Substances 0.000 description 6
- 230000003288 anthiarrhythmic effect Effects 0.000 description 6
- 230000003078 antioxidant effect Effects 0.000 description 6
- 239000002876 beta blocker Substances 0.000 description 6
- 229940097320 beta blocking agent Drugs 0.000 description 6
- 210000004204 blood vessel Anatomy 0.000 description 6
- 230000003925 brain function Effects 0.000 description 6
- 238000001816 cooling Methods 0.000 description 6
- 229940109239 creatinine Drugs 0.000 description 6
- 230000035487 diastolic blood pressure Effects 0.000 description 6
- 229960002768 dipyridamole Drugs 0.000 description 6
- IZEKFCXSFNUWAM-UHFFFAOYSA-N dipyridamole Chemical compound C=12N=C(N(CCO)CCO)N=C(N3CCCCC3)C2=NC(N(CCO)CCO)=NC=1N1CCCCC1 IZEKFCXSFNUWAM-UHFFFAOYSA-N 0.000 description 6
- 210000003191 femoral vein Anatomy 0.000 description 6
- 239000001257 hydrogen Substances 0.000 description 6
- 201000001421 hyperglycemia Diseases 0.000 description 6
- 239000007788 liquid Substances 0.000 description 6
- 239000003550 marker Substances 0.000 description 6
- 230000001404 mediated effect Effects 0.000 description 6
- 229960001597 nifedipine Drugs 0.000 description 6
- 238000002360 preparation method Methods 0.000 description 6
- 230000029058 respiratory gaseous exchange Effects 0.000 description 6
- 238000012552 review Methods 0.000 description 6
- 239000000126 substance Substances 0.000 description 6
- 230000002889 sympathetic effect Effects 0.000 description 6
- 208000011580 syndromic disease Diseases 0.000 description 6
- 230000009885 systemic effect Effects 0.000 description 6
- 239000003053 toxin Substances 0.000 description 6
- 231100000765 toxin Toxicity 0.000 description 6
- 108700012359 toxins Proteins 0.000 description 6
- 230000008736 traumatic injury Effects 0.000 description 6
- 208000001072 type 2 diabetes mellitus Diseases 0.000 description 6
- 210000001364 upper extremity Anatomy 0.000 description 6
- 210000002700 urine Anatomy 0.000 description 6
- 229960001722 verapamil Drugs 0.000 description 6
- 206010003497 Asphyxia Diseases 0.000 description 5
- 208000003322 Coinfection Diseases 0.000 description 5
- 206010010071 Coma Diseases 0.000 description 5
- 108010092674 Enkephalins Proteins 0.000 description 5
- 102000006587 Glutathione peroxidase Human genes 0.000 description 5
- 108700016172 Glutathione peroxidases Proteins 0.000 description 5
- 108010033040 Histones Proteins 0.000 description 5
- 206010020772 Hypertension Diseases 0.000 description 5
- 206010022489 Insulin Resistance Diseases 0.000 description 5
- JVTAAEKCZFNVCJ-UHFFFAOYSA-M Lactate Chemical compound CC(O)C([O-])=O JVTAAEKCZFNVCJ-UHFFFAOYSA-M 0.000 description 5
- URLZCHNOLZSCCA-VABKMULXSA-N Leu-enkephalin Chemical compound C([C@@H](C(=O)N[C@@H](CC(C)C)C(O)=O)NC(=O)CNC(=O)CNC(=O)[C@@H](N)CC=1C=CC(O)=CC=1)C1=CC=CC=C1 URLZCHNOLZSCCA-VABKMULXSA-N 0.000 description 5
- 206010030113 Oedema Diseases 0.000 description 5
- 239000002202 Polyethylene glycol Substances 0.000 description 5
- LCTONWCANYUPML-UHFFFAOYSA-M Pyruvate Chemical compound CC(=O)C([O-])=O LCTONWCANYUPML-UHFFFAOYSA-M 0.000 description 5
- 229930006000 Sucrose Natural products 0.000 description 5
- CZMRCDWAGMRECN-UGDNZRGBSA-N Sucrose Chemical compound O[C@H]1[C@H](O)[C@@H](CO)O[C@@]1(CO)O[C@@H]1[C@H](O)[C@@H](O)[C@H](O)[C@@H](CO)O1 CZMRCDWAGMRECN-UGDNZRGBSA-N 0.000 description 5
- 208000007536 Thrombosis Diseases 0.000 description 5
- 208000003443 Unconsciousness Diseases 0.000 description 5
- 230000015572 biosynthetic process Effects 0.000 description 5
- 210000001124 body fluid Anatomy 0.000 description 5
- 210000002168 brachiocephalic trunk Anatomy 0.000 description 5
- 210000000170 cell membrane Anatomy 0.000 description 5
- 230000001684 chronic effect Effects 0.000 description 5
- 230000009089 cytolysis Effects 0.000 description 5
- 230000003111 delayed effect Effects 0.000 description 5
- 238000010790 dilution Methods 0.000 description 5
- 239000012895 dilution Substances 0.000 description 5
- 230000004064 dysfunction Effects 0.000 description 5
- 230000004217 heart function Effects 0.000 description 5
- 230000006872 improvement Effects 0.000 description 5
- 230000028709 inflammatory response Effects 0.000 description 5
- 208000037906 ischaemic injury Diseases 0.000 description 5
- 208000012947 ischemia reperfusion injury Diseases 0.000 description 5
- 230000000302 ischemic effect Effects 0.000 description 5
- 231100000518 lethal Toxicity 0.000 description 5
- 230000001665 lethal effect Effects 0.000 description 5
- 230000000670 limiting effect Effects 0.000 description 5
- 210000004379 membrane Anatomy 0.000 description 5
- 239000012528 membrane Substances 0.000 description 5
- 210000001700 mitochondrial membrane Anatomy 0.000 description 5
- 210000000107 myocyte Anatomy 0.000 description 5
- 210000005036 nerve Anatomy 0.000 description 5
- 230000009251 neurologic dysfunction Effects 0.000 description 5
- 208000015015 neurological dysfunction Diseases 0.000 description 5
- 210000002569 neuron Anatomy 0.000 description 5
- LBHIOVVIQHSOQN-UHFFFAOYSA-N nicorandil Chemical compound [O-][N+](=O)OCCNC(=O)C1=CC=CN=C1 LBHIOVVIQHSOQN-UHFFFAOYSA-N 0.000 description 5
- 229960002497 nicorandil Drugs 0.000 description 5
- 230000010355 oscillation Effects 0.000 description 5
- 210000002963 paraventricular hypothalamic nucleus Anatomy 0.000 description 5
- 230000036961 partial effect Effects 0.000 description 5
- 239000000137 peptide hydrolase inhibitor Substances 0.000 description 5
- 229920001223 polyethylene glycol Polymers 0.000 description 5
- 238000004321 preservation Methods 0.000 description 5
- 239000000047 product Substances 0.000 description 5
- 108090000623 proteins and genes Proteins 0.000 description 5
- 229940044601 receptor agonist Drugs 0.000 description 5
- 239000000018 receptor agonist Substances 0.000 description 5
- 230000004044 response Effects 0.000 description 5
- 239000003195 sodium channel blocking agent Substances 0.000 description 5
- 230000002269 spontaneous effect Effects 0.000 description 5
- 239000005720 sucrose Substances 0.000 description 5
- 239000004094 surface-active agent Substances 0.000 description 5
- 239000000725 suspension Substances 0.000 description 5
- 230000002459 sustained effect Effects 0.000 description 5
- 230000001225 therapeutic effect Effects 0.000 description 5
- 239000002435 venom Substances 0.000 description 5
- 210000001048 venom Anatomy 0.000 description 5
- PGOHTUIFYSHAQG-LJSDBVFPSA-N (2S)-6-amino-2-[[(2S)-5-amino-2-[[(2S)-2-[[(2S)-2-[[(2S)-2-[[(2S)-4-amino-2-[[(2S)-2-[[(2S)-2-[[(2S)-2-[[(2S)-2-[[(2S)-5-amino-2-[[(2S)-5-amino-2-[[(2S)-2-[[(2S)-2-[[(2S)-2-[[(2S,3R)-2-[[(2S)-5-amino-2-[[(2S)-2-[[(2S)-2-[[(2S,3R)-2-[[(2S)-2-[[(2S)-2-[[(2S)-2-[[(2S)-2-[[(2S)-5-amino-2-[[(2S)-1-[(2S,3R)-2-[[(2S)-2-[[(2S)-2-[[(2R)-2-[[(2S)-2-[[(2S)-2-[[2-[[(2S)-2-[[(2S)-2-[[(2S)-2-[[(2S)-1-[(2S)-2-[[(2S)-2-[[(2S)-2-[[(2S)-2-amino-4-methylsulfanylbutanoyl]amino]-3-(1H-indol-3-yl)propanoyl]amino]-5-carbamimidamidopentanoyl]amino]propanoyl]pyrrolidine-2-carbonyl]amino]-3-methylbutanoyl]amino]-4-methylpentanoyl]amino]-4-methylpentanoyl]amino]acetyl]amino]-3-hydroxypropanoyl]amino]-4-methylpentanoyl]amino]-3-sulfanylpropanoyl]amino]-4-methylsulfanylbutanoyl]amino]-5-carbamimidamidopentanoyl]amino]-3-hydroxybutanoyl]pyrrolidine-2-carbonyl]amino]-5-oxopentanoyl]amino]-3-hydroxypropanoyl]amino]-3-hydroxypropanoyl]amino]-3-(1H-imidazol-5-yl)propanoyl]amino]-4-methylpentanoyl]amino]-3-hydroxybutanoyl]amino]-3-(1H-indol-3-yl)propanoyl]amino]-5-carbamimidamidopentanoyl]amino]-5-oxopentanoyl]amino]-3-hydroxybutanoyl]amino]-3-hydroxypropanoyl]amino]-3-carboxypropanoyl]amino]-3-hydroxypropanoyl]amino]-5-oxopentanoyl]amino]-5-oxopentanoyl]amino]-3-phenylpropanoyl]amino]-5-carbamimidamidopentanoyl]amino]-3-methylbutanoyl]amino]-4-methylpentanoyl]amino]-4-oxobutanoyl]amino]-5-carbamimidamidopentanoyl]amino]-3-(1H-indol-3-yl)propanoyl]amino]-4-carboxybutanoyl]amino]-5-oxopentanoyl]amino]hexanoic acid Chemical compound CSCC[C@H](N)C(=O)N[C@@H](Cc1c[nH]c2ccccc12)C(=O)N[C@@H](CCCNC(N)=N)C(=O)N[C@@H](C)C(=O)N1CCC[C@H]1C(=O)N[C@@H](C(C)C)C(=O)N[C@@H](CC(C)C)C(=O)N[C@@H](CC(C)C)C(=O)NCC(=O)N[C@@H](CO)C(=O)N[C@@H](CC(C)C)C(=O)N[C@@H](CS)C(=O)N[C@@H](CCSC)C(=O)N[C@@H](CCCNC(N)=N)C(=O)N[C@@H]([C@@H](C)O)C(=O)N1CCC[C@H]1C(=O)N[C@@H](CCC(N)=O)C(=O)N[C@@H](CO)C(=O)N[C@@H](CO)C(=O)N[C@@H](Cc1cnc[nH]1)C(=O)N[C@@H](CC(C)C)C(=O)N[C@@H]([C@@H](C)O)C(=O)N[C@@H](Cc1c[nH]c2ccccc12)C(=O)N[C@@H](CCCNC(N)=N)C(=O)N[C@@H](CCC(N)=O)C(=O)N[C@@H]([C@@H](C)O)C(=O)N[C@@H](CO)C(=O)N[C@@H](CC(O)=O)C(=O)N[C@@H](CO)C(=O)N[C@@H](CCC(N)=O)C(=O)N[C@@H](CCC(N)=O)C(=O)N[C@@H](Cc1ccccc1)C(=O)N[C@@H](CCCNC(N)=N)C(=O)N[C@@H](C(C)C)C(=O)N[C@@H](CC(C)C)C(=O)N[C@@H](CC(N)=O)C(=O)N[C@@H](CCCNC(N)=N)C(=O)N[C@@H](Cc1c[nH]c2ccccc12)C(=O)N[C@@H](CCC(O)=O)C(=O)N[C@@H](CCC(N)=O)C(=O)N[C@@H](CCCCN)C(O)=O PGOHTUIFYSHAQG-LJSDBVFPSA-N 0.000 description 4
- GVJHHUAWPYXKBD-UHFFFAOYSA-N (±)-α-Tocopherol Chemical compound OC1=C(C)C(C)=C2OC(CCCC(C)CCCC(C)CCCC(C)C)(C)CCC2=C1C GVJHHUAWPYXKBD-UHFFFAOYSA-N 0.000 description 4
- 241000700199 Cavia porcellus Species 0.000 description 4
- MYMOFIZGZYHOMD-UHFFFAOYSA-N Dioxygen Chemical compound O=O MYMOFIZGZYHOMD-UHFFFAOYSA-N 0.000 description 4
- 206010061216 Infarction Diseases 0.000 description 4
- 108091005975 Myofilaments Proteins 0.000 description 4
- 241000242583 Scyphozoa Species 0.000 description 4
- 108010052164 Sodium Channels Proteins 0.000 description 4
- 102000018674 Sodium Channels Human genes 0.000 description 4
- 230000036982 action potential Effects 0.000 description 4
- 230000002411 adverse Effects 0.000 description 4
- 239000000443 aerosol Substances 0.000 description 4
- 229940044094 angiotensin-converting-enzyme inhibitor Drugs 0.000 description 4
- 208000007474 aortic aneurysm Diseases 0.000 description 4
- 239000007900 aqueous suspension Substances 0.000 description 4
- 239000002473 artificial blood Substances 0.000 description 4
- 230000001580 bacterial effect Effects 0.000 description 4
- 230000035581 baroreflex Effects 0.000 description 4
- 238000003287 bathing Methods 0.000 description 4
- 230000000903 blocking effect Effects 0.000 description 4
- 239000010836 blood and blood product Substances 0.000 description 4
- 229940125691 blood product Drugs 0.000 description 4
- 230000037396 body weight Effects 0.000 description 4
- 239000000969 carrier Substances 0.000 description 4
- 230000005779 cell damage Effects 0.000 description 4
- 208000037887 cell injury Diseases 0.000 description 4
- 239000007859 condensation product Substances 0.000 description 4
- 238000011161 development Methods 0.000 description 4
- 230000018109 developmental process Effects 0.000 description 4
- HSUGRBWQSSZJOP-RTWAWAEBSA-N diltiazem Chemical compound C1=CC(OC)=CC=C1[C@H]1[C@@H](OC(C)=O)C(=O)N(CCN(C)C)C2=CC=CC=C2S1 HSUGRBWQSSZJOP-RTWAWAEBSA-N 0.000 description 4
- 229960004166 diltiazem Drugs 0.000 description 4
- 229910001882 dioxygen Inorganic materials 0.000 description 4
- 229940042399 direct acting antivirals protease inhibitors Drugs 0.000 description 4
- 208000009190 disseminated intravascular coagulation Diseases 0.000 description 4
- 210000002889 endothelial cell Anatomy 0.000 description 4
- 150000002148 esters Chemical class 0.000 description 4
- 210000002865 immune cell Anatomy 0.000 description 4
- 238000001727 in vivo Methods 0.000 description 4
- 230000007574 infarction Effects 0.000 description 4
- 230000003993 interaction Effects 0.000 description 4
- 239000000543 intermediate Substances 0.000 description 4
- AGBQKNBQESQNJD-UHFFFAOYSA-N lipoic acid Chemical compound OC(=O)CCCCC1CCSS1 AGBQKNBQESQNJD-UHFFFAOYSA-N 0.000 description 4
- 210000004185 liver Anatomy 0.000 description 4
- 235000019341 magnesium sulphate Nutrition 0.000 description 4
- 238000007726 management method Methods 0.000 description 4
- 210000003632 microfilament Anatomy 0.000 description 4
- 230000001537 neural effect Effects 0.000 description 4
- 239000008194 pharmaceutical composition Substances 0.000 description 4
- 230000036470 plasma concentration Effects 0.000 description 4
- 231100000614 poison Toxicity 0.000 description 4
- 239000002574 poison Substances 0.000 description 4
- 231100000572 poisoning Toxicity 0.000 description 4
- 230000000607 poisoning effect Effects 0.000 description 4
- 239000003755 preservative agent Substances 0.000 description 4
- 239000002516 radical scavenger Substances 0.000 description 4
- 239000003642 reactive oxygen metabolite Substances 0.000 description 4
- 230000009467 reduction Effects 0.000 description 4
- 230000002441 reversible effect Effects 0.000 description 4
- 239000000375 suspending agent Substances 0.000 description 4
- 230000002791 sympathovagal effect Effects 0.000 description 4
- 230000004873 systolic arterial blood pressure Effects 0.000 description 4
- XOAAWQZATWQOTB-UHFFFAOYSA-N taurine Chemical compound NCCS(O)(=O)=O XOAAWQZATWQOTB-UHFFFAOYSA-N 0.000 description 4
- 238000011269 treatment regimen Methods 0.000 description 4
- 230000004102 tricarboxylic acid cycle Effects 0.000 description 4
- 230000002485 urinary effect Effects 0.000 description 4
- 210000003462 vein Anatomy 0.000 description 4
- HDTRYLNUVZCQOY-UHFFFAOYSA-N α-D-glucopyranosyl-α-D-glucopyranoside Natural products OC1C(O)C(O)C(CO)OC1OC1C(O)C(O)C(O)C(CO)O1 HDTRYLNUVZCQOY-UHFFFAOYSA-N 0.000 description 3
- 230000002407 ATP formation Effects 0.000 description 3
- CSCPPACGZOOCGX-UHFFFAOYSA-N Acetone Chemical compound CC(C)=O CSCPPACGZOOCGX-UHFFFAOYSA-N 0.000 description 3
- 208000010444 Acidosis Diseases 0.000 description 3
- 208000024827 Alzheimer disease Diseases 0.000 description 3
- 241000894006 Bacteria Species 0.000 description 3
- 208000035143 Bacterial infection Diseases 0.000 description 3
- 108010074051 C-Reactive Protein Proteins 0.000 description 3
- 102100032752 C-reactive protein Human genes 0.000 description 3
- 206010010904 Convulsion Diseases 0.000 description 3
- FBPFZTCFMRRESA-FSIIMWSLSA-N D-Glucitol Natural products OC[C@H](O)[C@H](O)[C@@H](O)[C@H](O)CO FBPFZTCFMRRESA-FSIIMWSLSA-N 0.000 description 3
- FBPFZTCFMRRESA-JGWLITMVSA-N D-glucitol Chemical compound OC[C@H](O)[C@@H](O)[C@H](O)[C@H](O)CO FBPFZTCFMRRESA-JGWLITMVSA-N 0.000 description 3
- 208000002230 Diabetic coma Diseases 0.000 description 3
- 108010065372 Dynorphins Proteins 0.000 description 3
- 239000004150 EU approved colour Substances 0.000 description 3
- 108010049140 Endorphins Proteins 0.000 description 3
- 102000009025 Endorphins Human genes 0.000 description 3
- 102000004190 Enzymes Human genes 0.000 description 3
- 108090000790 Enzymes Proteins 0.000 description 3
- IAYPIBMASNFSPL-UHFFFAOYSA-N Ethylene oxide Chemical compound C1CO1 IAYPIBMASNFSPL-UHFFFAOYSA-N 0.000 description 3
- 102000001554 Hemoglobins Human genes 0.000 description 3
- 108010054147 Hemoglobins Proteins 0.000 description 3
- 102000006947 Histones Human genes 0.000 description 3
- 101000843809 Homo sapiens Hydroxycarboxylic acid receptor 2 Proteins 0.000 description 3
- 102100030643 Hydroxycarboxylic acid receptor 2 Human genes 0.000 description 3
- 208000013016 Hypoglycemia Diseases 0.000 description 3
- 206010058558 Hypoperfusion Diseases 0.000 description 3
- 206010062016 Immunosuppression Diseases 0.000 description 3
- 108090001005 Interleukin-6 Proteins 0.000 description 3
- 102000004889 Interleukin-6 Human genes 0.000 description 3
- 208000018737 Parkinson disease Diseases 0.000 description 3
- 229940127343 Potassium Channel Agonists Drugs 0.000 description 3
- DNIAPMSPPWPWGF-UHFFFAOYSA-N Propylene glycol Chemical compound CC(O)CO DNIAPMSPPWPWGF-UHFFFAOYSA-N 0.000 description 3
- 101800004937 Protein C Proteins 0.000 description 3
- 102000017975 Protein C Human genes 0.000 description 3
- 101100244562 Pseudomonas aeruginosa (strain ATCC 15692 / DSM 22644 / CIP 104116 / JCM 14847 / LMG 12228 / 1C / PRS 101 / PAO1) oprD gene Proteins 0.000 description 3
- 108090000583 R-Type Calcium Channels Proteins 0.000 description 3
- 102000004059 R-Type Calcium Channels Human genes 0.000 description 3
- 101800001700 Saposin-D Proteins 0.000 description 3
- NINIDFKCEFEMDL-UHFFFAOYSA-N Sulfur Chemical compound [S] NINIDFKCEFEMDL-UHFFFAOYSA-N 0.000 description 3
- UCKMPCXJQFINFW-UHFFFAOYSA-N Sulphide Chemical compound [S-2] UCKMPCXJQFINFW-UHFFFAOYSA-N 0.000 description 3
- 239000005864 Sulphur Substances 0.000 description 3
- 241000239292 Theraphosidae Species 0.000 description 3
- HDTRYLNUVZCQOY-WSWWMNSNSA-N Trehalose Natural products O[C@@H]1[C@@H](O)[C@@H](O)[C@@H](CO)O[C@@H]1O[C@@H]1[C@H](O)[C@@H](O)[C@@H](O)[C@@H](CO)O1 HDTRYLNUVZCQOY-WSWWMNSNSA-N 0.000 description 3
- 108090001027 Troponin Proteins 0.000 description 3
- 102000004903 Troponin Human genes 0.000 description 3
- XSQUKJJJFZCRTK-UHFFFAOYSA-N Urea Chemical compound NC(N)=O XSQUKJJJFZCRTK-UHFFFAOYSA-N 0.000 description 3
- 206010047700 Vomiting Diseases 0.000 description 3
- 206010052428 Wound Diseases 0.000 description 3
- 210000000683 abdominal cavity Anatomy 0.000 description 3
- 230000021736 acetylation Effects 0.000 description 3
- 238000006640 acetylation reaction Methods 0.000 description 3
- 239000002253 acid Substances 0.000 description 3
- 239000004480 active ingredient Substances 0.000 description 3
- HDTRYLNUVZCQOY-LIZSDCNHSA-N alpha,alpha-trehalose Chemical compound O[C@@H]1[C@@H](O)[C@H](O)[C@@H](CO)O[C@@H]1O[C@@H]1[C@H](O)[C@@H](O)[C@H](O)[C@@H](CO)O1 HDTRYLNUVZCQOY-LIZSDCNHSA-N 0.000 description 3
- XSDQTOBWRPYKKA-UHFFFAOYSA-N amiloride Chemical compound NC(=N)NC(=O)C1=NC(Cl)=C(N)N=C1N XSDQTOBWRPYKKA-UHFFFAOYSA-N 0.000 description 3
- 229960002576 amiloride Drugs 0.000 description 3
- 229940024606 amino acid Drugs 0.000 description 3
- 235000001014 amino acid Nutrition 0.000 description 3
- 150000003862 amino acid derivatives Chemical class 0.000 description 3
- 150000001413 amino acids Chemical class 0.000 description 3
- 230000001466 anti-adreneric effect Effects 0.000 description 3
- 239000004019 antithrombin Substances 0.000 description 3
- 210000000709 aorta Anatomy 0.000 description 3
- 208000022362 bacterial infectious disease Diseases 0.000 description 3
- 230000006399 behavior Effects 0.000 description 3
- 229960003665 bepridil Drugs 0.000 description 3
- UIEATEWHFDRYRU-UHFFFAOYSA-N bepridil Chemical compound C1CCCN1C(COCC(C)C)CN(C=1C=CC=CC=1)CC1=CC=CC=C1 UIEATEWHFDRYRU-UHFFFAOYSA-N 0.000 description 3
- 230000008499 blood brain barrier function Effects 0.000 description 3
- 230000008061 calcium-channel-blocking effect Effects 0.000 description 3
- 230000005961 cardioprotection Effects 0.000 description 3
- 230000015556 catabolic process Effects 0.000 description 3
- 210000004534 cecum Anatomy 0.000 description 3
- 230000030833 cell death Effects 0.000 description 3
- 230000004656 cell transport Effects 0.000 description 3
- 210000003169 central nervous system Anatomy 0.000 description 3
- 230000008859 change Effects 0.000 description 3
- 230000035606 childbirth Effects 0.000 description 3
- 230000001713 cholinergic effect Effects 0.000 description 3
- KRKNYBCHXYNGOX-UHFFFAOYSA-N citric acid Chemical compound OC(=O)CC(O)(C(O)=O)CC(O)=O KRKNYBCHXYNGOX-UHFFFAOYSA-N 0.000 description 3
- 230000008602 contraction Effects 0.000 description 3
- 239000006071 cream Substances 0.000 description 3
- 230000001120 cytoprotective effect Effects 0.000 description 3
- 230000006735 deficit Effects 0.000 description 3
- 108700023159 delta Opioid Receptors Proteins 0.000 description 3
- 102000048124 delta Opioid Receptors Human genes 0.000 description 3
- 230000002074 deregulated effect Effects 0.000 description 3
- 206010012601 diabetes mellitus Diseases 0.000 description 3
- 230000004882 diastolic arterial blood pressure Effects 0.000 description 3
- 239000002270 dispersing agent Substances 0.000 description 3
- 206010014599 encephalitis Diseases 0.000 description 3
- 229940088598 enzyme Drugs 0.000 description 3
- AQNDDEOPVVGCPG-UHFFFAOYSA-N esmolol Chemical compound COC(=O)CCC1=CC=C(OCC(O)CNC(C)C)C=C1 AQNDDEOPVVGCPG-UHFFFAOYSA-N 0.000 description 3
- 229960003745 esmolol Drugs 0.000 description 3
- 239000000796 flavoring agent Substances 0.000 description 3
- 230000034659 glycolysis Effects 0.000 description 3
- 230000009931 harmful effect Effects 0.000 description 3
- 210000002064 heart cell Anatomy 0.000 description 3
- 230000002008 hemorrhagic effect Effects 0.000 description 3
- 229940121372 histone deacetylase inhibitor Drugs 0.000 description 3
- 239000003276 histone deacetylase inhibitor Substances 0.000 description 3
- 229910000037 hydrogen sulfide Inorganic materials 0.000 description 3
- 230000002218 hypoglycaemic effect Effects 0.000 description 3
- 230000036737 immune function Effects 0.000 description 3
- 230000001506 immunosuppresive effect Effects 0.000 description 3
- 230000005764 inhibitory process Effects 0.000 description 3
- 230000003834 intracellular effect Effects 0.000 description 3
- 238000007917 intracranial administration Methods 0.000 description 3
- 150000002500 ions Chemical class 0.000 description 3
- 210000000265 leukocyte Anatomy 0.000 description 3
- 238000011068 loading method Methods 0.000 description 3
- 230000002438 mitochondrial effect Effects 0.000 description 3
- 210000003205 muscle Anatomy 0.000 description 3
- 210000000653 nervous system Anatomy 0.000 description 3
- 230000000926 neurological effect Effects 0.000 description 3
- 210000000440 neutrophil Anatomy 0.000 description 3
- 229940006093 opthalmologic coloring agent diagnostic Drugs 0.000 description 3
- 230000003647 oxidation Effects 0.000 description 3
- 238000007254 oxidation reaction Methods 0.000 description 3
- 230000036542 oxidative stress Effects 0.000 description 3
- 239000000546 pharmaceutical excipient Substances 0.000 description 3
- 125000001997 phenyl group Chemical group [H]C1=C([H])C([H])=C(*)C([H])=C1[H] 0.000 description 3
- 230000029279 positive regulation of transcription, DNA-dependent Effects 0.000 description 3
- 239000000843 powder Substances 0.000 description 3
- 230000002250 progressing effect Effects 0.000 description 3
- 230000000770 proinflammatory effect Effects 0.000 description 3
- 230000001737 promoting effect Effects 0.000 description 3
- 229960000856 protein c Drugs 0.000 description 3
- 239000002464 receptor antagonist Substances 0.000 description 3
- 229940044551 receptor antagonist Drugs 0.000 description 3
- 230000029865 regulation of blood pressure Effects 0.000 description 3
- 230000001105 regulatory effect Effects 0.000 description 3
- 230000035945 sensitivity Effects 0.000 description 3
- 238000004904 shortening Methods 0.000 description 3
- 210000003491 skin Anatomy 0.000 description 3
- HYHCSLBZRBJJCH-UHFFFAOYSA-M sodium hydrosulfide Chemical compound [Na+].[SH-] HYHCSLBZRBJJCH-UHFFFAOYSA-M 0.000 description 3
- 239000000600 sorbitol Substances 0.000 description 3
- 210000000278 spinal cord Anatomy 0.000 description 3
- 210000000952 spleen Anatomy 0.000 description 3
- 235000000346 sugar Nutrition 0.000 description 3
- 150000005846 sugar alcohols Polymers 0.000 description 3
- 150000008163 sugars Chemical class 0.000 description 3
- 239000003765 sweetening agent Substances 0.000 description 3
- 230000000699 topical effect Effects 0.000 description 3
- 230000002792 vascular Effects 0.000 description 3
- 230000008673 vomiting Effects 0.000 description 3
- 239000000080 wetting agent Substances 0.000 description 3
- AIFRHYZBTHREPW-UHFFFAOYSA-N β-carboline Chemical class N1=CC=C2C3=CC=CC=C3NC2=C1 AIFRHYZBTHREPW-UHFFFAOYSA-N 0.000 description 3
- BIXYYZIIJIXVFW-UUOKFMHZSA-N (2R,3R,4S,5R)-2-(6-amino-2-chloro-9-purinyl)-5-(hydroxymethyl)oxolane-3,4-diol Chemical compound C1=NC=2C(N)=NC(Cl)=NC=2N1[C@@H]1O[C@H](CO)[C@@H](O)[C@H]1O BIXYYZIIJIXVFW-UUOKFMHZSA-N 0.000 description 2
- QDZOEBFLNHCSSF-PFFBOGFISA-N (2S)-2-[[(2R)-2-[[(2S)-1-[(2S)-6-amino-2-[[(2S)-1-[(2R)-2-amino-5-carbamimidamidopentanoyl]pyrrolidine-2-carbonyl]amino]hexanoyl]pyrrolidine-2-carbonyl]amino]-3-(1H-indol-3-yl)propanoyl]amino]-N-[(2R)-1-[[(2S)-1-[[(2R)-1-[[(2S)-1-[[(2S)-1-amino-4-methyl-1-oxopentan-2-yl]amino]-4-methyl-1-oxopentan-2-yl]amino]-3-(1H-indol-3-yl)-1-oxopropan-2-yl]amino]-1-oxo-3-phenylpropan-2-yl]amino]-3-(1H-indol-3-yl)-1-oxopropan-2-yl]pentanediamide Chemical compound C([C@@H](C(=O)N[C@H](CC=1C2=CC=CC=C2NC=1)C(=O)N[C@@H](CC(C)C)C(=O)N[C@@H](CC(C)C)C(N)=O)NC(=O)[C@@H](CC=1C2=CC=CC=C2NC=1)NC(=O)[C@H](CCC(N)=O)NC(=O)[C@@H](CC=1C2=CC=CC=C2NC=1)NC(=O)[C@H]1N(CCC1)C(=O)[C@H](CCCCN)NC(=O)[C@H]1N(CCC1)C(=O)[C@H](N)CCCNC(N)=N)C1=CC=CC=C1 QDZOEBFLNHCSSF-PFFBOGFISA-N 0.000 description 2
- VLPIATFUUWWMKC-SNVBAGLBSA-N (2r)-1-(2,6-dimethylphenoxy)propan-2-amine Chemical compound C[C@@H](N)COC1=C(C)C=CC=C1C VLPIATFUUWWMKC-SNVBAGLBSA-N 0.000 description 2
- MHKFLPIBDSYTPZ-AXYPVASZSA-N (2r,3r,4r,5r)-3-amino-2-(6-aminopurin-9-yl)-5-(hydroxymethyl)-2-(2-phenylethyl)oxolane-3,4-diol Chemical compound C1=NC=2C(N)=NC=NC=2N1[C@]1(CCC=2C=CC=CC=2)O[C@H](CO)[C@@H](O)[C@@]1(N)O MHKFLPIBDSYTPZ-AXYPVASZSA-N 0.000 description 2
- PHIQHXFUZVPYII-ZCFIWIBFSA-O (R)-carnitinium Chemical compound C[N+](C)(C)C[C@H](O)CC(O)=O PHIQHXFUZVPYII-ZCFIWIBFSA-O 0.000 description 2
- AZUYLZMQTIKGSC-UHFFFAOYSA-N 1-[6-[4-(5-chloro-6-methyl-1H-indazol-4-yl)-5-methyl-3-(1-methylindazol-5-yl)pyrazol-1-yl]-2-azaspiro[3.3]heptan-2-yl]prop-2-en-1-one Chemical compound ClC=1C(=C2C=NNC2=CC=1C)C=1C(=NN(C=1C)C1CC2(CN(C2)C(C=C)=O)C1)C=1C=C2C=NN(C2=CC=1)C AZUYLZMQTIKGSC-UHFFFAOYSA-N 0.000 description 2
- AQTKXCPRNZDOJU-NXRLNHOXSA-N 2-(alpha-D-galactosyl)glycerol Chemical compound OCC(CO)O[C@H]1O[C@H](CO)[C@H](O)[C@H](O)[C@H]1O AQTKXCPRNZDOJU-NXRLNHOXSA-N 0.000 description 2
- AQTKXCPRNZDOJU-UHFFFAOYSA-N 2-O-alpha-D-Galactopyranosylglycerol Natural products OCC(CO)OC1OC(CO)C(O)C(O)C1O AQTKXCPRNZDOJU-UHFFFAOYSA-N 0.000 description 2
- KPGXRSRHYNQIFN-UHFFFAOYSA-L 2-oxoglutarate(2-) Chemical compound [O-]C(=O)CCC(=O)C([O-])=O KPGXRSRHYNQIFN-UHFFFAOYSA-L 0.000 description 2
- VUBFHEZKFGCCSE-UHFFFAOYSA-N 3-acetamido-6-aminohexanoic acid Chemical compound CC(=O)NC(CC(O)=O)CCCN VUBFHEZKFGCCSE-UHFFFAOYSA-N 0.000 description 2
- UIAGMCDKSXEBJQ-IBGZPJMESA-N 3-o-(2-methoxyethyl) 5-o-propan-2-yl (4s)-2,6-dimethyl-4-(3-nitrophenyl)-1,4-dihydropyridine-3,5-dicarboxylate Chemical compound COCCOC(=O)C1=C(C)NC(C)=C(C(=O)OC(C)C)[C@H]1C1=CC=CC([N+]([O-])=O)=C1 UIAGMCDKSXEBJQ-IBGZPJMESA-N 0.000 description 2
- 239000005541 ACE inhibitor Substances 0.000 description 2
- 101150007969 ADORA1 gene Proteins 0.000 description 2
- RTRQQBHATOEIAF-UHFFFAOYSA-N AICA riboside Natural products NC1=C(C(=O)N)N=CN1C1C(O)C(O)C(CO)O1 RTRQQBHATOEIAF-UHFFFAOYSA-N 0.000 description 2
- RZVAJINKPMORJF-UHFFFAOYSA-N Acetaminophen Chemical compound CC(=O)NC1=CC=C(O)C=C1 RZVAJINKPMORJF-UHFFFAOYSA-N 0.000 description 2
- 206010048998 Acute phase reaction Diseases 0.000 description 2
- 206010001052 Acute respiratory distress syndrome Diseases 0.000 description 2
- 241001204830 Alatina alata Species 0.000 description 2
- 208000007848 Alcoholism Diseases 0.000 description 2
- ITPDYQOUSLNIHG-UHFFFAOYSA-N Amiodarone hydrochloride Chemical compound [Cl-].CCCCC=1OC2=CC=CC=C2C=1C(=O)C1=CC(I)=C(OCC[NH+](CC)CC)C(I)=C1 ITPDYQOUSLNIHG-UHFFFAOYSA-N 0.000 description 2
- 206010002383 Angina Pectoris Diseases 0.000 description 2
- 108010064733 Angiotensins Proteins 0.000 description 2
- 102000015427 Angiotensins Human genes 0.000 description 2
- 108010085443 Anserine Proteins 0.000 description 2
- 108010039627 Aprotinin Proteins 0.000 description 2
- 239000004475 Arginine Substances 0.000 description 2
- BSYNRYMUTXBXSQ-UHFFFAOYSA-N Aspirin Chemical compound CC(=O)OC1=CC=CC=C1C(O)=O BSYNRYMUTXBXSQ-UHFFFAOYSA-N 0.000 description 2
- IJGRMHOSHXDMSA-UHFFFAOYSA-N Atomic nitrogen Chemical compound N#N IJGRMHOSHXDMSA-UHFFFAOYSA-N 0.000 description 2
- KXDAEFPNCMNJSK-UHFFFAOYSA-N Benzamide Chemical compound NC(=O)C1=CC=CC=C1 KXDAEFPNCMNJSK-UHFFFAOYSA-N 0.000 description 2
- BPYKTIZUTYGOLE-IFADSCNNSA-N Bilirubin Chemical compound N1C(=O)C(C)=C(C=C)\C1=C\C1=C(C)C(CCC(O)=O)=C(CC2=C(C(C)=C(\C=C/3C(=C(C=C)C(=O)N\3)C)N2)CCC(O)=O)N1 BPYKTIZUTYGOLE-IFADSCNNSA-N 0.000 description 2
- 102000015081 Blood Coagulation Factors Human genes 0.000 description 2
- 108010039209 Blood Coagulation Factors Proteins 0.000 description 2
- 241000283690 Bos taurus Species 0.000 description 2
- 241000252983 Caecum Species 0.000 description 2
- 241000282472 Canis lupus familiaris Species 0.000 description 2
- CURLTUGMZLYLDI-UHFFFAOYSA-N Carbon dioxide Chemical compound O=C=O CURLTUGMZLYLDI-UHFFFAOYSA-N 0.000 description 2
- 241000426847 Carukia Species 0.000 description 2
- 208000035473 Communicable disease Diseases 0.000 description 2
- 206010011703 Cyanosis Diseases 0.000 description 2
- FBPFZTCFMRRESA-KVTDHHQDSA-N D-Mannitol Chemical compound OC[C@@H](O)[C@@H](O)[C@H](O)[C@H](O)CO FBPFZTCFMRRESA-KVTDHHQDSA-N 0.000 description 2
- 101710088194 Dehydrogenase Proteins 0.000 description 2
- 206010012735 Diarrhoea Diseases 0.000 description 2
- RTZKZFJDLAIYFH-UHFFFAOYSA-N Diethyl ether Chemical compound CCOCC RTZKZFJDLAIYFH-UHFFFAOYSA-N 0.000 description 2
- 241000017055 Dipluridae Species 0.000 description 2
- 208000003870 Drug Overdose Diseases 0.000 description 2
- WQXNXVUDBPYKBA-UHFFFAOYSA-N Ectoine Natural products CC1=NCCC(C(O)=O)N1 WQXNXVUDBPYKBA-UHFFFAOYSA-N 0.000 description 2
- 102000002322 Egg Proteins Human genes 0.000 description 2
- 108010000912 Egg Proteins Proteins 0.000 description 2
- 208000037487 Endotoxemia Diseases 0.000 description 2
- CTKXFMQHOOWWEB-UHFFFAOYSA-N Ethylene oxide/propylene oxide copolymer Chemical compound CCCOC(C)COCCO CTKXFMQHOOWWEB-UHFFFAOYSA-N 0.000 description 2
- 229940123457 Free radical scavenger Drugs 0.000 description 2
- 102000053171 Glial Fibrillary Acidic Human genes 0.000 description 2
- 101710193519 Glial fibrillary acidic protein Proteins 0.000 description 2
- 108010063907 Glutathione Reductase Proteins 0.000 description 2
- 102100036442 Glutathione reductase, mitochondrial Human genes 0.000 description 2
- DHMQDGOQFOQNFH-UHFFFAOYSA-N Glycine Chemical compound NCC(O)=O DHMQDGOQFOQNFH-UHFFFAOYSA-N 0.000 description 2
- 102000003886 Glycoproteins Human genes 0.000 description 2
- 108090000288 Glycoproteins Proteins 0.000 description 2
- 229940121710 HMGCoA reductase inhibitor Drugs 0.000 description 2
- 208000013875 Heart injury Diseases 0.000 description 2
- 101000831616 Homo sapiens Protachykinin-1 Proteins 0.000 description 2
- UFHFLCQGNIYNRP-UHFFFAOYSA-N Hydrogen Chemical compound [H][H] UFHFLCQGNIYNRP-UHFFFAOYSA-N 0.000 description 2
- 208000008454 Hyperhidrosis Diseases 0.000 description 2
- 206010020751 Hypersensitivity Diseases 0.000 description 2
- 102000015696 Interleukins Human genes 0.000 description 2
- 108010063738 Interleukins Proteins 0.000 description 2
- 201000008450 Intracranial aneurysm Diseases 0.000 description 2
- 102000004310 Ion Channels Human genes 0.000 description 2
- 108090000862 Ion Channels Proteins 0.000 description 2
- XUJNEKJLAYXESH-REOHCLBHSA-N L-Cysteine Chemical compound SC[C@H](N)C(O)=O XUJNEKJLAYXESH-REOHCLBHSA-N 0.000 description 2
- ONIBWKKTOPOVIA-BYPYZUCNSA-N L-Proline Chemical compound OC(=O)[C@@H]1CCCN1 ONIBWKKTOPOVIA-BYPYZUCNSA-N 0.000 description 2
- QNAYBMKLOCPYGJ-REOHCLBHSA-N L-alanine Chemical compound C[C@H](N)C(O)=O QNAYBMKLOCPYGJ-REOHCLBHSA-N 0.000 description 2
- SLRNWACWRVGMKD-UHFFFAOYSA-N L-anserine Natural products CN1C=NC(CC(NC(=O)CCN)C(O)=O)=C1 SLRNWACWRVGMKD-UHFFFAOYSA-N 0.000 description 2
- ODKSFYDXXFIFQN-BYPYZUCNSA-P L-argininium(2+) Chemical compound NC(=[NH2+])NCCC[C@H]([NH3+])C(O)=O ODKSFYDXXFIFQN-BYPYZUCNSA-P 0.000 description 2
- CKLJMWTZIZZHCS-REOHCLBHSA-N L-aspartic acid Chemical compound OC(=O)[C@@H](N)CC(O)=O CKLJMWTZIZZHCS-REOHCLBHSA-N 0.000 description 2
- WHUUTDBJXJRKMK-VKHMYHEASA-N L-glutamic acid Chemical compound OC(=O)[C@@H](N)CCC(O)=O WHUUTDBJXJRKMK-VKHMYHEASA-N 0.000 description 2
- TWRXJAOTZQYOKJ-UHFFFAOYSA-L Magnesium chloride Chemical compound [Mg+2].[Cl-].[Cl-] TWRXJAOTZQYOKJ-UHFFFAOYSA-L 0.000 description 2
- 229930195725 Mannitol Natural products 0.000 description 2
- YJPIGAIKUZMOQA-UHFFFAOYSA-N Melatonin Natural products COC1=CC=C2N(C(C)=O)C=C(CCN)C2=C1 YJPIGAIKUZMOQA-UHFFFAOYSA-N 0.000 description 2
- 201000009906 Meningitis Diseases 0.000 description 2
- 208000034486 Multi-organ failure Diseases 0.000 description 2
- 208000010718 Multiple Organ Failure Diseases 0.000 description 2
- 206010028347 Muscle twitching Diseases 0.000 description 2
- JADDQZYHOWSFJD-FLNNQWSLSA-N N-ethyl-5'-carboxamidoadenosine Chemical compound O[C@@H]1[C@H](O)[C@@H](C(=O)NCC)O[C@H]1N1C2=NC=NC(N)=C2N=C1 JADDQZYHOWSFJD-FLNNQWSLSA-N 0.000 description 2
- 238000004497 NIR spectroscopy Methods 0.000 description 2
- 208000006079 Near drowning Diseases 0.000 description 2
- 206010028851 Necrosis Diseases 0.000 description 2
- 102000008763 Neurofilament Proteins Human genes 0.000 description 2
- 108010088373 Neurofilament Proteins Proteins 0.000 description 2
- 206010058119 Neurogenic shock Diseases 0.000 description 2
- ZBBHBTPTTSWHBA-UHFFFAOYSA-N Nicardipine Chemical compound COC(=O)C1=C(C)NC(C)=C(C(=O)OCCN(C)CC=2C=CC=CC=2)C1C1=CC=CC([N+]([O-])=O)=C1 ZBBHBTPTTSWHBA-UHFFFAOYSA-N 0.000 description 2
- 206010073708 Obstructive shock Diseases 0.000 description 2
- 229940127450 Opioid Agonists Drugs 0.000 description 2
- 108010093625 Opioid Peptides Proteins 0.000 description 2
- 102000001490 Opioid Peptides Human genes 0.000 description 2
- 206010053159 Organ failure Diseases 0.000 description 2
- 206010033296 Overdoses Diseases 0.000 description 2
- 229920002123 Pentastarch Polymers 0.000 description 2
- CXOFVDLJLONNDW-UHFFFAOYSA-N Phenytoin Chemical compound N1C(=O)NC(=O)C1(C=1C=CC=CC=1)C1=CC=CC=C1 CXOFVDLJLONNDW-UHFFFAOYSA-N 0.000 description 2
- 208000005374 Poisoning Diseases 0.000 description 2
- 206010067268 Post procedural infection Diseases 0.000 description 2
- 102100024622 Proenkephalin-B Human genes 0.000 description 2
- ONIBWKKTOPOVIA-UHFFFAOYSA-N Proline Natural products OC(=O)C1CCCN1 ONIBWKKTOPOVIA-UHFFFAOYSA-N 0.000 description 2
- 102100024304 Protachykinin-1 Human genes 0.000 description 2
- 108010094028 Prothrombin Proteins 0.000 description 2
- 102100027378 Prothrombin Human genes 0.000 description 2
- MUPFEKGTMRGPLJ-RMMQSMQOSA-N Raffinose Natural products O(C[C@H]1[C@@H](O)[C@H](O)[C@@H](O)[C@@H](O[C@@]2(CO)[C@H](O)[C@@H](O)[C@@H](CO)O2)O1)[C@@H]1[C@H](O)[C@@H](O)[C@@H](O)[C@@H](CO)O1 MUPFEKGTMRGPLJ-RMMQSMQOSA-N 0.000 description 2
- 208000013616 Respiratory Distress Syndrome Diseases 0.000 description 2
- 239000008156 Ringer's lactate solution Substances 0.000 description 2
- DBMJMQXJHONAFJ-UHFFFAOYSA-M Sodium laurylsulphate Chemical compound [Na+].CCCCCCCCCCCCOS([O-])(=O)=O DBMJMQXJHONAFJ-UHFFFAOYSA-M 0.000 description 2
- 229920002472 Starch Polymers 0.000 description 2
- 102400000096 Substance P Human genes 0.000 description 2
- 101800003906 Substance P Proteins 0.000 description 2
- 241000282887 Suidae Species 0.000 description 2
- 102000019197 Superoxide Dismutase Human genes 0.000 description 2
- 108010012715 Superoxide dismutase Proteins 0.000 description 2
- 208000002847 Surgical Wound Diseases 0.000 description 2
- IUJDSEJGGMCXSG-UHFFFAOYSA-N Thiopental Chemical compound CCCC(C)C1(CC)C(=O)NC(=S)NC1=O IUJDSEJGGMCXSG-UHFFFAOYSA-N 0.000 description 2
- 108090000190 Thrombin Proteins 0.000 description 2
- 102000004887 Transforming Growth Factor beta Human genes 0.000 description 2
- 108090001012 Transforming Growth Factor beta Proteins 0.000 description 2
- MUPFEKGTMRGPLJ-UHFFFAOYSA-N UNPD196149 Natural products OC1C(O)C(CO)OC1(CO)OC1C(O)C(O)C(O)C(COC2C(C(O)C(O)C(CO)O2)O)O1 MUPFEKGTMRGPLJ-UHFFFAOYSA-N 0.000 description 2
- LEHOTFFKMJEONL-UHFFFAOYSA-N Uric Acid Chemical compound N1C(=O)NC(=O)C2=C1NC(=O)N2 LEHOTFFKMJEONL-UHFFFAOYSA-N 0.000 description 2
- 102000005789 Vascular Endothelial Growth Factors Human genes 0.000 description 2
- 108010019530 Vascular Endothelial Growth Factors Proteins 0.000 description 2
- DDNCQMVWWZOMLN-IRLDBZIGSA-N Vinpocetine Chemical compound C1=CC=C2C(CCN3CCC4)=C5[C@@H]3[C@]4(CC)C=C(C(=O)OCC)N5C2=C1 DDNCQMVWWZOMLN-IRLDBZIGSA-N 0.000 description 2
- 229930003427 Vitamin E Natural products 0.000 description 2
- XJLXINKUBYWONI-DQQFMEOOSA-N [[(2r,3r,4r,5r)-5-(6-aminopurin-9-yl)-3-hydroxy-4-phosphonooxyoxolan-2-yl]methoxy-hydroxyphosphoryl] [(2s,3r,4s,5s)-5-(3-carbamoylpyridin-1-ium-1-yl)-3,4-dihydroxyoxolan-2-yl]methyl phosphate Chemical compound NC(=O)C1=CC=C[N+]([C@@H]2[C@H]([C@@H](O)[C@H](COP([O-])(=O)OP(O)(=O)OC[C@@H]3[C@H]([C@@H](OP(O)(O)=O)[C@@H](O3)N3C4=NC=NC(N)=C4N=C3)O)O2)O)=C1 XJLXINKUBYWONI-DQQFMEOOSA-N 0.000 description 2
- 238000012084 abdominal surgery Methods 0.000 description 2
- 230000002159 abnormal effect Effects 0.000 description 2
- RTRQQBHATOEIAF-UUOKFMHZSA-N acadesine Chemical compound NC1=C(C(=O)N)N=CN1[C@H]1[C@H](O)[C@H](O)[C@@H](CO)O1 RTRQQBHATOEIAF-UUOKFMHZSA-N 0.000 description 2
- 230000001133 acceleration Effects 0.000 description 2
- 238000009825 accumulation Methods 0.000 description 2
- 229960001138 acetylsalicylic acid Drugs 0.000 description 2
- 230000007950 acidosis Effects 0.000 description 2
- 208000026545 acidosis disease Diseases 0.000 description 2
- 239000000654 additive Substances 0.000 description 2
- 208000011341 adult acute respiratory distress syndrome Diseases 0.000 description 2
- 201000000028 adult respiratory distress syndrome Diseases 0.000 description 2
- 235000004279 alanine Nutrition 0.000 description 2
- 206010001584 alcohol abuse Diseases 0.000 description 2
- 208000025746 alcohol use disease Diseases 0.000 description 2
- 208000030961 allergic reaction Diseases 0.000 description 2
- 230000003281 allosteric effect Effects 0.000 description 2
- 230000004075 alteration Effects 0.000 description 2
- 229960005260 amiodarone Drugs 0.000 description 2
- 230000010100 anticoagulation Effects 0.000 description 2
- 229940127218 antiplatelet drug Drugs 0.000 description 2
- 230000006907 apoptotic process Effects 0.000 description 2
- 229960004405 aprotinin Drugs 0.000 description 2
- ODKSFYDXXFIFQN-UHFFFAOYSA-N arginine Natural products OC(=O)C(N)CCCNC(N)=N ODKSFYDXXFIFQN-UHFFFAOYSA-N 0.000 description 2
- KBZOIRJILGZLEJ-LGYYRGKSSA-N argipressin Chemical compound C([C@H]1C(=O)N[C@@H](CCC(N)=O)C(=O)N[C@@H](CC(N)=O)C(=O)N[C@@H](CSSC[C@@H](C(N[C@@H](CC=2C=CC(O)=CC=2)C(=O)N1)=O)N)C(=O)N1[C@@H](CCC1)C(=O)N[C@@H](CCCN=C(N)N)C(=O)NCC(N)=O)C1=CC=CC=C1 KBZOIRJILGZLEJ-LGYYRGKSSA-N 0.000 description 2
- 230000002763 arrhythmic effect Effects 0.000 description 2
- 235000010323 ascorbic acid Nutrition 0.000 description 2
- 239000011668 ascorbic acid Substances 0.000 description 2
- 229940009098 aspartate Drugs 0.000 description 2
- 238000011888 autopsy Methods 0.000 description 2
- 108091008698 baroreceptors Proteins 0.000 description 2
- 229940049706 benzodiazepine Drugs 0.000 description 2
- 150000001557 benzodiazepines Chemical class 0.000 description 2
- WPYMKLBDIGXBTP-UHFFFAOYSA-N benzoic acid group Chemical group C(C1=CC=CC=C1)(=O)O WPYMKLBDIGXBTP-UHFFFAOYSA-N 0.000 description 2
- 239000000090 biomarker Substances 0.000 description 2
- 239000003114 blood coagulation factor Substances 0.000 description 2
- 239000003633 blood substitute Substances 0.000 description 2
- 210000001218 blood-brain barrier Anatomy 0.000 description 2
- 239000010839 body fluid Substances 0.000 description 2
- 230000036471 bradycardia Effects 0.000 description 2
- 208000006218 bradycardia Diseases 0.000 description 2
- 230000005587 bubbling Effects 0.000 description 2
- 150000001669 calcium Chemical class 0.000 description 2
- 229910052799 carbon Inorganic materials 0.000 description 2
- 229910002092 carbon dioxide Inorganic materials 0.000 description 2
- 150000003857 carboxamides Chemical class 0.000 description 2
- 150000001735 carboxylic acids Chemical class 0.000 description 2
- 230000003293 cardioprotective effect Effects 0.000 description 2
- IWXNYAIICFKCTM-UHFFFAOYSA-N cariporide Chemical compound CC(C)C1=CC=C(C(=O)N=C(N)N)C=C1S(C)(=O)=O IWXNYAIICFKCTM-UHFFFAOYSA-N 0.000 description 2
- 229960004203 carnitine Drugs 0.000 description 2
- 210000001715 carotid artery Anatomy 0.000 description 2
- 230000003915 cell function Effects 0.000 description 2
- 230000007541 cellular toxicity Effects 0.000 description 2
- 230000002057 chronotropic effect Effects 0.000 description 2
- ACTIUHUUMQJHFO-UPTCCGCDSA-N coenzyme Q10 Chemical compound COC1=C(OC)C(=O)C(C\C=C(/C)CC\C=C(/C)CC\C=C(/C)CC\C=C(/C)CC\C=C(/C)CC\C=C(/C)CC\C=C(/C)CC\C=C(/C)CC\C=C(/C)CCC=C(C)C)=C(C)C1=O ACTIUHUUMQJHFO-UPTCCGCDSA-N 0.000 description 2
- 230000006999 cognitive decline Effects 0.000 description 2
- 208000010877 cognitive disease Diseases 0.000 description 2
- 230000002860 competitive effect Effects 0.000 description 2
- 108050003126 conotoxin Proteins 0.000 description 2
- 230000036757 core body temperature Effects 0.000 description 2
- VFLDPWHFBUODDF-FCXRPNKRSA-N curcumin Chemical compound C1=C(O)C(OC)=CC(\C=C\C(=O)CC(=O)\C=C\C=2C=C(OC)C(O)=CC=2)=C1 VFLDPWHFBUODDF-FCXRPNKRSA-N 0.000 description 2
- SDZRWUKZFQQKKV-JHADDHBZSA-N cytochalasin D Chemical compound C([C@H]1[C@@H]2[C@@H](C([C@@H](O)[C@H]\3[C@]2([C@@H](/C=C/[C@@](C)(O)C(=O)[C@@H](C)C/C=C/3)OC(C)=O)C(=O)N1)=C)C)C1=CC=CC=C1 SDZRWUKZFQQKKV-JHADDHBZSA-N 0.000 description 2
- 230000000254 damaging effect Effects 0.000 description 2
- 230000003412 degenerative effect Effects 0.000 description 2
- 230000018044 dehydration Effects 0.000 description 2
- 238000006297 dehydration reaction Methods 0.000 description 2
- 230000001934 delay Effects 0.000 description 2
- 230000002939 deleterious effect Effects 0.000 description 2
- 108700041286 delta Proteins 0.000 description 2
- 230000000881 depressing effect Effects 0.000 description 2
- 230000001627 detrimental effect Effects 0.000 description 2
- FSEUPUDHEBLWJY-UHFFFAOYSA-N diacetylmonoxime Chemical compound CC(=O)C(C)=NO FSEUPUDHEBLWJY-UHFFFAOYSA-N 0.000 description 2
- 238000002405 diagnostic procedure Methods 0.000 description 2
- 238000010586 diagram Methods 0.000 description 2
- 238000000502 dialysis Methods 0.000 description 2
- 229910003460 diamond Inorganic materials 0.000 description 2
- 239000010432 diamond Substances 0.000 description 2
- 230000003205 diastolic effect Effects 0.000 description 2
- 125000004925 dihydropyridyl group Chemical group N1(CC=CC=C1)* 0.000 description 2
- HDRXZJPWHTXQRI-BHDTVMLSSA-N diltiazem hydrochloride Chemical compound [Cl-].C1=CC(OC)=CC=C1[C@H]1[C@@H](OC(C)=O)C(=O)N(CC[NH+](C)C)C2=CC=CC=C2S1 HDRXZJPWHTXQRI-BHDTVMLSSA-N 0.000 description 2
- 238000007907 direct compression Methods 0.000 description 2
- 230000005059 dormancy Effects 0.000 description 2
- 230000001091 dromotropic effect Effects 0.000 description 2
- 231100000725 drug overdose Toxicity 0.000 description 2
- WQXNXVUDBPYKBA-YFKPBYRVSA-N ectoine Chemical compound CC1=[NH+][C@H](C([O-])=O)CCN1 WQXNXVUDBPYKBA-YFKPBYRVSA-N 0.000 description 2
- 238000000537 electroencephalography Methods 0.000 description 2
- 239000000839 emulsion Substances 0.000 description 2
- 230000003511 endothelial effect Effects 0.000 description 2
- 210000003989 endothelium vascular Anatomy 0.000 description 2
- 239000002158 endotoxin Substances 0.000 description 2
- 239000003623 enhancer Substances 0.000 description 2
- 239000002532 enzyme inhibitor Substances 0.000 description 2
- 229940125532 enzyme inhibitor Drugs 0.000 description 2
- 230000003492 excitotoxic effect Effects 0.000 description 2
- 231100000063 excitotoxicity Toxicity 0.000 description 2
- 230000002349 favourable effect Effects 0.000 description 2
- 235000019162 flavin adenine dinucleotide Nutrition 0.000 description 2
- UKYVGQJPUFNXKS-UHFFFAOYSA-N floridoside Natural products CC(=O)OCC(COC(C)=O)OC1OC(COC(C)=O)C(OC(C)=O)C(OC(C)=O)C1OC(C)=O UKYVGQJPUFNXKS-UHFFFAOYSA-N 0.000 description 2
- 235000003599 food sweetener Nutrition 0.000 description 2
- 238000009472 formulation Methods 0.000 description 2
- WIGCFUFOHFEKBI-UHFFFAOYSA-N gamma-tocopherol Natural products CC(C)CCCC(C)CCCC(C)CCCC1CCC2C(C)C(O)C(C)C(C)C2O1 WIGCFUFOHFEKBI-UHFFFAOYSA-N 0.000 description 2
- 239000003193 general anesthetic agent Substances 0.000 description 2
- 210000004602 germ cell Anatomy 0.000 description 2
- 210000005046 glial fibrillary acidic protein Anatomy 0.000 description 2
- 229930195712 glutamate Natural products 0.000 description 2
- RWSXRVCMGQZWBV-WDSKDSINSA-N glutathione Chemical compound OC(=O)[C@@H](N)CCC(=O)N[C@@H](CS)C(=O)NCC(O)=O RWSXRVCMGQZWBV-WDSKDSINSA-N 0.000 description 2
- PCHJSUWPFVWCPO-UHFFFAOYSA-N gold Chemical compound [Au] PCHJSUWPFVWCPO-UHFFFAOYSA-N 0.000 description 2
- 239000008187 granular material Substances 0.000 description 2
- 238000003306 harvesting Methods 0.000 description 2
- 230000036541 health Effects 0.000 description 2
- 230000005986 heart dysfunction Effects 0.000 description 2
- 230000006266 hibernation Effects 0.000 description 2
- 230000003284 homeostatic effect Effects 0.000 description 2
- 230000013632 homeostatic process Effects 0.000 description 2
- JYGXADMDTFJGBT-VWUMJDOOSA-N hydrocortisone Chemical compound O=C1CC[C@]2(C)[C@H]3[C@@H](O)C[C@](C)([C@@](CC4)(O)C(=O)CO)[C@@H]4[C@@H]3CCC2=C1 JYGXADMDTFJGBT-VWUMJDOOSA-N 0.000 description 2
- 239000000819 hypertonic solution Substances 0.000 description 2
- 229940021223 hypertonic solution Drugs 0.000 description 2
- 230000002267 hypothalamic effect Effects 0.000 description 2
- CGIGDMFJXJATDK-UHFFFAOYSA-N indomethacin Chemical compound CC1=C(CC(O)=O)C2=CC(OC)=CC=C2N1C(=O)C1=CC=C(Cl)C=C1 CGIGDMFJXJATDK-UHFFFAOYSA-N 0.000 description 2
- 230000006698 induction Effects 0.000 description 2
- ZPNFWUPYTFPOJU-LPYSRVMUSA-N iniprol Chemical compound C([C@H]1C(=O)NCC(=O)NCC(=O)N[C@H]2CSSC[C@H]3C(=O)N[C@@H](CCCCN)C(=O)N[C@@H](C)C(=O)N[C@@H](CCCNC(N)=N)C(=O)N[C@H](C(N[C@H](C(=O)N[C@@H](CCCNC(N)=N)C(=O)N[C@@H](CC=4C=CC(O)=CC=4)C(=O)N[C@@H](CC=4C=CC=CC=4)C(=O)N[C@@H](CC=4C=CC(O)=CC=4)C(=O)N[C@@H](CC(N)=O)C(=O)N[C@@H](C)C(=O)N[C@@H](CCCCN)C(=O)N[C@@H](C)C(=O)NCC(=O)N[C@@H](CC(C)C)C(=O)N[C@@H](CSSC[C@H](NC(=O)[C@H](CC(O)=O)NC(=O)[C@H](CCC(O)=O)NC(=O)[C@H](C)NC(=O)[C@H](CO)NC(=O)[C@H](CCCCN)NC(=O)[C@H](CC=4C=CC=CC=4)NC(=O)[C@H](CC(N)=O)NC(=O)[C@H](CC(N)=O)NC(=O)[C@H](CCCNC(N)=N)NC(=O)[C@H](CCCCN)NC(=O)[C@H](C)NC(=O)[C@H](CCCNC(N)=N)NC2=O)C(=O)N[C@@H](CCSC)C(=O)N[C@@H](CCCNC(N)=N)C(=O)N[C@@H]([C@@H](C)O)C(=O)N[C@@H](CSSC[C@H](NC(=O)[C@H](CC=2C=CC=CC=2)NC(=O)[C@H](CC(O)=O)NC(=O)[C@H]2N(CCC2)C(=O)[C@@H](N)CCCNC(N)=N)C(=O)N[C@@H](CC(C)C)C(=O)N[C@@H](CCC(O)=O)C(=O)N2[C@@H](CCC2)C(=O)N2[C@@H](CCC2)C(=O)N[C@@H](CC=2C=CC(O)=CC=2)C(=O)N[C@@H]([C@@H](C)O)C(=O)NCC(=O)N2[C@@H](CCC2)C(=O)N3)C(=O)NCC(=O)NCC(=O)N[C@@H](C)C(O)=O)C(=O)N[C@@H](CCC(N)=O)C(=O)N[C@H](C(=O)N[C@@H](CC=2C=CC=CC=2)C(=O)N[C@H](C(=O)N1)C(C)C)[C@@H](C)O)[C@@H](C)CC)=O)[C@@H](C)CC)C1=CC=C(O)C=C1 ZPNFWUPYTFPOJU-LPYSRVMUSA-N 0.000 description 2
- 229940100601 interleukin-6 Drugs 0.000 description 2
- 201000009941 intracranial hypertension Diseases 0.000 description 2
- 238000010255 intramuscular injection Methods 0.000 description 2
- 239000007928 intraperitoneal injection Substances 0.000 description 2
- 230000002427 irreversible effect Effects 0.000 description 2
- FZWBNHMXJMCXLU-BLAUPYHCSA-N isomaltotriose Chemical compound O[C@@H]1[C@@H](O)[C@H](O)[C@@H](CO)O[C@@H]1OC[C@@H]1[C@@H](O)[C@H](O)[C@@H](O)[C@@H](OC[C@@H](O)[C@@H](O)[C@H](O)[C@@H](O)C=O)O1 FZWBNHMXJMCXLU-BLAUPYHCSA-N 0.000 description 2
- 102000048260 kappa Opioid Receptors Human genes 0.000 description 2
- 230000003907 kidney function Effects 0.000 description 2
- 238000009533 lab test Methods 0.000 description 2
- 238000002350 laparotomy Methods 0.000 description 2
- 235000019136 lipoic acid Nutrition 0.000 description 2
- 230000007774 longterm Effects 0.000 description 2
- 210000002540 macrophage Anatomy 0.000 description 2
- 229940049920 malate Drugs 0.000 description 2
- BJEPYKJPYRNKOW-UHFFFAOYSA-N malic acid Chemical compound OC(=O)C(O)CC(O)=O BJEPYKJPYRNKOW-UHFFFAOYSA-N 0.000 description 2
- 239000000594 mannitol Substances 0.000 description 2
- 235000010355 mannitol Nutrition 0.000 description 2
- DRLFMBDRBRZALE-UHFFFAOYSA-N melatonin Chemical compound COC1=CC=C2NC=C(CCNC(C)=O)C2=C1 DRLFMBDRBRZALE-UHFFFAOYSA-N 0.000 description 2
- 229960003987 melatonin Drugs 0.000 description 2
- 230000028161 membrane depolarization Effects 0.000 description 2
- 230000007102 metabolic function Effects 0.000 description 2
- CWWARWOPSKGELM-SARDKLJWSA-N methyl (2s)-2-[[(2s)-2-[[2-[[(2s)-2-[[(2s)-2-[[(2s)-5-amino-2-[[(2s)-5-amino-2-[[(2s)-1-[(2s)-6-amino-2-[[(2s)-1-[(2s)-2-amino-5-(diaminomethylideneamino)pentanoyl]pyrrolidine-2-carbonyl]amino]hexanoyl]pyrrolidine-2-carbonyl]amino]-5-oxopentanoyl]amino]-5 Chemical compound C([C@@H](C(=O)NCC(=O)N[C@@H](CC(C)C)C(=O)N[C@@H](CCSC)C(=O)OC)NC(=O)[C@H](CC=1C=CC=CC=1)NC(=O)[C@H](CCC(N)=O)NC(=O)[C@H](CCC(N)=O)NC(=O)[C@H]1N(CCC1)C(=O)[C@H](CCCCN)NC(=O)[C@H]1N(CCC1)C(=O)[C@@H](N)CCCN=C(N)N)C1=CC=CC=C1 CWWARWOPSKGELM-SARDKLJWSA-N 0.000 description 2
- 229960003404 mexiletine Drugs 0.000 description 2
- DDLIGBOFAVUZHB-UHFFFAOYSA-N midazolam Chemical compound C12=CC(Cl)=CC=C2N2C(C)=NC=C2CN=C1C1=CC=CC=C1F DDLIGBOFAVUZHB-UHFFFAOYSA-N 0.000 description 2
- 229960003793 midazolam Drugs 0.000 description 2
- 230000003278 mimic effect Effects 0.000 description 2
- 210000001616 monocyte Anatomy 0.000 description 2
- BQJCRHHNABKAKU-KBQPJGBKSA-N morphine Chemical compound O([C@H]1[C@H](C=C[C@H]23)O)C4=C5[C@@]12CCN(C)[C@@H]3CC5=CC=C4O BQJCRHHNABKAKU-KBQPJGBKSA-N 0.000 description 2
- 208000029744 multiple organ dysfunction syndrome Diseases 0.000 description 2
- 230000002107 myocardial effect Effects 0.000 description 2
- 208000031225 myocardial ischemia Diseases 0.000 description 2
- 210000004165 myocardium Anatomy 0.000 description 2
- UADMBZFZZOBWBB-UHFFFAOYSA-N n-(diaminomethylidene)-2-methyl-5-methylsulfonyl-4-pyrrol-1-ylbenzamide Chemical compound C1=C(C(=O)N=C(N)N)C(C)=CC(N2C=CC=C2)=C1S(C)(=O)=O UADMBZFZZOBWBB-UHFFFAOYSA-N 0.000 description 2
- 230000017074 necrotic cell death Effects 0.000 description 2
- 208000015122 neurodegenerative disease Diseases 0.000 description 2
- 210000005044 neurofilament Anatomy 0.000 description 2
- 230000007971 neurological deficit Effects 0.000 description 2
- 229960001783 nicardipine Drugs 0.000 description 2
- 229930027945 nicotinamide-adenine dinucleotide Natural products 0.000 description 2
- 229960000715 nimodipine Drugs 0.000 description 2
- 239000002840 nitric oxide donor Substances 0.000 description 2
- 229910052757 nitrogen Inorganic materials 0.000 description 2
- HCZKYJDFEPMADG-UHFFFAOYSA-N nordihydroguaiaretic acid Chemical compound C=1C=C(O)C(O)=CC=1CC(C)C(C)CC1=CC=C(O)C(O)=C1 HCZKYJDFEPMADG-UHFFFAOYSA-N 0.000 description 2
- 235000015097 nutrients Nutrition 0.000 description 2
- 239000002674 ointment Substances 0.000 description 2
- 239000003399 opiate peptide Substances 0.000 description 2
- 210000003463 organelle Anatomy 0.000 description 2
- 210000004798 organs belonging to the digestive system Anatomy 0.000 description 2
- 230000003204 osmotic effect Effects 0.000 description 2
- 210000001672 ovary Anatomy 0.000 description 2
- 210000004681 ovum Anatomy 0.000 description 2
- 239000007800 oxidant agent Substances 0.000 description 2
- 230000001590 oxidative effect Effects 0.000 description 2
- 230000036284 oxygen consumption Effects 0.000 description 2
- 238000006213 oxygenation reaction Methods 0.000 description 2
- 210000000496 pancreas Anatomy 0.000 description 2
- 230000032696 parturition Effects 0.000 description 2
- 239000006072 paste Substances 0.000 description 2
- 230000001575 pathological effect Effects 0.000 description 2
- 230000007170 pathology Effects 0.000 description 2
- 229940101738 pentastarch Drugs 0.000 description 2
- 230000002093 peripheral effect Effects 0.000 description 2
- 229960002036 phenytoin Drugs 0.000 description 2
- BASFCYQUMIYNBI-UHFFFAOYSA-N platinum Chemical compound [Pt] BASFCYQUMIYNBI-UHFFFAOYSA-N 0.000 description 2
- 229920001993 poloxamer 188 Polymers 0.000 description 2
- 229940044519 poloxamer 188 Drugs 0.000 description 2
- 150000008442 polyphenolic compounds Chemical class 0.000 description 2
- 235000013824 polyphenols Nutrition 0.000 description 2
- 230000031915 positive regulation of coagulation Effects 0.000 description 2
- FCTRVTQZOUKUIV-MCDZGGTQSA-M potassium;[[[(2r,3s,4r,5r)-5-(6-aminopurin-9-yl)-3,4-dihydroxyoxolan-2-yl]methoxy-hydroxyphosphoryl]oxy-hydroxyphosphoryl] hydrogen phosphate Chemical compound [K+].C1=NC=2C(N)=NC=NC=2N1[C@@H]1O[C@H](COP(O)(=O)OP(O)(=O)OP(O)([O-])=O)[C@@H](O)[C@H]1O FCTRVTQZOUKUIV-MCDZGGTQSA-M 0.000 description 2
- 210000001774 pressoreceptor Anatomy 0.000 description 2
- 230000002265 prevention Effects 0.000 description 2
- 230000002035 prolonged effect Effects 0.000 description 2
- AQHHHDLHHXJYJD-UHFFFAOYSA-N propranolol Chemical compound C1=CC=C2C(OCC(O)CNC(C)C)=CC=CC2=C1 AQHHHDLHHXJYJD-UHFFFAOYSA-N 0.000 description 2
- QELSKZZBTMNZEB-UHFFFAOYSA-N propylparaben Chemical compound CCCOC(=O)C1=CC=C(O)C=C1 QELSKZZBTMNZEB-UHFFFAOYSA-N 0.000 description 2
- 235000018102 proteins Nutrition 0.000 description 2
- 102000004169 proteins and genes Human genes 0.000 description 2
- 229940039716 prothrombin Drugs 0.000 description 2
- 230000002685 pulmonary effect Effects 0.000 description 2
- 230000035485 pulse pressure Effects 0.000 description 2
- LOUPRKONTZGTKE-LHHVKLHASA-N quinidine Chemical compound C([C@H]([C@H](C1)C=C)C2)C[N@@]1[C@H]2[C@@H](O)C1=CC=NC2=CC=C(OC)C=C21 LOUPRKONTZGTKE-LHHVKLHASA-N 0.000 description 2
- 230000005855 radiation Effects 0.000 description 2
- 150000003254 radicals Chemical class 0.000 description 2
- MUPFEKGTMRGPLJ-ZQSKZDJDSA-N raffinose Chemical compound O[C@H]1[C@H](O)[C@@H](CO)O[C@@]1(CO)O[C@@H]1[C@H](O)[C@@H](O)[C@H](O)[C@@H](CO[C@@H]2[C@@H]([C@@H](O)[C@@H](O)[C@@H](CO)O2)O)O1 MUPFEKGTMRGPLJ-ZQSKZDJDSA-N 0.000 description 2
- 108091006082 receptor inhibitors Proteins 0.000 description 2
- 230000011514 reflex Effects 0.000 description 2
- 230000001850 reproductive effect Effects 0.000 description 2
- 230000033764 rhythmic process Effects 0.000 description 2
- 210000000518 sarcolemma Anatomy 0.000 description 2
- 210000004706 scrotum Anatomy 0.000 description 2
- 210000002966 serum Anatomy 0.000 description 2
- 208000037974 severe injury Diseases 0.000 description 2
- 230000009528 severe injury Effects 0.000 description 2
- 210000004927 skin cell Anatomy 0.000 description 2
- 230000007958 sleep Effects 0.000 description 2
- NSUPRLHDCFNOKD-UHFFFAOYSA-N snx 482 Chemical compound N1C(=O)C(CCCNC(N)=N)NC(=O)C(NC(=O)CNC(=O)C(C)NC(=O)C(CCCCN)NC(=O)C(CC(O)=O)NC(=O)C(NC(=O)CN)C(C)C)CSSCC(C(N2CCCC2C(=O)NC(CCCNC(N)=N)C(=O)NC(CC(C)C)C(=O)NCC(=O)N2)=O)NC(=O)C(NC(=O)C(CC(O)=O)NC(=O)C(CC(O)=O)NC(=O)C(CC(N)=O)NC(=O)C(C(C)C)NC(=O)C(CO)NC3=O)CSSCC(C(=O)NC(C)C(=O)NC(CC=4C5=CC=CC=C5NC=4)C(=O)NC(CC(O)=O)C(=O)NC(CC(C)C)C(=O)NC(C(C)O)C(=O)NC(CC=4C=CC=CC=4)C(=O)NC(CO)C(=O)NC(CC(O)=O)C(O)=O)NC(=O)C(CC=4C=CC(O)=CC=4)NC(=O)C(CO)NC(=O)C(CC=4C=CC=CC=4)NC(=O)C(CC(C)C)NC(=O)C(CO)NC(=O)C(CC=4N=CNC=4)NC(=O)C2CSSCC3NC(=O)CNC(=O)CNC(=O)C(CC=2C=CC=CC=2)NC(=O)C(CCSC)NC(=O)C1CC1=CC=C(O)C=C1 NSUPRLHDCFNOKD-UHFFFAOYSA-N 0.000 description 2
- 239000007787 solid Substances 0.000 description 2
- 239000008107 starch Substances 0.000 description 2
- 235000019698 starch Nutrition 0.000 description 2
- 210000001562 sternum Anatomy 0.000 description 2
- 210000002784 stomach Anatomy 0.000 description 2
- 238000003860 storage Methods 0.000 description 2
- ADNPLDHMAVUMIW-CUZNLEPHSA-N substance P Chemical compound C([C@@H](C(=O)NCC(=O)N[C@@H](CC(C)C)C(=O)N[C@@H](CCSC)C(N)=O)NC(=O)[C@H](CC=1C=CC=CC=1)NC(=O)[C@H](CCC(N)=O)NC(=O)[C@H](CCC(N)=O)NC(=O)[C@H]1N(CCC1)C(=O)[C@H](CCCCN)NC(=O)[C@H]1N(CCC1)C(=O)[C@@H](N)CCCN=C(N)N)C1=CC=CC=C1 ADNPLDHMAVUMIW-CUZNLEPHSA-N 0.000 description 2
- KDYFGRWQOYBRFD-UHFFFAOYSA-L succinate(2-) Chemical compound [O-]C(=O)CCC([O-])=O KDYFGRWQOYBRFD-UHFFFAOYSA-L 0.000 description 2
- 239000013589 supplement Substances 0.000 description 2
- 230000035900 sweating Effects 0.000 description 2
- 230000008700 sympathetic activation Effects 0.000 description 2
- 208000024891 symptom Diseases 0.000 description 2
- 239000006188 syrup Substances 0.000 description 2
- 235000020357 syrup Nutrition 0.000 description 2
- 230000008718 systemic inflammatory response Effects 0.000 description 2
- 229960003080 taurine Drugs 0.000 description 2
- 210000001550 testis Anatomy 0.000 description 2
- ZRKFYGHZFMAOKI-QMGMOQQFSA-N tgfbeta Chemical compound C([C@H](NC(=O)[C@H](C(C)C)NC(=O)CNC(=O)[C@H](CCC(O)=O)NC(=O)[C@H](CCCNC(N)=N)NC(=O)[C@H](CC(N)=O)NC(=O)[C@H](CC(C)C)NC(=O)[C@H]([C@@H](C)O)NC(=O)[C@H](CCC(O)=O)NC(=O)[C@H]([C@@H](C)O)NC(=O)[C@H](CC(C)C)NC(=O)CNC(=O)[C@H](C)NC(=O)[C@H](CO)NC(=O)[C@H](CCC(N)=O)NC(=O)[C@@H](NC(=O)[C@H](C)NC(=O)[C@H](C)NC(=O)[C@@H](NC(=O)[C@H](CC(C)C)NC(=O)[C@@H](N)CCSC)C(C)C)[C@@H](C)CC)C(=O)N[C@@H]([C@@H](C)O)C(=O)N[C@@H](C(C)C)C(=O)N[C@@H](CC=1C=CC=CC=1)C(=O)N[C@@H](C)C(=O)N1[C@@H](CCC1)C(=O)N[C@@H]([C@@H](C)O)C(=O)N[C@@H](CC(N)=O)C(=O)N[C@@H](CCC(O)=O)C(=O)N[C@@H](C)C(=O)N[C@@H](CC=1C=CC=CC=1)C(=O)N[C@@H](CCCNC(N)=N)C(=O)N[C@@H](C)C(=O)N[C@@H](CC(C)C)C(=O)N1[C@@H](CCC1)C(=O)N1[C@@H](CCC1)C(=O)N[C@@H](CCCNC(N)=N)C(=O)N[C@@H](CCC(O)=O)C(=O)N[C@@H](CCCNC(N)=N)C(=O)N[C@@H](CO)C(=O)N[C@@H](CCCNC(N)=N)C(=O)N[C@@H](CC(C)C)C(=O)N[C@@H](CC(C)C)C(O)=O)C1=CC=C(O)C=C1 ZRKFYGHZFMAOKI-QMGMOQQFSA-N 0.000 description 2
- 229960002663 thioctic acid Drugs 0.000 description 2
- 229960003279 thiopental Drugs 0.000 description 2
- UMGDCJDMYOKAJW-UHFFFAOYSA-N thiourea Chemical compound NC(N)=S UMGDCJDMYOKAJW-UHFFFAOYSA-N 0.000 description 2
- 229960004072 thrombin Drugs 0.000 description 2
- 201000005665 thrombophilia Diseases 0.000 description 2
- 230000000451 tissue damage Effects 0.000 description 2
- 231100000827 tissue damage Toxicity 0.000 description 2
- 238000002627 tracheal intubation Methods 0.000 description 2
- 230000001052 transient effect Effects 0.000 description 2
- 150000003626 triacylglycerols Chemical class 0.000 description 2
- 238000009424 underpinning Methods 0.000 description 2
- 210000003932 urinary bladder Anatomy 0.000 description 2
- 210000004291 uterus Anatomy 0.000 description 2
- 210000005166 vasculature Anatomy 0.000 description 2
- 230000024883 vasodilation Effects 0.000 description 2
- 229940124549 vasodilator Drugs 0.000 description 2
- 239000003071 vasodilator agent Substances 0.000 description 2
- 238000010865 video microscopy Methods 0.000 description 2
- 229960000744 vinpocetine Drugs 0.000 description 2
- 235000019165 vitamin E Nutrition 0.000 description 2
- 229940046009 vitamin E Drugs 0.000 description 2
- 239000011709 vitamin E Substances 0.000 description 2
- 210000004885 white matter Anatomy 0.000 description 2
- 108020001588 κ-opioid receptors Proteins 0.000 description 2
- KNJNGVKTAFTUFL-OCMUWRIYSA-N ω-conotoxin Chemical compound N([C@@H](CO)C(=O)N[C@@H](CCCN=C(N)N)C(=O)N[C@@H](CC(C)C)C(=O)N[C@@H](CCSC)C(=O)N[C@@H](CC=1C=CC(O)=CC=1)C(=O)N[C@@H](CC(O)=O)C(=O)N[C@H]1C(N[C@@H](CSSC1)C(=O)N[C@@H]([C@@H](C)O)C(=O)NCC(=O)N[C@@H](CO)C(=O)N[C@@H]1C(N[C@@H](CCCN=C(N)N)C(=O)N[C@H](CO)C(=O)NCC(=O)N[C@H](CCCCN)C(=O)N[C@H](CSSC1)C(N)=O)=O)=O)C(=O)[C@@H]1CSSC[C@@H](N)C(=O)N[C@H](CCCCN)C(=O)NCC(=O)N[C@H](CCCCN)C(=O)NCC(=O)N[C@H](C)C(=O)N[C@@H](CCCCN)C(=O)N1 KNJNGVKTAFTUFL-OCMUWRIYSA-N 0.000 description 2
- 108091058550 ω-conotoxin Proteins 0.000 description 2
- HMJIYCCIJYRONP-UHFFFAOYSA-N (+-)-Isradipine Chemical compound COC(=O)C1=C(C)NC(C)=C(C(=O)OC(C)C)C1C1=CC=CC2=NON=C12 HMJIYCCIJYRONP-UHFFFAOYSA-N 0.000 description 1
- WMBWREPUVVBILR-WIYYLYMNSA-N (-)-Epigallocatechin-3-o-gallate Chemical compound O([C@@H]1CC2=C(O)C=C(C=C2O[C@@H]1C=1C=C(O)C(O)=C(O)C=1)O)C(=O)C1=CC(O)=C(O)C(O)=C1 WMBWREPUVVBILR-WIYYLYMNSA-N 0.000 description 1
- GKEMHVLBZNVZOI-SJKOYZFVSA-N (1r,2r)-n-methyl-1-oxo-2-pyridin-3-ylthiane-2-carbothioamide Chemical compound C=1C=CN=CC=1[C@@]1(C(=S)NC)CCCC[S@]1=O GKEMHVLBZNVZOI-SJKOYZFVSA-N 0.000 description 1
- FCDRFVCGMLUYPG-ROUUACIJSA-N (2S,3S)-3-[[3,5-bis(trifluoromethyl)phenyl]methoxy]-2-phenylpiperidine Chemical compound FC(F)(F)C1=CC(C(F)(F)F)=CC(CO[C@@H]2[C@@H](NCCC2)C=2C=CC=CC=2)=C1 FCDRFVCGMLUYPG-ROUUACIJSA-N 0.000 description 1
- ZHUJMSMQIPIPTF-IBURTVSXSA-N (2r)-2-[[(2s)-2-[[2-[[(2r)-2-[[(2s)-2-amino-3-(4-hydroxyphenyl)propanoyl]amino]propanoyl]amino]acetyl]amino]-3-phenylpropanoyl]amino]-4-methylpentanoic acid Chemical compound C([C@@H](C(=O)N[C@H](CC(C)C)C(O)=O)NC(=O)CNC(=O)[C@@H](C)NC(=O)[C@@H](N)CC=1C=CC(O)=CC=1)C1=CC=CC=C1 ZHUJMSMQIPIPTF-IBURTVSXSA-N 0.000 description 1
- BUJAGSGYPOAWEI-SECBINFHSA-N (2r)-2-amino-n-(2,6-dimethylphenyl)propanamide Chemical compound C[C@@H](N)C(=O)NC1=C(C)C=CC=C1C BUJAGSGYPOAWEI-SECBINFHSA-N 0.000 description 1
- CHMUHOFITZIING-XNIJJKJLSA-N (2r,3r,4s,5r)-2-(6-aminopurin-9-yl)-2-cyclohexyl-5-(hydroxymethyl)oxolane-3,4-diol Chemical compound C1=NC=2C(N)=NC=NC=2N1[C@]1(C2CCCCC2)O[C@H](CO)[C@@H](O)[C@H]1O CHMUHOFITZIING-XNIJJKJLSA-N 0.000 description 1
- ZHWHMUIGIKPSJN-WOUKDFQISA-N (2r,3r,4s,5r)-2-(6-aminopurin-9-yl)-2-ethyl-5-(hydroxymethyl)oxolane-3,4-diol Chemical compound C1=NC2=C(N)N=CN=C2N1[C@]1(CC)O[C@H](CO)[C@@H](O)[C@H]1O ZHWHMUIGIKPSJN-WOUKDFQISA-N 0.000 description 1
- OESBDSFYJMDRJY-BAYCTPFLSA-N (2r,3s,4r,5r)-2-(hydroxymethyl)-5-[6-[[(3r)-oxolan-3-yl]amino]purin-9-yl]oxolane-3,4-diol Chemical compound O[C@@H]1[C@H](O)[C@@H](CO)O[C@H]1N1C2=NC=NC(N[C@H]3COCC3)=C2N=C1 OESBDSFYJMDRJY-BAYCTPFLSA-N 0.000 description 1
- XTYSXGHMTNTKFH-BDEHJDMKSA-N (2s)-1-[(2s,4r)-4-benzyl-2-hydroxy-5-[[(1s,2r)-2-hydroxy-2,3-dihydro-1h-inden-1-yl]amino]-5-oxopentyl]-n-tert-butyl-4-(pyridin-3-ylmethyl)piperazine-2-carboxamide;hydrate Chemical compound O.C([C@H](N(CC1)C[C@@H](O)C[C@@H](CC=2C=CC=CC=2)C(=O)N[C@H]2C3=CC=CC=C3C[C@H]2O)C(=O)NC(C)(C)C)N1CC1=CC=CN=C1 XTYSXGHMTNTKFH-BDEHJDMKSA-N 0.000 description 1
- LDYMCRRFCMRFKB-MOROJQBDSA-N (2s,3s,4r,5r)-5-[6-[(4-aminophenyl)methylamino]purin-9-yl]-3,4-dihydroxy-n-methyloxolane-2-carboxamide Chemical compound O[C@@H]1[C@H](O)[C@@H](C(=O)NC)O[C@H]1N1C2=NC=NC(NCC=3C=CC(N)=CC=3)=C2N=C1 LDYMCRRFCMRFKB-MOROJQBDSA-N 0.000 description 1
- METKIMKYRPQLGS-GFCCVEGCSA-N (R)-atenolol Chemical compound CC(C)NC[C@@H](O)COC1=CC=C(CC(N)=O)C=C1 METKIMKYRPQLGS-GFCCVEGCSA-N 0.000 description 1
- RTHCYVBBDHJXIQ-MRXNPFEDSA-N (R)-fluoxetine Chemical compound O([C@H](CCNC)C=1C=CC=CC=1)C1=CC=C(C(F)(F)F)C=C1 RTHCYVBBDHJXIQ-MRXNPFEDSA-N 0.000 description 1
- BJEPYKJPYRNKOW-REOHCLBHSA-N (S)-malic acid Chemical compound OC(=O)[C@@H](O)CC(O)=O BJEPYKJPYRNKOW-REOHCLBHSA-N 0.000 description 1
- PVHUJELLJLJGLN-INIZCTEOSA-N (S)-nitrendipine Chemical compound CCOC(=O)C1=C(C)NC(C)=C(C(=O)OC)[C@@H]1C1=CC=CC([N+]([O-])=O)=C1 PVHUJELLJLJGLN-INIZCTEOSA-N 0.000 description 1
- ZORQXIQZAOLNGE-UHFFFAOYSA-N 1,1-difluorocyclohexane Chemical compound FC1(F)CCCCC1 ZORQXIQZAOLNGE-UHFFFAOYSA-N 0.000 description 1
- XTFIVUDBNACUBN-UHFFFAOYSA-N 1,3,5-trinitro-1,3,5-triazinane Chemical compound [O-][N+](=O)N1CN([N+]([O-])=O)CN([N+]([O-])=O)C1 XTFIVUDBNACUBN-UHFFFAOYSA-N 0.000 description 1
- OGYGFUAIIOPWQD-UHFFFAOYSA-N 1,3-thiazolidine Chemical compound C1CSCN1 OGYGFUAIIOPWQD-UHFFFAOYSA-N 0.000 description 1
- YNGDWRXWKFWCJY-UHFFFAOYSA-N 1,4-Dihydropyridine Chemical class C1C=CNC=C1 YNGDWRXWKFWCJY-UHFFFAOYSA-N 0.000 description 1
- KMXPHBJUGYLXDM-LSDHHAIUSA-N 1-[(7r,8s)-7-hydroxy-6,6-dimethyl-7,8-dihydropyrano[2,3-f][2,1,3]benzoxadiazol-8-yl]piperidin-2-one Chemical compound N1([C@H]2C3=CC4=NON=C4C=C3OC([C@@H]2O)(C)C)CCCCC1=O KMXPHBJUGYLXDM-LSDHHAIUSA-N 0.000 description 1
- ULHFFAFDSSHFDA-UHFFFAOYSA-N 1-amino-2-ethoxybenzene Chemical compound CCOC1=CC=CC=C1N ULHFFAFDSSHFDA-UHFFFAOYSA-N 0.000 description 1
- RGPUSZZTRKTMNA-UHFFFAOYSA-N 1-benzofuran-7-carbaldehyde Chemical compound O=CC1=CC=CC2=C1OC=C2 RGPUSZZTRKTMNA-UHFFFAOYSA-N 0.000 description 1
- IVVNZDGDKPTYHK-JTQLQIEISA-N 1-cyano-2-[(2s)-3,3-dimethylbutan-2-yl]-3-pyridin-4-ylguanidine Chemical compound CC(C)(C)[C@H](C)N=C(NC#N)NC1=CC=NC=C1 IVVNZDGDKPTYHK-JTQLQIEISA-N 0.000 description 1
- IXPNQXFRVYWDDI-UHFFFAOYSA-N 1-methyl-2,4-dioxo-1,3-diazinane-5-carboximidamide Chemical compound CN1CC(C(N)=N)C(=O)NC1=O IXPNQXFRVYWDDI-UHFFFAOYSA-N 0.000 description 1
- IIZPXYDJLKNOIY-JXPKJXOSSA-N 1-palmitoyl-2-arachidonoyl-sn-glycero-3-phosphocholine Chemical compound CCCCCCCCCCCCCCCC(=O)OC[C@H](COP([O-])(=O)OCC[N+](C)(C)C)OC(=O)CCC\C=C/C\C=C/C\C=C/C\C=C/CCCCC IIZPXYDJLKNOIY-JXPKJXOSSA-N 0.000 description 1
- FPIPGXGPPPQFEQ-UHFFFAOYSA-N 13-cis retinol Natural products OCC=C(C)C=CC=C(C)C=CC1=C(C)CCCC1(C)C FPIPGXGPPPQFEQ-UHFFFAOYSA-N 0.000 description 1
- IHWDSEPNZDYMNF-UHFFFAOYSA-N 1H-indol-2-amine Chemical class C1=CC=C2NC(N)=CC2=C1 IHWDSEPNZDYMNF-UHFFFAOYSA-N 0.000 description 1
- DSCFFEYYQKSRSV-UHFFFAOYSA-N 1L-O1-methyl-muco-inositol Natural products COC1C(O)C(O)C(O)C(O)C1O DSCFFEYYQKSRSV-UHFFFAOYSA-N 0.000 description 1
- AWBOSXFRPFZLOP-UHFFFAOYSA-N 2,1,3-benzoxadiazole Chemical compound C1=CC=CC2=NON=C21 AWBOSXFRPFZLOP-UHFFFAOYSA-N 0.000 description 1
- IHPYMWDTONKSCO-UHFFFAOYSA-N 2,2'-piperazine-1,4-diylbisethanesulfonic acid Chemical compound OS(=O)(=O)CCN1CCN(CCS(O)(=O)=O)CC1 IHPYMWDTONKSCO-UHFFFAOYSA-N 0.000 description 1
- LPEPDWACHDVAIC-UHFFFAOYSA-N 2,2,6-trimethyl-4,7-dihydro-3h-indolo[2,3-c]quinolin-1-one Chemical compound C12=CC=CC=C2NC2=C1C(C(=O)C(C)(C)CC1)=C1N=C2C LPEPDWACHDVAIC-UHFFFAOYSA-N 0.000 description 1
- AEQDJSLRWYMAQI-UHFFFAOYSA-N 2,3,9,10-tetramethoxy-6,8,13,13a-tetrahydro-5H-isoquinolino[2,1-b]isoquinoline Chemical compound C1CN2CC(C(=C(OC)C=C3)OC)=C3CC2C2=C1C=C(OC)C(OC)=C2 AEQDJSLRWYMAQI-UHFFFAOYSA-N 0.000 description 1
- IAWXTSMHXFRLQR-UHFFFAOYSA-N 2,3-bis($l^{1}-oxidanyl)-7-nitroquinoxaline-6-carbonitrile Chemical compound O=C1C(=O)N=C2C=C(C#N)C([N+](=O)[O-])=CC2=N1 IAWXTSMHXFRLQR-UHFFFAOYSA-N 0.000 description 1
- JKMHFZQWWAIEOD-UHFFFAOYSA-N 2-[4-(2-hydroxyethyl)piperazin-1-yl]ethanesulfonic acid Chemical compound OCC[NH+]1CCN(CCS([O-])(=O)=O)CC1 JKMHFZQWWAIEOD-UHFFFAOYSA-N 0.000 description 1
- YSUBLPUJDOWYDP-UHFFFAOYSA-N 2-[4-[(2,5-difluorophenyl)methoxy]phenoxy]-5-ethoxyaniline Chemical compound NC1=CC(OCC)=CC=C1OC(C=C1)=CC=C1OCC1=CC(F)=CC=C1F YSUBLPUJDOWYDP-UHFFFAOYSA-N 0.000 description 1
- 125000000954 2-hydroxyethyl group Chemical group [H]C([*])([H])C([H])([H])O[H] 0.000 description 1
- GHCZTIFQWKKGSB-UHFFFAOYSA-N 2-hydroxypropane-1,2,3-tricarboxylic acid;phosphoric acid Chemical compound OP(O)(O)=O.OC(=O)CC(O)(C(O)=O)CC(O)=O GHCZTIFQWKKGSB-UHFFFAOYSA-N 0.000 description 1
- 125000004204 2-methoxyphenyl group Chemical group [H]C1=C([H])C(*)=C(OC([H])([H])[H])C([H])=C1[H] 0.000 description 1
- RIBYSHCVSQIIJE-UHFFFAOYSA-N 3-hydroxy-2,2-dimethyl-4-(1-methyl-6-oxopyridazin-3-yl)oxy-3,4-dihydrochromene-6-carbonitrile Chemical compound C1=CC(=O)N(C)N=C1OC1C2=CC(C#N)=CC=C2OC(C)(C)C1O RIBYSHCVSQIIJE-UHFFFAOYSA-N 0.000 description 1
- 125000004208 3-hydroxyphenyl group Chemical group [H]OC1=C([H])C([H])=C([H])C(*)=C1[H] 0.000 description 1
- MQNYRKWJSMQECI-QFIPXVFZSA-N 3-methyl-2-phenyl-N-[(1S)-1-phenylpropyl]-4-quinolinecarboxamide Chemical compound N([C@@H](CC)C=1C=CC=CC=1)C(=O)C(C1=CC=CC=C1N=1)=C(C)C=1C1=CC=CC=C1 MQNYRKWJSMQECI-QFIPXVFZSA-N 0.000 description 1
- 239000003477 4 aminobutyric acid receptor stimulating agent Substances 0.000 description 1
- LBLDMHBSVIVJPM-YZIHRLCOSA-N 4-[(R)-[(2S,5R)-2,5-dimethyl-4-prop-2-enyl-1-piperazinyl]-(3-hydroxyphenyl)methyl]-N,N-diethylbenzamide Chemical compound C1=CC(C(=O)N(CC)CC)=CC=C1[C@H](C=1C=C(O)C=CC=1)N1[C@@H](C)CN(CC=C)[C@H](C)C1 LBLDMHBSVIVJPM-YZIHRLCOSA-N 0.000 description 1
- KQWVAUSXZDRQPZ-UMTXDNHDSA-N 4-[(R)-[(2S,5R)-2,5-dimethyl-4-prop-2-enyl-1-piperazinyl]-(3-methoxyphenyl)methyl]-N,N-diethylbenzamide Chemical compound C1=CC(C(=O)N(CC)CC)=CC=C1[C@H](C=1C=C(OC)C=CC=1)N1[C@@H](C)CN(CC=C)[C@H](C)C1 KQWVAUSXZDRQPZ-UMTXDNHDSA-N 0.000 description 1
- DDSCNRYOJYAXOK-DUELTEGESA-N 4-[[(2r,5s)-4-[(r)-[4-(diethylcarbamoyl)phenyl]-(3-hydroxyphenyl)methyl]-2,5-dimethylpiperazin-1-yl]methyl]benzoic acid Chemical compound C1=CC(C(=O)N(CC)CC)=CC=C1[C@H](C=1C=C(O)C=CC=1)N1[C@@H](C)CN(CC=2C=CC(=CC=2)C(O)=O)[C@H](C)C1 DDSCNRYOJYAXOK-DUELTEGESA-N 0.000 description 1
- 101710169336 5'-deoxyadenosine deaminase Proteins 0.000 description 1
- GJOHLWZHWQUKAU-UHFFFAOYSA-N 5-azaniumylpentan-2-yl-(6-methoxyquinolin-8-yl)azanium;dihydrogen phosphate Chemical compound OP(O)(O)=O.OP(O)(O)=O.N1=CC=CC2=CC(OC)=CC(NC(C)CCCN)=C21 GJOHLWZHWQUKAU-UHFFFAOYSA-N 0.000 description 1
- SQDAZGGFXASXDW-UHFFFAOYSA-N 5-bromo-2-(trifluoromethoxy)pyridine Chemical compound FC(F)(F)OC1=CC=C(Br)C=N1 SQDAZGGFXASXDW-UHFFFAOYSA-N 0.000 description 1
- RZTAMFZIAATZDJ-HNNXBMFYSA-N 5-o-ethyl 3-o-methyl (4s)-4-(2,3-dichlorophenyl)-2,6-dimethyl-1,4-dihydropyridine-3,5-dicarboxylate Chemical compound CCOC(=O)C1=C(C)NC(C)=C(C(=O)OC)[C@@H]1C1=CC=CC(Cl)=C1Cl RZTAMFZIAATZDJ-HNNXBMFYSA-N 0.000 description 1
- MBAJNQDWJUHYOF-UHFFFAOYSA-N 7h-purin-6-amine;pyridine-3-carboxamide Chemical compound NC(=O)C1=CC=CN=C1.NC1=NC=NC2=C1NC=N2 MBAJNQDWJUHYOF-UHFFFAOYSA-N 0.000 description 1
- 208000030507 AIDS Diseases 0.000 description 1
- 244000215068 Acacia senegal Species 0.000 description 1
- 235000006491 Acacia senegal Nutrition 0.000 description 1
- QTBSBXVTEAMEQO-UHFFFAOYSA-M Acetate Chemical compound CC([O-])=O QTBSBXVTEAMEQO-UHFFFAOYSA-M 0.000 description 1
- 208000013824 Acidemia Diseases 0.000 description 1
- 241000251468 Actinopterygii Species 0.000 description 1
- 208000009304 Acute Kidney Injury Diseases 0.000 description 1
- 108010060263 Adenosine A1 Receptor Proteins 0.000 description 1
- 102000030814 Adenosine A1 receptor Human genes 0.000 description 1
- 102100036664 Adenosine deaminase Human genes 0.000 description 1
- 108050000203 Adenosine receptors Proteins 0.000 description 1
- 102000009346 Adenosine receptors Human genes 0.000 description 1
- 108010088751 Albumins Proteins 0.000 description 1
- 102000009027 Albumins Human genes 0.000 description 1
- 102100034452 Alternative prion protein Human genes 0.000 description 1
- QGZKDVFQNNGYKY-UHFFFAOYSA-O Ammonium Chemical compound [NH4+] QGZKDVFQNNGYKY-UHFFFAOYSA-O 0.000 description 1
- 206010002199 Anaphylactic shock Diseases 0.000 description 1
- 206010002388 Angina unstable Diseases 0.000 description 1
- 208000019901 Anxiety disease Diseases 0.000 description 1
- 206010060874 Aortic rupture Diseases 0.000 description 1
- 206010003011 Appendicitis Diseases 0.000 description 1
- 206010003662 Atrial flutter Diseases 0.000 description 1
- 206010003671 Atrioventricular Block Diseases 0.000 description 1
- 241000242587 Aurelia Species 0.000 description 1
- 208000023275 Autoimmune disease Diseases 0.000 description 1
- 206010070545 Bacterial translocation Diseases 0.000 description 1
- SLRNWACWRVGMKD-QMMMGPOBSA-N Balenine Chemical compound CN1C=NC(C[C@H](N=C(O)CCN)C(O)=O)=C1 SLRNWACWRVGMKD-QMMMGPOBSA-N 0.000 description 1
- 239000005711 Benzoic acid Substances 0.000 description 1
- 102000010183 Bradykinin receptor Human genes 0.000 description 1
- 108050001736 Bradykinin receptor Proteins 0.000 description 1
- 208000002381 Brain Hypoxia Diseases 0.000 description 1
- 201000006474 Brain Ischemia Diseases 0.000 description 1
- PAOANWZGLPPROA-RQXXJAGISA-N CGS-21680 Chemical compound O[C@@H]1[C@H](O)[C@@H](C(=O)NCC)O[C@H]1N1C2=NC(NCCC=3C=CC(CCC(O)=O)=CC=3)=NC(N)=C2N=C1 PAOANWZGLPPROA-RQXXJAGISA-N 0.000 description 1
- QAGYKUNXZHXKMR-UHFFFAOYSA-N CPD000469186 Natural products CC1=C(O)C=CC=C1C(=O)NC(C(O)CN1C(CC2CCCCC2C1)C(=O)NC(C)(C)C)CSC1=CC=CC=C1 QAGYKUNXZHXKMR-UHFFFAOYSA-N 0.000 description 1
- 102000003922 Calcium Channels Human genes 0.000 description 1
- 108090000312 Calcium Channels Proteins 0.000 description 1
- BHPQYMZQTOCNFJ-UHFFFAOYSA-N Calcium cation Chemical compound [Ca+2] BHPQYMZQTOCNFJ-UHFFFAOYSA-N 0.000 description 1
- 208000006017 Cardiac Tamponade Diseases 0.000 description 1
- 206010007558 Cardiac failure chronic Diseases 0.000 description 1
- 208000031229 Cardiomyopathies Diseases 0.000 description 1
- 208000024172 Cardiovascular disease Diseases 0.000 description 1
- QRYRORQUOLYVBU-VBKZILBWSA-N Carnosic acid Natural products CC([C@@H]1CC2)(C)CCC[C@]1(C(O)=O)C1=C2C=C(C(C)C)C(O)=C1O QRYRORQUOLYVBU-VBKZILBWSA-N 0.000 description 1
- 108010087806 Carnosine Proteins 0.000 description 1
- 241000426846 Carukia barnesi Species 0.000 description 1
- 241000426844 Carybdea xaymacana Species 0.000 description 1
- 102100035882 Catalase Human genes 0.000 description 1
- 108010053835 Catalase Proteins 0.000 description 1
- 241000700198 Cavia Species 0.000 description 1
- 206010065384 Cerebral hypoperfusion Diseases 0.000 description 1
- 206010008531 Chills Diseases 0.000 description 1
- 241000191257 Chironex fleckeri Species 0.000 description 1
- 229920001287 Chondroitin sulfate Polymers 0.000 description 1
- 208000006545 Chronic Obstructive Pulmonary Disease Diseases 0.000 description 1
- 208000002330 Congenital Heart Defects Diseases 0.000 description 1
- 206010010356 Congenital anomaly Diseases 0.000 description 1
- 241000237942 Conidae Species 0.000 description 1
- 241000237972 Conus geographus Species 0.000 description 1
- 241000242741 Cubozoa Species 0.000 description 1
- 241001126326 Cyanea <Cnidaria> Species 0.000 description 1
- 229930105110 Cyclosporin A Natural products 0.000 description 1
- PMATZTZNYRCHOR-CGLBZJNRSA-N Cyclosporin A Chemical compound CC[C@@H]1NC(=O)[C@H]([C@H](O)[C@H](C)C\C=C\C)N(C)C(=O)[C@H](C(C)C)N(C)C(=O)[C@H](CC(C)C)N(C)C(=O)[C@H](CC(C)C)N(C)C(=O)[C@@H](C)NC(=O)[C@H](C)NC(=O)[C@H](CC(C)C)N(C)C(=O)[C@H](C(C)C)NC(=O)[C@H](CC(C)C)N(C)C(=O)CN(C)C1=O PMATZTZNYRCHOR-CGLBZJNRSA-N 0.000 description 1
- 108010036949 Cyclosporine Proteins 0.000 description 1
- VJXUJFAZXQOXMJ-UHFFFAOYSA-N D-1-O-Methyl-muco-inositol Natural products CC12C(OC)(C)OC(C)(C)C2CC(=O)C(C23OC2C(=O)O2)(C)C1CCC3(C)C2C=1C=COC=1 VJXUJFAZXQOXMJ-UHFFFAOYSA-N 0.000 description 1
- ZZZCUOFIHGPKAK-UHFFFAOYSA-N D-erythro-ascorbic acid Natural products OCC1OC(=O)C(O)=C1O ZZZCUOFIHGPKAK-UHFFFAOYSA-N 0.000 description 1
- RGHNJXZEOKUKBD-SQOUGZDYSA-M D-gluconate Chemical compound OC[C@@H](O)[C@@H](O)[C@H](O)[C@@H](O)C([O-])=O RGHNJXZEOKUKBD-SQOUGZDYSA-M 0.000 description 1
- DSCFFEYYQKSRSV-KLJZZCKASA-N D-pinitol Chemical compound CO[C@@H]1[C@@H](O)[C@@H](O)[C@H](O)[C@H](O)[C@H]1O DSCFFEYYQKSRSV-KLJZZCKASA-N 0.000 description 1
- 235000008375 Decussocarpus nagi Nutrition 0.000 description 1
- 244000309456 Decussocarpus nagi Species 0.000 description 1
- 206010012218 Delirium Diseases 0.000 description 1
- 208000034423 Delivery Diseases 0.000 description 1
- 229920002307 Dextran Polymers 0.000 description 1
- 206010061818 Disease progression Diseases 0.000 description 1
- 208000002251 Dissecting Aneurysm Diseases 0.000 description 1
- 206010013647 Drowning Diseases 0.000 description 1
- 206010013654 Drug abuse Diseases 0.000 description 1
- DYEFUKCXAQOFHX-UHFFFAOYSA-N Ebselen Chemical compound [se]1C2=CC=CC=C2C(=O)N1C1=CC=CC=C1 DYEFUKCXAQOFHX-UHFFFAOYSA-N 0.000 description 1
- 206010014357 Electric shock Diseases 0.000 description 1
- 208000005189 Embolism Diseases 0.000 description 1
- 241000196324 Embryophyta Species 0.000 description 1
- 108010061435 Enalapril Proteins 0.000 description 1
- 208000004145 Endometritis Diseases 0.000 description 1
- 241000283073 Equus caballus Species 0.000 description 1
- UOACKFBJUYNSLK-XRKIENNPSA-N Estradiol Cypionate Chemical compound O([C@H]1CC[C@H]2[C@H]3[C@@H](C4=CC=C(O)C=C4CC3)CC[C@@]21C)C(=O)CCC1CCCC1 UOACKFBJUYNSLK-XRKIENNPSA-N 0.000 description 1
- 241000206602 Eukaryota Species 0.000 description 1
- 206010015719 Exsanguination Diseases 0.000 description 1
- YPZRHBJKEMOYQH-UYBVJOGSSA-N FADH2 Chemical compound C1=NC2=C(N)N=CN=C2N1[C@@H]([C@H](O)[C@@H]1O)O[C@@H]1COP(O)(=O)OP(O)(=O)OC[C@@H](O)[C@@H](O)[C@@H](O)CN1C(NC(=O)NC2=O)=C2NC2=C1C=C(C)C(C)=C2 YPZRHBJKEMOYQH-UYBVJOGSSA-N 0.000 description 1
- 108010071289 Factor XIII Proteins 0.000 description 1
- 241000282326 Felis catus Species 0.000 description 1
- 206010016654 Fibrosis Diseases 0.000 description 1
- DJBNUMBKLMJRSA-UHFFFAOYSA-N Flecainide Chemical compound FC(F)(F)COC1=CC=C(OCC(F)(F)F)C(C(=O)NCC2NCCCC2)=C1 DJBNUMBKLMJRSA-UHFFFAOYSA-N 0.000 description 1
- 102000003688 G-Protein-Coupled Receptors Human genes 0.000 description 1
- 108090000045 G-Protein-Coupled Receptors Proteins 0.000 description 1
- WMBWREPUVVBILR-UHFFFAOYSA-N GCG Natural products C=1C(O)=C(O)C(O)=CC=1C1OC2=CC(O)=CC(O)=C2CC1OC(=O)C1=CC(O)=C(O)C(O)=C1 WMBWREPUVVBILR-UHFFFAOYSA-N 0.000 description 1
- 241000237858 Gastropoda Species 0.000 description 1
- 108010010803 Gelatin Proteins 0.000 description 1
- 241001323797 Gerongia rifkinae Species 0.000 description 1
- 108010024636 Glutathione Proteins 0.000 description 1
- 239000004471 Glycine Substances 0.000 description 1
- NYHBQMYGNKIUIF-UUOKFMHZSA-N Guanosine Chemical compound C1=NC=2C(=O)NC(N)=NC=2N1[C@@H]1O[C@H](CO)[C@@H](O)[C@H]1O NYHBQMYGNKIUIF-UUOKFMHZSA-N 0.000 description 1
- 229920000084 Gum arabic Polymers 0.000 description 1
- 239000007995 HEPES buffer Substances 0.000 description 1
- 241000238894 Hadronyche versuta Species 0.000 description 1
- 241001157778 Haplopelma schmidti Species 0.000 description 1
- 206010019196 Head injury Diseases 0.000 description 1
- 102000008015 Hemeproteins Human genes 0.000 description 1
- 108010089792 Hemeproteins Proteins 0.000 description 1
- CPELXLSAUQHCOX-UHFFFAOYSA-N Hydrogen bromide Chemical class Br CPELXLSAUQHCOX-UHFFFAOYSA-N 0.000 description 1
- 241001136306 Hydrophiidae Species 0.000 description 1
- 229920001612 Hydroxyethyl starch Polymers 0.000 description 1
- 206010020843 Hyperthermia Diseases 0.000 description 1
- 206010021138 Hypovolaemic shock Diseases 0.000 description 1
- 241000245954 Hysterocrates gigas Species 0.000 description 1
- 206010061213 Iatrogenic injury Diseases 0.000 description 1
- HEFNNWSXXWATRW-UHFFFAOYSA-N Ibuprofen Chemical compound CC(C)CC1=CC=C(C(C)C(O)=O)C=C1 HEFNNWSXXWATRW-UHFFFAOYSA-N 0.000 description 1
- 108050000123 Inactive phospholipase C-like protein 1 Proteins 0.000 description 1
- 108010002352 Interleukin-1 Proteins 0.000 description 1
- 102000000589 Interleukin-1 Human genes 0.000 description 1
- 102000013462 Interleukin-12 Human genes 0.000 description 1
- 108010065805 Interleukin-12 Proteins 0.000 description 1
- 108090001007 Interleukin-8 Proteins 0.000 description 1
- 206010022773 Intracranial pressure increased Diseases 0.000 description 1
- KJHKTHWMRKYKJE-SUGCFTRWSA-N Kaletra Chemical compound N1([C@@H](C(C)C)C(=O)N[C@H](C[C@H](O)[C@H](CC=2C=CC=CC=2)NC(=O)COC=2C(=CC=CC=2C)C)CC=2C=CC=CC=2)CCCNC1=O KJHKTHWMRKYKJE-SUGCFTRWSA-N 0.000 description 1
- 239000012839 Krebs-Henseleit buffer Substances 0.000 description 1
- 101710103741 Kurtoxin Proteins 0.000 description 1
- PWKSKIMOESPYIA-BYPYZUCNSA-N L-N-acetyl-Cysteine Chemical compound CC(=O)N[C@@H](CS)C(O)=O PWKSKIMOESPYIA-BYPYZUCNSA-N 0.000 description 1
- 239000004201 L-cysteine Substances 0.000 description 1
- 235000013878 L-cysteine Nutrition 0.000 description 1
- HNDVDQJCIGZPNO-YFKPBYRVSA-N L-histidine Chemical compound OC(=O)[C@@H](N)CC1=CN=CN1 HNDVDQJCIGZPNO-YFKPBYRVSA-N 0.000 description 1
- 241001602180 Lamia Species 0.000 description 1
- 102000016469 Large-Conductance Calcium-Activated Potassium Channels Human genes 0.000 description 1
- 108010092555 Large-Conductance Calcium-Activated Potassium Channels Proteins 0.000 description 1
- 108010004028 Leucine-2-Alanine Enkephalin Proteins 0.000 description 1
- 239000000867 Lipoxygenase Inhibitor Substances 0.000 description 1
- WHXSMMKQMYFTQS-UHFFFAOYSA-N Lithium Chemical compound [Li] WHXSMMKQMYFTQS-UHFFFAOYSA-N 0.000 description 1
- 206010067125 Liver injury Diseases 0.000 description 1
- 208000009378 Low Cardiac Output Diseases 0.000 description 1
- 208000004852 Lung Injury Diseases 0.000 description 1
- UPYKUZBSLRQECL-UKMVMLAPSA-N Lycopene Natural products CC(=C/C=C/C=C(C)/C=C/C=C(C)/C=C/C1C(=C)CCCC1(C)C)C=CC=C(/C)C=CC2C(=C)CCCC2(C)C UPYKUZBSLRQECL-UKMVMLAPSA-N 0.000 description 1
- JEVVKJMRZMXFBT-XWDZUXABSA-N Lycophyll Natural products OC/C(=C/CC/C(=C\C=C\C(=C/C=C/C(=C\C=C\C=C(/C=C/C=C(\C=C\C=C(/CC/C=C(/CO)\C)\C)/C)\C)/C)\C)/C)/C JEVVKJMRZMXFBT-XWDZUXABSA-N 0.000 description 1
- 241000286819 Malo Species 0.000 description 1
- 241000124008 Mammalia Species 0.000 description 1
- 102000018697 Membrane Proteins Human genes 0.000 description 1
- 108010052285 Membrane Proteins Proteins 0.000 description 1
- AFVFQIVMOAPDHO-UHFFFAOYSA-N Methanesulfonic acid Chemical compound CS(O)(=O)=O AFVFQIVMOAPDHO-UHFFFAOYSA-N 0.000 description 1
- HBNPJJILLOYFJU-VMPREFPWSA-N Mibefradil Chemical compound C1CC2=CC(F)=CC=C2[C@H](C(C)C)[C@@]1(OC(=O)COC)CCN(C)CCCC1=NC2=CC=CC=C2N1 HBNPJJILLOYFJU-VMPREFPWSA-N 0.000 description 1
- ZFMITUMMTDLWHR-UHFFFAOYSA-N Minoxidil Chemical compound NC1=[N+]([O-])C(N)=CC(N2CCCCC2)=N1 ZFMITUMMTDLWHR-UHFFFAOYSA-N 0.000 description 1
- 241000039080 Morbakka Species 0.000 description 1
- 241000699666 Mus <mouse, genus> Species 0.000 description 1
- 206010069140 Myocardial depression Diseases 0.000 description 1
- 229940122960 Myosin inhibitor Drugs 0.000 description 1
- VLCDUOXHFNUCKK-UHFFFAOYSA-N N,N'-Dimethylthiourea Chemical compound CNC(=S)NC VLCDUOXHFNUCKK-UHFFFAOYSA-N 0.000 description 1
- 108090001041 N-Methyl-D-Aspartate Receptors Proteins 0.000 description 1
- 108090000699 N-Type Calcium Channels Proteins 0.000 description 1
- 102000004129 N-Type Calcium Channels Human genes 0.000 description 1
- UBQYURCVBFRUQT-UHFFFAOYSA-N N-benzoyl-Ferrioxamine B Chemical compound CC(=O)N(O)CCCCCNC(=O)CCC(=O)N(O)CCCCCNC(=O)CCC(=O)N(O)CCCCCN UBQYURCVBFRUQT-UHFFFAOYSA-N 0.000 description 1
- CQOVPNPJLQNMDC-UHFFFAOYSA-N N-beta-alanyl-L-histidine Natural products NCCC(=O)NC(C(O)=O)CC1=CN=CN1 CQOVPNPJLQNMDC-UHFFFAOYSA-N 0.000 description 1
- RNRMWTCECDHNQU-XYOKQWHBSA-N N-tert-butyl-1-(1-oxidopyridin-1-ium-4-yl)methanimine oxide Chemical compound CC(C)(C)[N+](\[O-])=C/C1=CC=[N+]([O-])C=C1 RNRMWTCECDHNQU-XYOKQWHBSA-N 0.000 description 1
- 229940124634 N-type calcium channel blocker Drugs 0.000 description 1
- BAWFJGJZGIEFAR-NNYOXOHSSA-N NAD zwitterion Chemical compound NC(=O)C1=CC=C[N+]([C@H]2[C@@H]([C@H](O)[C@@H](COP([O-])(=O)OP(O)(=O)OC[C@@H]3[C@H]([C@@H](O)[C@@H](O3)N3C4=NC=NC(N)=C4N=C3)O)O2)O)=C1 BAWFJGJZGIEFAR-NNYOXOHSSA-N 0.000 description 1
- 108010002998 NADPH Oxidases Proteins 0.000 description 1
- 102000004722 NADPH Oxidases Human genes 0.000 description 1
- 102000014649 NMDA glutamate receptor activity proteins Human genes 0.000 description 1
- CMWTZPSULFXXJA-UHFFFAOYSA-N Naproxen Natural products C1=C(C(C)C(O)=O)C=CC2=CC(OC)=CC=C21 CMWTZPSULFXXJA-UHFFFAOYSA-N 0.000 description 1
- 208000013901 Nephropathies and tubular disease Diseases 0.000 description 1
- 102000009493 Neurokinin receptors Human genes 0.000 description 1
- 108050000302 Neurokinin receptors Proteins 0.000 description 1
- 102000003797 Neuropeptides Human genes 0.000 description 1
- 108090000189 Neuropeptides Proteins 0.000 description 1
- 101100135355 Neurospora crassa (strain ATCC 24698 / 74-OR23-1A / CBS 708.71 / DSM 1257 / FGSC 987) pacc-1 gene Proteins 0.000 description 1
- PVNIIMVLHYAWGP-UHFFFAOYSA-N Niacin Chemical compound OC(=O)C1=CC=CN=C1 PVNIIMVLHYAWGP-UHFFFAOYSA-N 0.000 description 1
- UPMRZALMHVUCIN-UHFFFAOYSA-N Nitecapone Chemical compound CC(=O)C(C(C)=O)=CC1=CC(O)=C(O)C([N+]([O-])=O)=C1 UPMRZALMHVUCIN-UHFFFAOYSA-N 0.000 description 1
- 102000008299 Nitric Oxide Synthase Human genes 0.000 description 1
- 108010021487 Nitric Oxide Synthase Proteins 0.000 description 1
- 229940123134 Nitric oxide inhibitor Drugs 0.000 description 1
- 241000238413 Octopus Species 0.000 description 1
- 229940121954 Opioid receptor agonist Drugs 0.000 description 1
- 239000008896 Opium Substances 0.000 description 1
- 241000283973 Oryctolagus cuniculus Species 0.000 description 1
- 102000004316 Oxidoreductases Human genes 0.000 description 1
- 108090000854 Oxidoreductases Proteins 0.000 description 1
- 241000272104 Oxyuranus scutellatus scutellatus Species 0.000 description 1
- 108700012358 P/Q-type calcium channel Proteins 0.000 description 1
- 102000050761 P/Q-type calcium channel Human genes 0.000 description 1
- 102000016387 Pancreatic elastase Human genes 0.000 description 1
- 108010067372 Pancreatic elastase Proteins 0.000 description 1
- 240000001090 Papaver somniferum Species 0.000 description 1
- 235000008753 Papaver somniferum Nutrition 0.000 description 1
- 241001494479 Pecora Species 0.000 description 1
- 241000426956 Pelagia Species 0.000 description 1
- 206010034486 Pericarditis adhesive Diseases 0.000 description 1
- 102000012288 Phosphopyruvate Hydratase Human genes 0.000 description 1
- 108010022181 Phosphopyruvate Hydratase Proteins 0.000 description 1
- 102000015795 Platelet Membrane Glycoproteins Human genes 0.000 description 1
- 108010010336 Platelet Membrane Glycoproteins Proteins 0.000 description 1
- 206010035664 Pneumonia Diseases 0.000 description 1
- RVGRUAULSDPKGF-UHFFFAOYSA-N Poloxamer Chemical compound C1CO1.CC1CO1 RVGRUAULSDPKGF-UHFFFAOYSA-N 0.000 description 1
- 229920003171 Poly (ethylene oxide) Polymers 0.000 description 1
- 239000004698 Polyethylene Substances 0.000 description 1
- 229920002565 Polyethylene Glycol 400 Polymers 0.000 description 1
- 206010036416 Postpartum complications Diseases 0.000 description 1
- 241000210053 Potentilla elegans Species 0.000 description 1
- TUZYXOIXSAXUGO-UHFFFAOYSA-N Pravastatin Natural products C1=CC(C)C(CCC(O)CC(O)CC(O)=O)C2C(OC(=O)C(C)CC)CC(O)C=C21 TUZYXOIXSAXUGO-UHFFFAOYSA-N 0.000 description 1
- 206010062300 Procedural hypotension Diseases 0.000 description 1
- 229940124158 Protease/peptidase inhibitor Drugs 0.000 description 1
- 108010029485 Protein Isoforms Proteins 0.000 description 1
- 102000001708 Protein Isoforms Human genes 0.000 description 1
- 208000001431 Psychomotor Agitation Diseases 0.000 description 1
- 208000010378 Pulmonary Embolism Diseases 0.000 description 1
- 208000033626 Renal failure acute Diseases 0.000 description 1
- 206010061481 Renal injury Diseases 0.000 description 1
- 208000004756 Respiratory Insufficiency Diseases 0.000 description 1
- 206010038678 Respiratory depression Diseases 0.000 description 1
- 206010038743 Restlessness Diseases 0.000 description 1
- FTALBRSUTCGOEG-UHFFFAOYSA-N Riluzole Chemical compound C1=C(OC(F)(F)F)C=C2SC(N)=NC2=C1 FTALBRSUTCGOEG-UHFFFAOYSA-N 0.000 description 1
- NCDNCNXCDXHOMX-UHFFFAOYSA-N Ritonavir Natural products C=1C=CC=CC=1CC(NC(=O)OCC=1SC=NC=1)C(O)CC(CC=1C=CC=CC=1)NC(=O)C(C(C)C)NC(=O)N(C)CC1=CSC(C(C)C)=N1 NCDNCNXCDXHOMX-UHFFFAOYSA-N 0.000 description 1
- 241000220317 Rosa Species 0.000 description 1
- 102000011425 S100 Calcium Binding Protein beta Subunit Human genes 0.000 description 1
- 108010023918 S100 Calcium Binding Protein beta Subunit Proteins 0.000 description 1
- 208000006117 ST-elevation myocardial infarction Diseases 0.000 description 1
- 241000239226 Scorpiones Species 0.000 description 1
- BUGBHKTXTAQXES-UHFFFAOYSA-N Selenium Chemical compound [Se] BUGBHKTXTAQXES-UHFFFAOYSA-N 0.000 description 1
- 206010069141 Septic encephalopathy Diseases 0.000 description 1
- 208000004301 Sinus Arrhythmia Diseases 0.000 description 1
- 102000002582 Small-Conductance Calcium-Activated Potassium Channels Human genes 0.000 description 1
- 108010093479 Small-Conductance Calcium-Activated Potassium Channels Proteins 0.000 description 1
- 102100030980 Sodium/hydrogen exchanger 1 Human genes 0.000 description 1
- 206010041349 Somnolence Diseases 0.000 description 1
- 208000032851 Subarachnoid Hemorrhage Diseases 0.000 description 1
- 208000003734 Supraventricular Tachycardia Diseases 0.000 description 1
- 241000722085 Synanceia horrida Species 0.000 description 1
- 102000003691 T-Type Calcium Channels Human genes 0.000 description 1
- 108090000030 T-Type Calcium Channels Proteins 0.000 description 1
- 241000227521 Tamoya Species 0.000 description 1
- 208000021945 Tendon injury Diseases 0.000 description 1
- 241000906446 Theraps Species 0.000 description 1
- 206010052779 Transplant rejections Diseases 0.000 description 1
- 206010069363 Traumatic lung injury Diseases 0.000 description 1
- FNYLWPVRPXGIIP-UHFFFAOYSA-N Triamterene Chemical compound NC1=NC2=NC(N)=NC(N)=C2N=C1C1=CC=CC=C1 FNYLWPVRPXGIIP-UHFFFAOYSA-N 0.000 description 1
- GLEVLJDDWXEYCO-UHFFFAOYSA-N Trolox Chemical compound O1C(C)(C(O)=O)CCC2=C1C(C)=C(C)C(O)=C2C GLEVLJDDWXEYCO-UHFFFAOYSA-N 0.000 description 1
- 108060008683 Tumor Necrosis Factor Receptor Proteins 0.000 description 1
- 206010054094 Tumour necrosis Diseases 0.000 description 1
- 108090000848 Ubiquitin Proteins 0.000 description 1
- 102000044159 Ubiquitin Human genes 0.000 description 1
- 208000007814 Unstable Angina Diseases 0.000 description 1
- TVWHNULVHGKJHS-UHFFFAOYSA-N Uric acid Natural products N1C(=O)NC(=O)C2NC(=O)NC21 TVWHNULVHGKJHS-UHFFFAOYSA-N 0.000 description 1
- 206010047139 Vasoconstriction Diseases 0.000 description 1
- GXBMIBRIOWHPDT-UHFFFAOYSA-N Vasopressin Natural products N1C(=O)C(CC=2C=C(O)C=CC=2)NC(=O)C(N)CSSCC(C(=O)N2C(CCC2)C(=O)NC(CCCN=C(N)N)C(=O)NCC(N)=O)NC(=O)C(CC(N)=O)NC(=O)C(CCC(N)=O)NC(=O)C1CC1=CC=CC=C1 GXBMIBRIOWHPDT-UHFFFAOYSA-N 0.000 description 1
- 108010004977 Vasopressins Proteins 0.000 description 1
- 102000002852 Vasopressins Human genes 0.000 description 1
- 206010047163 Vasospasm Diseases 0.000 description 1
- 208000033774 Ventricular Remodeling Diseases 0.000 description 1
- FPIPGXGPPPQFEQ-BOOMUCAASA-N Vitamin A Natural products OC/C=C(/C)\C=C\C=C(\C)/C=C/C1=C(C)CCCC1(C)C FPIPGXGPPPQFEQ-BOOMUCAASA-N 0.000 description 1
- 229930003268 Vitamin C Natural products 0.000 description 1
- 206010048038 Wound infection Diseases 0.000 description 1
- LRFVTYWOQMYALW-UHFFFAOYSA-N Xanthine Natural products O=C1NC(=O)NC2=C1NC=N2 LRFVTYWOQMYALW-UHFFFAOYSA-N 0.000 description 1
- HCHKCACWOHOZIP-UHFFFAOYSA-N Zinc Chemical compound [Zn] HCHKCACWOHOZIP-UHFFFAOYSA-N 0.000 description 1
- YGCODSQDUUUKIV-UHFFFAOYSA-N Zoxazolamine Chemical compound ClC1=CC=C2OC(N)=NC2=C1 YGCODSQDUUUKIV-UHFFFAOYSA-N 0.000 description 1
- OBAAIGREYDUOHX-ZGOQAQPGSA-N [(2r,3s,4r,5r)-3,4-dihydroxy-5-[6-[[(3r)-oxolan-3-yl]amino]purin-9-yl]oxolan-2-yl]methyl n-ethylcarbamate Chemical compound O[C@@H]1[C@H](O)[C@@H](COC(=O)NCC)O[C@H]1N1C2=NC=NC(N[C@H]3COCC3)=C2N=C1 OBAAIGREYDUOHX-ZGOQAQPGSA-N 0.000 description 1
- WERKSKAQRVDLDW-ANOHMWSOSA-N [(2s,3r,4r,5r)-2,3,4,5,6-pentahydroxyhexyl] (z)-octadec-9-enoate Chemical compound CCCCCCCC\C=C/CCCCCCCC(=O)OC[C@H](O)[C@@H](O)[C@H](O)[C@H](O)CO WERKSKAQRVDLDW-ANOHMWSOSA-N 0.000 description 1
- 229960000446 abciximab Drugs 0.000 description 1
- 210000001015 abdomen Anatomy 0.000 description 1
- 208000002223 abdominal aortic aneurysm Diseases 0.000 description 1
- 230000003187 abdominal effect Effects 0.000 description 1
- 235000010489 acacia gum Nutrition 0.000 description 1
- 229960003000 acadesine Drugs 0.000 description 1
- WDJHALXBUFZDSR-UHFFFAOYSA-M acetoacetate Chemical compound CC(=O)CC([O-])=O WDJHALXBUFZDSR-UHFFFAOYSA-M 0.000 description 1
- 229940100228 acetyl coenzyme a Drugs 0.000 description 1
- 229960004308 acetylcysteine Drugs 0.000 description 1
- 239000012190 activator Substances 0.000 description 1
- 239000011149 active material Substances 0.000 description 1
- 201000011040 acute kidney failure Diseases 0.000 description 1
- 230000006978 adaptation Effects 0.000 description 1
- 229960000643 adenine Drugs 0.000 description 1
- 239000002582 adenosine A1 receptor agonist Substances 0.000 description 1
- 150000003838 adenosines Chemical class 0.000 description 1
- 210000001789 adipocyte Anatomy 0.000 description 1
- 239000000674 adrenergic antagonist Substances 0.000 description 1
- OENHQHLEOONYIE-UKMVMLAPSA-N all-trans beta-carotene Natural products CC=1CCCC(C)(C)C=1/C=C/C(/C)=C/C=C/C(/C)=C/C=C/C=C(C)C=CC=C(C)C=CC1=C(C)CCCC1(C)C OENHQHLEOONYIE-UKMVMLAPSA-N 0.000 description 1
- FPIPGXGPPPQFEQ-OVSJKPMPSA-N all-trans-retinol Chemical compound OC\C=C(/C)\C=C\C=C(/C)\C=C\C1=C(C)CCCC1(C)C FPIPGXGPPPQFEQ-OVSJKPMPSA-N 0.000 description 1
- 150000001408 amides Chemical class 0.000 description 1
- 229960000528 amlodipine Drugs 0.000 description 1
- HTIQEAQVCYTUBX-UHFFFAOYSA-N amlodipine Chemical compound CCOC(=O)C1=C(COCCN)NC(C)=C(C(=O)OC)C1C1=CC=CC=C1Cl HTIQEAQVCYTUBX-UHFFFAOYSA-N 0.000 description 1
- 150000003863 ammonium salts Chemical class 0.000 description 1
- 229960001830 amprenavir Drugs 0.000 description 1
- YMARZQAQMVYCKC-OEMFJLHTSA-N amprenavir Chemical compound C([C@@H]([C@H](O)CN(CC(C)C)S(=O)(=O)C=1C=CC(N)=CC=1)NC(=O)O[C@@H]1COCC1)C1=CC=CC=C1 YMARZQAQMVYCKC-OEMFJLHTSA-N 0.000 description 1
- 230000001195 anabolic effect Effects 0.000 description 1
- 230000036592 analgesia Effects 0.000 description 1
- 229940035676 analgesics Drugs 0.000 description 1
- 208000003455 anaphylaxis Diseases 0.000 description 1
- 238000002399 angioplasty Methods 0.000 description 1
- 150000008064 anhydrides Chemical class 0.000 description 1
- 150000001450 anions Chemical class 0.000 description 1
- 230000009517 anoxic brain damage Effects 0.000 description 1
- MYYIAHXIVFADCU-QMMMGPOBSA-N anserine Chemical compound CN1C=NC=C1C[C@H](NC(=O)CC[NH3+])C([O-])=O MYYIAHXIVFADCU-QMMMGPOBSA-N 0.000 description 1
- 239000000730 antalgic agent Substances 0.000 description 1
- 230000001455 anti-clotting effect Effects 0.000 description 1
- 230000003276 anti-hypertensive effect Effects 0.000 description 1
- 238000011861 anti-inflammatory therapy Methods 0.000 description 1
- 230000001028 anti-proliverative effect Effects 0.000 description 1
- 230000000259 anti-tumor effect Effects 0.000 description 1
- 230000009016 anticipatory response Effects 0.000 description 1
- 229940127090 anticoagulant agent Drugs 0.000 description 1
- 229940127219 anticoagulant drug Drugs 0.000 description 1
- 108010065183 antilipopolysaccharide antibodies Proteins 0.000 description 1
- 230000036506 anxiety Effects 0.000 description 1
- 206010002895 aortic dissection Diseases 0.000 description 1
- 229950005617 aprikalim Drugs 0.000 description 1
- 239000007864 aqueous solution Substances 0.000 description 1
- 208000037849 arterial hypertension Diseases 0.000 description 1
- 230000001174 ascending effect Effects 0.000 description 1
- 229940072107 ascorbate Drugs 0.000 description 1
- 229960005070 ascorbic acid Drugs 0.000 description 1
- 125000003289 ascorbyl group Chemical group [H]O[C@@]([H])(C([H])([H])O*)[C@@]1([H])OC(=O)C(O*)=C1O* 0.000 description 1
- 229960002274 atenolol Drugs 0.000 description 1
- 230000001746 atrial effect Effects 0.000 description 1
- 230000001363 autoimmune Effects 0.000 description 1
- 230000037424 autonomic function Effects 0.000 description 1
- 210000003403 autonomic nervous system Anatomy 0.000 description 1
- 210000000467 autonomic pathway Anatomy 0.000 description 1
- 230000007375 bacterial translocation Effects 0.000 description 1
- WXBLLCUINBKULX-UHFFFAOYSA-N benzoic acid Chemical compound OC(=O)C1=CC=CC=C1.OC(=O)C1=CC=CC=C1 WXBLLCUINBKULX-UHFFFAOYSA-N 0.000 description 1
- 235000010233 benzoic acid Nutrition 0.000 description 1
- 150000001558 benzoic acid derivatives Chemical class 0.000 description 1
- 125000003236 benzoyl group Chemical group [H]C1=C([H])C([H])=C(C([H])=C1[H])C(*)=O 0.000 description 1
- 125000001797 benzyl group Chemical group [H]C1=C([H])C([H])=C(C([H])=C1[H])C([H])([H])* 0.000 description 1
- 235000013734 beta-carotene Nutrition 0.000 description 1
- 239000011648 beta-carotene Substances 0.000 description 1
- TUPZEYHYWIEDIH-WAIFQNFQSA-N beta-carotene Natural products CC(=C/C=C/C=C(C)/C=C/C=C(C)/C=C/C1=C(C)CCCC1(C)C)C=CC=C(/C)C=CC2=CCCCC2(C)C TUPZEYHYWIEDIH-WAIFQNFQSA-N 0.000 description 1
- 229960002747 betacarotene Drugs 0.000 description 1
- 230000002146 bilateral effect Effects 0.000 description 1
- 229940093797 bioflavonoids Drugs 0.000 description 1
- 230000023555 blood coagulation Effects 0.000 description 1
- 238000009530 blood pressure measurement Methods 0.000 description 1
- 210000000988 bone and bone Anatomy 0.000 description 1
- 230000008344 brain blood flow Effects 0.000 description 1
- 210000004781 brain capillary Anatomy 0.000 description 1
- 210000004958 brain cell Anatomy 0.000 description 1
- 208000025698 brain inflammatory disease Diseases 0.000 description 1
- 230000007052 brain toxicity Effects 0.000 description 1
- 210000000481 breast Anatomy 0.000 description 1
- 230000003139 buffering effect Effects 0.000 description 1
- 229940088033 calan Drugs 0.000 description 1
- 229960005069 calcium Drugs 0.000 description 1
- 230000004094 calcium homeostasis Effects 0.000 description 1
- 229910001424 calcium ion Inorganic materials 0.000 description 1
- 230000002213 calciumantagonistic effect Effects 0.000 description 1
- 244000309466 calf Species 0.000 description 1
- FAKRSMQSSFJEIM-RQJHMYQMSA-N captopril Chemical group SC[C@@H](C)C(=O)N1CCC[C@H]1C(O)=O FAKRSMQSSFJEIM-RQJHMYQMSA-N 0.000 description 1
- 229960000830 captopril Drugs 0.000 description 1
- FFGPTBGBLSHEPO-UHFFFAOYSA-N carbamazepine Chemical compound C1=CC2=CC=CC=C2N(C(=O)N)C2=CC=CC=C21 FFGPTBGBLSHEPO-UHFFFAOYSA-N 0.000 description 1
- 229960000623 carbamazepine Drugs 0.000 description 1
- 239000004202 carbamide Substances 0.000 description 1
- DKVNPHBNOWQYFE-UHFFFAOYSA-N carbamodithioic acid Chemical compound NC(S)=S DKVNPHBNOWQYFE-UHFFFAOYSA-N 0.000 description 1
- 125000003178 carboxy group Chemical group [H]OC(*)=O 0.000 description 1
- 210000005242 cardiac chamber Anatomy 0.000 description 1
- 230000003683 cardiac damage Effects 0.000 description 1
- 206010061592 cardiac fibrillation Diseases 0.000 description 1
- 230000001269 cardiogenic effect Effects 0.000 description 1
- 230000002802 cardiorespiratory effect Effects 0.000 description 1
- 229940088029 cardizem Drugs 0.000 description 1
- 229950008393 cariporide Drugs 0.000 description 1
- 229940044199 carnosine Drugs 0.000 description 1
- CQOVPNPJLQNMDC-ZETCQYMHSA-N carnosine Chemical compound [NH3+]CCC(=O)N[C@H](C([O-])=O)CC1=CNC=N1 CQOVPNPJLQNMDC-ZETCQYMHSA-N 0.000 description 1
- 235000021466 carotenoid Nutrition 0.000 description 1
- 150000001747 carotenoids Chemical class 0.000 description 1
- 210000001168 carotid artery common Anatomy 0.000 description 1
- 150000003943 catecholamines Chemical class 0.000 description 1
- 150000001768 cations Chemical class 0.000 description 1
- 230000001364 causal effect Effects 0.000 description 1
- 231100000976 cerebrotoxicity Toxicity 0.000 description 1
- 208000026106 cerebrovascular disease Diseases 0.000 description 1
- OEUUFNIKLCFNLN-LLVKDONJSA-N chembl432481 Chemical compound OC(=O)[C@@]1(C)CSC(C=2C(=CC(O)=CC=2)O)=N1 OEUUFNIKLCFNLN-LLVKDONJSA-N 0.000 description 1
- 238000006243 chemical reaction Methods 0.000 description 1
- 108091008690 chemoreceptors Proteins 0.000 description 1
- QZXCCPZJCKEPSA-UHFFFAOYSA-N chlorfenac Chemical compound OC(=O)CC1=C(Cl)C=CC(Cl)=C1Cl QZXCCPZJCKEPSA-UHFFFAOYSA-N 0.000 description 1
- TZFWDZFKRBELIQ-UHFFFAOYSA-N chlorzoxazone Chemical compound ClC1=CC=C2OC(O)=NC2=C1 TZFWDZFKRBELIQ-UHFFFAOYSA-N 0.000 description 1
- 229960003633 chlorzoxazone Drugs 0.000 description 1
- 229940059329 chondroitin sulfate Drugs 0.000 description 1
- 208000020832 chronic kidney disease Diseases 0.000 description 1
- 229960001265 ciclosporin Drugs 0.000 description 1
- LOUPRKONTZGTKE-UHFFFAOYSA-N cinchonine Natural products C1C(C(C2)C=C)CCN2C1C(O)C1=CC=NC2=CC=C(OC)C=C21 LOUPRKONTZGTKE-UHFFFAOYSA-N 0.000 description 1
- 229960004106 citric acid Drugs 0.000 description 1
- 238000003759 clinical diagnosis Methods 0.000 description 1
- 235000017471 coenzyme Q10 Nutrition 0.000 description 1
- 230000007278 cognition impairment Effects 0.000 description 1
- 230000001149 cognitive effect Effects 0.000 description 1
- 238000004891 communication Methods 0.000 description 1
- 229920002770 condensed tannin Polymers 0.000 description 1
- 208000028831 congenital heart disease Diseases 0.000 description 1
- 210000004351 coronary vessel Anatomy 0.000 description 1
- 238000012937 correction Methods 0.000 description 1
- 230000001054 cortical effect Effects 0.000 description 1
- ILVITZMPXQQPBD-OFAXGOBFSA-N crobenetine Chemical compound O([C@H](CN1[C@@H]2CC3=CC=CC=C3[C@@H](C2(C)C)CC1)C)CC1=CC=CC=C1 ILVITZMPXQQPBD-OFAXGOBFSA-N 0.000 description 1
- 229950005056 crobenetine Drugs 0.000 description 1
- 235000012754 curcumin Nutrition 0.000 description 1
- 239000004148 curcumin Substances 0.000 description 1
- 229940109262 curcumin Drugs 0.000 description 1
- 210000004292 cytoskeleton Anatomy 0.000 description 1
- 210000000172 cytosol Anatomy 0.000 description 1
- 230000001086 cytosolic effect Effects 0.000 description 1
- 210000003785 decidua Anatomy 0.000 description 1
- 239000008367 deionised water Substances 0.000 description 1
- 239000003405 delayed action preparation Substances 0.000 description 1
- 239000000841 delta opiate receptor agonist Substances 0.000 description 1
- 230000002999 depolarising effect Effects 0.000 description 1
- 230000008021 deposition Effects 0.000 description 1
- 229940099217 desferal Drugs 0.000 description 1
- 229940119744 dextran 40 Drugs 0.000 description 1
- 238000003745 diagnosis Methods 0.000 description 1
- VFLDPWHFBUODDF-UHFFFAOYSA-N diferuloylmethane Natural products C1=C(O)C(OC)=CC(C=CC(=O)CC(=O)C=CC=2C=C(OC)C(O)=CC=2)=C1 VFLDPWHFBUODDF-UHFFFAOYSA-N 0.000 description 1
- NSNHWTBQMQIDCF-UHFFFAOYSA-N dihydrate;hydrochloride Chemical compound O.O.Cl NSNHWTBQMQIDCF-UHFFFAOYSA-N 0.000 description 1
- 230000010339 dilation Effects 0.000 description 1
- 230000003292 diminished effect Effects 0.000 description 1
- 230000005750 disease progression Effects 0.000 description 1
- UVTNFZQICZKOEM-UHFFFAOYSA-N disopyramide Chemical compound C=1C=CC=NC=1C(C(N)=O)(CCN(C(C)C)C(C)C)C1=CC=CC=C1 UVTNFZQICZKOEM-UHFFFAOYSA-N 0.000 description 1
- 229960001066 disopyramide Drugs 0.000 description 1
- 208000035475 disorder Diseases 0.000 description 1
- 238000002224 dissection Methods 0.000 description 1
- 238000009826 distribution Methods 0.000 description 1
- MAHNFPMIPQKPPI-UHFFFAOYSA-N disulfur Chemical compound S=S MAHNFPMIPQKPPI-UHFFFAOYSA-N 0.000 description 1
- 239000012990 dithiocarbamate Substances 0.000 description 1
- 208000007784 diverticulitis Diseases 0.000 description 1
- 230000003828 downregulation Effects 0.000 description 1
- 238000009509 drug development Methods 0.000 description 1
- 230000009977 dual effect Effects 0.000 description 1
- JMNJYGMAUMANNW-FIXZTSJVSA-N dynorphin a Chemical compound C([C@@H](C(=O)N[C@@H](CC(C)C)C(=O)N[C@@H](CCCNC(N)=N)C(=O)N[C@@H](CCCNC(N)=N)C(=O)N[C@@H]([C@@H](C)CC)C(=O)N[C@@H](CCCNC(N)=N)C(=O)N1[C@@H](CCC1)C(=O)N[C@@H](CCCCN)C(=O)N[C@@H](CC(C)C)C(=O)N[C@@H](CCCCN)C(=O)N[C@@H](CC=1C2=CC=CC=C2NC=1)C(=O)N[C@@H](CC(O)=O)C(=O)N[C@@H](CC(N)=O)C(=O)N[C@@H](CCC(N)=O)C(O)=O)NC(=O)CNC(=O)CNC(=O)[C@@H](N)CC=1C=CC(O)=CC=1)C1=CC=CC=C1 JMNJYGMAUMANNW-FIXZTSJVSA-N 0.000 description 1
- 229950010033 ebselen Drugs 0.000 description 1
- 230000005611 electricity Effects 0.000 description 1
- 239000003792 electrolyte Substances 0.000 description 1
- 239000003974 emollient agent Substances 0.000 description 1
- 239000003995 emulsifying agent Substances 0.000 description 1
- GBXSMTUPTTWBMN-XIRDDKMYSA-N enalapril Chemical compound C([C@@H](C(=O)OCC)N[C@@H](C)C(=O)N1[C@@H](CCC1)C(O)=O)CC1=CC=CC=C1 GBXSMTUPTTWBMN-XIRDDKMYSA-N 0.000 description 1
- 229960000873 enalapril Drugs 0.000 description 1
- 206010014665 endocarditis Diseases 0.000 description 1
- 230000002124 endocrine Effects 0.000 description 1
- 230000007368 endocrine function Effects 0.000 description 1
- 230000008753 endothelial function Effects 0.000 description 1
- 238000005516 engineering process Methods 0.000 description 1
- 230000002708 enhancing effect Effects 0.000 description 1
- 229950011365 eniporide Drugs 0.000 description 1
- 229960000610 enoxaparin Drugs 0.000 description 1
- 231100000740 envenomation Toxicity 0.000 description 1
- 230000007613 environmental effect Effects 0.000 description 1
- 229940030275 epigallocatechin gallate Drugs 0.000 description 1
- 210000000981 epithelium Anatomy 0.000 description 1
- 210000003743 erythrocyte Anatomy 0.000 description 1
- 150000002170 ethers Chemical class 0.000 description 1
- 125000001495 ethyl group Chemical group [H]C([H])([H])C([H])([H])* 0.000 description 1
- QDERNBXNXJCIQK-UHFFFAOYSA-N ethylisopropylamiloride Chemical compound CCN(C(C)C)C1=NC(N)=C(C(=O)N=C(N)N)N=C1Cl QDERNBXNXJCIQK-UHFFFAOYSA-N 0.000 description 1
- 238000011156 evaluation Methods 0.000 description 1
- 210000001723 extracellular space Anatomy 0.000 description 1
- PCOBBVZJEWWZFR-UHFFFAOYSA-N ezogabine Chemical compound C1=C(N)C(NC(=O)OCC)=CC=C1NCC1=CC=C(F)C=C1 PCOBBVZJEWWZFR-UHFFFAOYSA-N 0.000 description 1
- 229940012444 factor xiii Drugs 0.000 description 1
- 206010016256 fatigue Diseases 0.000 description 1
- 229960003580 felodipine Drugs 0.000 description 1
- 229960002428 fentanyl Drugs 0.000 description 1
- IVLVTNPOHDFFCJ-UHFFFAOYSA-N fentanyl citrate Chemical compound OC(=O)CC(O)(C(O)=O)CC(O)=O.C=1C=CC=CC=1N(C(=O)CC)C(CC1)CCN1CCC1=CC=CC=C1 IVLVTNPOHDFFCJ-UHFFFAOYSA-N 0.000 description 1
- 230000002600 fibrillogenic effect Effects 0.000 description 1
- 230000020764 fibrinolysis Effects 0.000 description 1
- 230000004761 fibrosis Effects 0.000 description 1
- 238000011049 filling Methods 0.000 description 1
- 238000009093 first-line therapy Methods 0.000 description 1
- 229930003935 flavonoid Natural products 0.000 description 1
- 150000002215 flavonoids Chemical class 0.000 description 1
- 235000017173 flavonoids Nutrition 0.000 description 1
- 229960000449 flecainide Drugs 0.000 description 1
- 238000002637 fluid replacement therapy Methods 0.000 description 1
- 229960002464 fluoxetine Drugs 0.000 description 1
- 239000006260 foam Substances 0.000 description 1
- 235000013355 food flavoring agent Nutrition 0.000 description 1
- 235000021588 free fatty acids Nutrition 0.000 description 1
- 239000004023 fresh frozen plasma Substances 0.000 description 1
- 210000001652 frontal lobe Anatomy 0.000 description 1
- 235000011389 fruit/vegetable juice Nutrition 0.000 description 1
- 230000002538 fungal effect Effects 0.000 description 1
- 229960003692 gamma aminobutyric acid Drugs 0.000 description 1
- BTCSSZJGUNDROE-UHFFFAOYSA-N gamma-aminobutyric acid Chemical compound NCCCC(O)=O BTCSSZJGUNDROE-UHFFFAOYSA-N 0.000 description 1
- 239000007789 gas Substances 0.000 description 1
- 239000008273 gelatin Substances 0.000 description 1
- 229920000159 gelatin Polymers 0.000 description 1
- 235000019322 gelatine Nutrition 0.000 description 1
- 235000011852 gelatine desserts Nutrition 0.000 description 1
- 230000002068 genetic effect Effects 0.000 description 1
- 229940050410 gluconate Drugs 0.000 description 1
- 230000004153 glucose metabolism Effects 0.000 description 1
- 230000004190 glucose uptake Effects 0.000 description 1
- 229960003180 glutathione Drugs 0.000 description 1
- 230000002641 glycemic effect Effects 0.000 description 1
- 108010093115 growth factor-activatable Na-H exchanger NHE-1 Proteins 0.000 description 1
- 229920000591 gum Polymers 0.000 description 1
- 229940093915 gynecological organic acid Drugs 0.000 description 1
- 230000001435 haemodynamic effect Effects 0.000 description 1
- 210000002837 heart atrium Anatomy 0.000 description 1
- 210000005003 heart tissue Anatomy 0.000 description 1
- 210000003709 heart valve Anatomy 0.000 description 1
- 230000020169 heat generation Effects 0.000 description 1
- 208000011316 hemodynamic instability Diseases 0.000 description 1
- 231100000234 hepatic damage Toxicity 0.000 description 1
- 210000003494 hepatocyte Anatomy 0.000 description 1
- 230000028974 hepatocyte apoptotic process Effects 0.000 description 1
- 229940027278 hetastarch Drugs 0.000 description 1
- HNDVDQJCIGZPNO-UHFFFAOYSA-N histidine Natural products OC(=O)C(N)CC1=CN=CN1 HNDVDQJCIGZPNO-UHFFFAOYSA-N 0.000 description 1
- 239000005556 hormone Substances 0.000 description 1
- 229940088597 hormone Drugs 0.000 description 1
- 235000003642 hunger Nutrition 0.000 description 1
- 229960000890 hydrocortisone Drugs 0.000 description 1
- 230000002209 hydrophobic effect Effects 0.000 description 1
- UWYVPFMHMJIBHE-OWOJBTEDSA-N hydroxymaleic acid group Chemical group O/C(/C(=O)O)=C/C(=O)O UWYVPFMHMJIBHE-OWOJBTEDSA-N 0.000 description 1
- 239000002471 hydroxymethylglutaryl coenzyme A reductase inhibitor Substances 0.000 description 1
- 230000036031 hyperthermia Effects 0.000 description 1
- 239000000076 hypertonic saline solution Substances 0.000 description 1
- 210000003016 hypothalamus Anatomy 0.000 description 1
- 230000001146 hypoxic effect Effects 0.000 description 1
- 229960001680 ibuprofen Drugs 0.000 description 1
- 229960002240 iloprost Drugs 0.000 description 1
- HIFJCPQKFCZDDL-ACWOEMLNSA-N iloprost Chemical compound C1\C(=C/CCCC(O)=O)C[C@@H]2[C@@H](/C=C/[C@@H](O)C(C)CC#CC)[C@H](O)C[C@@H]21 HIFJCPQKFCZDDL-ACWOEMLNSA-N 0.000 description 1
- BCGWQEUPMDMJNV-UHFFFAOYSA-N imipramine Chemical compound C1CC2=CC=CC=C2N(CCCN(C)C)C2=CC=CC=C21 BCGWQEUPMDMJNV-UHFFFAOYSA-N 0.000 description 1
- 229960004801 imipramine Drugs 0.000 description 1
- 230000005934 immune activation Effects 0.000 description 1
- 230000008073 immune recognition Effects 0.000 description 1
- 230000028993 immune response Effects 0.000 description 1
- 208000026278 immune system disease Diseases 0.000 description 1
- 239000000367 immunologic factor Substances 0.000 description 1
- 230000003308 immunostimulating effect Effects 0.000 description 1
- 230000001771 impaired effect Effects 0.000 description 1
- 238000002513 implantation Methods 0.000 description 1
- 229960001936 indinavir Drugs 0.000 description 1
- 229960000905 indomethacin Drugs 0.000 description 1
- 230000008595 infiltration Effects 0.000 description 1
- 238000001764 infiltration Methods 0.000 description 1
- 230000004941 influx Effects 0.000 description 1
- 239000003978 infusion fluid Substances 0.000 description 1
- 239000003999 initiator Substances 0.000 description 1
- 230000000977 initiatory effect Effects 0.000 description 1
- 230000000266 injurious effect Effects 0.000 description 1
- 230000010354 integration Effects 0.000 description 1
- 201000004332 intermediate coronary syndrome Diseases 0.000 description 1
- 210000004347 intestinal mucosa Anatomy 0.000 description 1
- 238000001361 intraarterial administration Methods 0.000 description 1
- 239000007927 intramuscular injection Substances 0.000 description 1
- 238000010253 intravenous injection Methods 0.000 description 1
- 239000003456 ion exchange resin Substances 0.000 description 1
- 229920003303 ion-exchange polymer Polymers 0.000 description 1
- 230000001788 irregular Effects 0.000 description 1
- 229960004427 isradipine Drugs 0.000 description 1
- 235000015110 jellies Nutrition 0.000 description 1
- 239000008274 jelly Substances 0.000 description 1
- 239000002632 kappa opiate receptor agonist Substances 0.000 description 1
- 229940126470 kappa opioid receptor agonist Drugs 0.000 description 1
- 210000003292 kidney cell Anatomy 0.000 description 1
- 210000003127 knee Anatomy 0.000 description 1
- 229940099584 lactobionate Drugs 0.000 description 1
- JYTUSYBCFIZPBE-AMTLMPIISA-N lactobionic acid Chemical compound OC(=O)[C@H](O)[C@@H](O)[C@@H]([C@H](O)CO)O[C@@H]1O[C@H](CO)[C@H](O)[C@H](O)[C@H]1O JYTUSYBCFIZPBE-AMTLMPIISA-N 0.000 description 1
- 239000000787 lecithin Substances 0.000 description 1
- 229940067606 lecithin Drugs 0.000 description 1
- 235000010445 lecithin Nutrition 0.000 description 1
- 210000005240 left ventricle Anatomy 0.000 description 1
- 230000003902 lesion Effects 0.000 description 1
- 230000002197 limbic effect Effects 0.000 description 1
- 229920006008 lipopolysaccharide Polymers 0.000 description 1
- 239000007791 liquid phase Substances 0.000 description 1
- 229910052744 lithium Inorganic materials 0.000 description 1
- 229960001078 lithium Drugs 0.000 description 1
- 230000008818 liver damage Effects 0.000 description 1
- 244000144972 livestock Species 0.000 description 1
- 239000003589 local anesthetic agent Substances 0.000 description 1
- 229960005015 local anesthetics Drugs 0.000 description 1
- 229960004525 lopinavir Drugs 0.000 description 1
- 239000003055 low molecular weight heparin Substances 0.000 description 1
- 229940127215 low-molecular weight heparin Drugs 0.000 description 1
- 231100000515 lung injury Toxicity 0.000 description 1
- 235000012680 lutein Nutrition 0.000 description 1
- 229960005375 lutein Drugs 0.000 description 1
- 239000001656 lutein Substances 0.000 description 1
- KBPHJBAIARWVSC-RGZFRNHPSA-N lutein Chemical compound C([C@H](O)CC=1C)C(C)(C)C=1\C=C\C(\C)=C\C=C\C(\C)=C\C=C\C=C(/C)\C=C\C=C(/C)\C=C\[C@H]1C(C)=C[C@H](O)CC1(C)C KBPHJBAIARWVSC-RGZFRNHPSA-N 0.000 description 1
- ORAKUVXRZWMARG-WZLJTJAWSA-N lutein Natural products CC(=C/C=C/C=C(C)/C=C/C=C(C)/C=C/C1=C(C)CCCC1(C)C)C=CC=C(/C)C=CC2C(=CC(O)CC2(C)C)C ORAKUVXRZWMARG-WZLJTJAWSA-N 0.000 description 1
- 235000012661 lycopene Nutrition 0.000 description 1
- 229960004999 lycopene Drugs 0.000 description 1
- 239000001751 lycopene Substances 0.000 description 1
- OAIJSZIZWZSQBC-GYZMGTAESA-N lycopene Chemical compound CC(C)=CCC\C(C)=C\C=C\C(\C)=C\C=C\C(\C)=C\C=C\C=C(/C)\C=C\C=C(/C)\C=C\C=C(/C)CCC=C(C)C OAIJSZIZWZSQBC-GYZMGTAESA-N 0.000 description 1
- 229910001629 magnesium chloride Inorganic materials 0.000 description 1
- 238000012423 maintenance Methods 0.000 description 1
- 230000003211 malignant effect Effects 0.000 description 1
- 229960001855 mannitol Drugs 0.000 description 1
- 239000000463 material Substances 0.000 description 1
- 230000008774 maternal effect Effects 0.000 description 1
- 238000005399 mechanical ventilation Methods 0.000 description 1
- 230000010534 mechanism of action Effects 0.000 description 1
- 201000001231 mediastinitis Diseases 0.000 description 1
- 239000002609 medium Substances 0.000 description 1
- 230000003340 mental effect Effects 0.000 description 1
- 230000037323 metabolic rate Effects 0.000 description 1
- 239000002207 metabolite Substances 0.000 description 1
- WGIKEBHIKKWJLG-UHFFFAOYSA-N methanesulfonic acid;2-[4-[(4-nitrophenyl)methoxy]phenyl]ethyl carbamimidothioate Chemical compound CS(O)(=O)=O.C1=CC(CCSC(=N)N)=CC=C1OCC1=CC=C([N+]([O-])=O)C=C1 WGIKEBHIKKWJLG-UHFFFAOYSA-N 0.000 description 1
- 125000000956 methoxy group Chemical group [H]C([H])([H])O* 0.000 description 1
- VKQFCGNPDRICFG-UHFFFAOYSA-N methyl 2-methylpropyl 2,6-dimethyl-4-(2-nitrophenyl)-1,4-dihydropyridine-3,5-dicarboxylate Chemical compound COC(=O)C1=C(C)NC(C)=C(C(=O)OCC(C)C)C1C1=CC=CC=C1[N+]([O-])=O VKQFCGNPDRICFG-UHFFFAOYSA-N 0.000 description 1
- 229920000609 methyl cellulose Polymers 0.000 description 1
- 239000001923 methylcellulose Substances 0.000 description 1
- 235000010981 methylcellulose Nutrition 0.000 description 1
- IUBSYMUCCVWXPE-UHFFFAOYSA-N metoprolol Chemical compound COCCC1=CC=C(OCC(O)CNC(C)C)C=C1 IUBSYMUCCVWXPE-UHFFFAOYSA-N 0.000 description 1
- 229960002237 metoprolol Drugs 0.000 description 1
- 229960004438 mibefradil Drugs 0.000 description 1
- 230000000813 microbial effect Effects 0.000 description 1
- 210000003657 middle cerebral artery Anatomy 0.000 description 1
- 150000007522 mineralic acids Chemical class 0.000 description 1
- 229960003632 minoxidil Drugs 0.000 description 1
- 230000006676 mitochondrial damage Effects 0.000 description 1
- 230000004065 mitochondrial dysfunction Effects 0.000 description 1
- 230000006540 mitochondrial respiration Effects 0.000 description 1
- 230000008811 mitochondrial respiratory chain Effects 0.000 description 1
- 238000002156 mixing Methods 0.000 description 1
- 230000036651 mood Effects 0.000 description 1
- 229960002608 moracizine Drugs 0.000 description 1
- FUBVWMNBEHXPSU-UHFFFAOYSA-N moricizine Chemical compound C12=CC(NC(=O)OCC)=CC=C2SC2=CC=CC=C2N1C(=O)CCN1CCOCC1 FUBVWMNBEHXPSU-UHFFFAOYSA-N 0.000 description 1
- 229960005181 morphine Drugs 0.000 description 1
- 102000051367 mu Opioid Receptors Human genes 0.000 description 1
- 230000010016 myocardial function Effects 0.000 description 1
- RNYMYKXFXYDCAS-UHFFFAOYSA-N n'-benzylpropanehydrazide Chemical class CCC(=O)NNCC1=CC=CC=C1 RNYMYKXFXYDCAS-UHFFFAOYSA-N 0.000 description 1
- KEXJLZMJVOTFOY-QEGDFHJFSA-N n,n-diethyl-4-[(s)-[(2s,5r)-4-[(3-fluorophenyl)methyl]-2,5-dimethylpiperazin-1-yl]-phenylmethyl]benzamide Chemical compound C1=CC(C(=O)N(CC)CC)=CC=C1[C@H](C=1C=CC=CC=1)N1[C@@H](C)CN(CC=2C=C(F)C=CC=2)[C@H](C)C1 KEXJLZMJVOTFOY-QEGDFHJFSA-N 0.000 description 1
- XARNMUQDYQFLNA-UHFFFAOYSA-N n-(diaminomethylidene)-3-methylsulfonyl-4-piperidin-1-ylbenzamide;hydrochloride Chemical compound Cl.CS(=O)(=O)C1=CC(C(=O)N=C(N)N)=CC=C1N1CCCCC1 XARNMUQDYQFLNA-UHFFFAOYSA-N 0.000 description 1
- SQDFHQJTAWCFIB-UHFFFAOYSA-N n-methylidenehydroxylamine Chemical compound ON=C SQDFHQJTAWCFIB-UHFFFAOYSA-N 0.000 description 1
- SQMWSBKSHWARHU-SDBHATRESA-N n6-cyclopentyladenosine Chemical compound O[C@@H]1[C@H](O)[C@@H](CO)O[C@H]1N1C2=NC=NC(NC3CCCC3)=C2N=C1 SQMWSBKSHWARHU-SDBHATRESA-N 0.000 description 1
- 229960002009 naproxen Drugs 0.000 description 1
- CMWTZPSULFXXJA-VIFPVBQESA-N naproxen Chemical compound C1=C([C@H](C)C(O)=O)C=CC2=CC(OC)=CC=C21 CMWTZPSULFXXJA-VIFPVBQESA-N 0.000 description 1
- 230000014508 negative regulation of coagulation Effects 0.000 description 1
- 229960000884 nelfinavir Drugs 0.000 description 1
- QAGYKUNXZHXKMR-HKWSIXNMSA-N nelfinavir Chemical compound CC1=C(O)C=CC=C1C(=O)N[C@H]([C@H](O)CN1[C@@H](C[C@@H]2CCCC[C@@H]2C1)C(=O)NC(C)(C)C)CSC1=CC=CC=C1 QAGYKUNXZHXKMR-HKWSIXNMSA-N 0.000 description 1
- 210000000944 nerve tissue Anatomy 0.000 description 1
- 230000010004 neural pathway Effects 0.000 description 1
- 230000000626 neurodegenerative effect Effects 0.000 description 1
- 230000016273 neuron death Effects 0.000 description 1
- 239000004090 neuroprotective agent Substances 0.000 description 1
- 239000002547 new drug Substances 0.000 description 1
- BOPGDPNILDQYTO-NNYOXOHSSA-N nicotinamide-adenine dinucleotide Chemical compound C1=CCC(C(=O)N)=CN1[C@H]1[C@H](O)[C@H](O)[C@@H](COP(O)(=O)OP(O)(=O)OC[C@@H]2[C@H]([C@@H](O)[C@@H](O2)N2C3=NC=NC(N)=C3N=C2)O)O1 BOPGDPNILDQYTO-NNYOXOHSSA-N 0.000 description 1
- 229960003512 nicotinic acid Drugs 0.000 description 1
- 235000001968 nicotinic acid Nutrition 0.000 description 1
- 239000011664 nicotinic acid Substances 0.000 description 1
- 229960000227 nisoldipine Drugs 0.000 description 1
- 229950008980 nitecapone Drugs 0.000 description 1
- 229960005425 nitrendipine Drugs 0.000 description 1
- 239000000041 non-steroidal anti-inflammatory agent Substances 0.000 description 1
- 229940021182 non-steroidal anti-inflammatory drug Drugs 0.000 description 1
- 239000012457 nonaqueous media Substances 0.000 description 1
- 239000002687 nonaqueous vehicle Substances 0.000 description 1
- 150000005830 nonesterified fatty acids Chemical class 0.000 description 1
- 239000002736 nonionic surfactant Substances 0.000 description 1
- 230000001777 nootropic effect Effects 0.000 description 1
- 230000001019 normoglycemic effect Effects 0.000 description 1
- 230000037000 normothermia Effects 0.000 description 1
- 239000002777 nucleoside Substances 0.000 description 1
- 150000003833 nucleoside derivatives Chemical class 0.000 description 1
- 239000002417 nutraceutical Substances 0.000 description 1
- 235000021436 nutraceutical agent Nutrition 0.000 description 1
- GYCKQBWUSACYIF-UHFFFAOYSA-N o-hydroxybenzoic acid ethyl ester Natural products CCOC(=O)C1=CC=CC=C1O GYCKQBWUSACYIF-UHFFFAOYSA-N 0.000 description 1
- ZQPPMHVWECSIRJ-KTKRTIGZSA-N oleic acid group Chemical group C(CCCCCCC\C=C/CCCCCCCC)(=O)O ZQPPMHVWECSIRJ-KTKRTIGZSA-N 0.000 description 1
- 239000003402 opiate agonist Substances 0.000 description 1
- 229960001027 opium Drugs 0.000 description 1
- 239000000082 organ preservation Substances 0.000 description 1
- 150000007524 organic acids Chemical class 0.000 description 1
- 235000005985 organic acids Nutrition 0.000 description 1
- DZOJBGLFWINFBF-UMSFTDKQSA-N osanetant Chemical compound C([C@](C1)(CCCN2CCC(CC2)(N(C(C)=O)C)C=2C=CC=CC=2)C=2C=C(Cl)C(Cl)=CC=2)CCN1C(=O)C1=CC=CC=C1 DZOJBGLFWINFBF-UMSFTDKQSA-N 0.000 description 1
- 230000000065 osmolyte Effects 0.000 description 1
- 230000008723 osmotic stress Effects 0.000 description 1
- 230000010627 oxidative phosphorylation Effects 0.000 description 1
- HXNFUBHNUDHIGC-UHFFFAOYSA-N oxypurinol Chemical compound O=C1NC(=O)N=C2NNC=C21 HXNFUBHNUDHIGC-UHFFFAOYSA-N 0.000 description 1
- IPCSVZSSVZVIGE-UHFFFAOYSA-N palmitic acid group Chemical group C(CCCCCCCCCCCCCCC)(=O)O IPCSVZSSVZVIGE-UHFFFAOYSA-N 0.000 description 1
- 238000007911 parenteral administration Methods 0.000 description 1
- 239000004031 partial agonist Substances 0.000 description 1
- 230000001991 pathophysiological effect Effects 0.000 description 1
- 230000007310 pathophysiology Effects 0.000 description 1
- 239000008188 pellet Substances 0.000 description 1
- 230000000149 penetrating effect Effects 0.000 description 1
- 230000035515 penetration Effects 0.000 description 1
- NQPDZGIKBAWPEJ-UHFFFAOYSA-N pentanoic acid group Chemical class C(CCCC)(=O)O NQPDZGIKBAWPEJ-UHFFFAOYSA-N 0.000 description 1
- WTWWXOGTJWMJHI-UHFFFAOYSA-N perflubron Chemical group FC(F)(F)C(F)(F)C(F)(F)C(F)(F)C(F)(F)C(F)(F)C(F)(F)C(F)(F)Br WTWWXOGTJWMJHI-UHFFFAOYSA-N 0.000 description 1
- 229960001217 perflubron Drugs 0.000 description 1
- 210000002640 perineum Anatomy 0.000 description 1
- 210000003200 peritoneal cavity Anatomy 0.000 description 1
- 230000037050 permeability transition Effects 0.000 description 1
- 230000002085 persistent effect Effects 0.000 description 1
- 239000000825 pharmaceutical preparation Substances 0.000 description 1
- 125000000951 phenoxy group Chemical group [H]C1=C([H])C([H])=C(O*)C([H])=C1[H] 0.000 description 1
- 229910052698 phosphorus Inorganic materials 0.000 description 1
- 230000001766 physiological effect Effects 0.000 description 1
- BCQTVJKBTWGHCX-UHFFFAOYSA-N pilsicainide Chemical compound CC1=CC=CC(C)=C1NC(=O)CC1(CCC2)N2CCC1 BCQTVJKBTWGHCX-UHFFFAOYSA-N 0.000 description 1
- 229950010769 pilsicainide Drugs 0.000 description 1
- 229960002310 pinacidil Drugs 0.000 description 1
- 239000004033 plastic Substances 0.000 description 1
- 229920003023 plastic Polymers 0.000 description 1
- 239000000106 platelet aggregation inhibitor Substances 0.000 description 1
- 229910052697 platinum Inorganic materials 0.000 description 1
- 229920000573 polyethylene Polymers 0.000 description 1
- 238000006116 polymerization reaction Methods 0.000 description 1
- 235000010482 polyoxyethylene sorbitan monooleate Nutrition 0.000 description 1
- 229920000053 polysorbate 80 Polymers 0.000 description 1
- 239000001267 polyvinylpyrrolidone Substances 0.000 description 1
- 235000013855 polyvinylpyrrolidone Nutrition 0.000 description 1
- 229920000036 polyvinylpyrrolidone Polymers 0.000 description 1
- 239000011148 porous material Substances 0.000 description 1
- 230000010411 postconditioning Effects 0.000 description 1
- 230000003389 potentiating effect Effects 0.000 description 1
- TUZYXOIXSAXUGO-PZAWKZKUSA-N pravastatin Chemical compound C1=C[C@H](C)[C@H](CC[C@@H](O)C[C@@H](O)CC(O)=O)[C@H]2[C@@H](OC(=O)[C@@H](C)CC)C[C@H](O)C=C21 TUZYXOIXSAXUGO-PZAWKZKUSA-N 0.000 description 1
- 229960002965 pravastatin Drugs 0.000 description 1
- IENZQIKPVFGBNW-UHFFFAOYSA-N prazosin Chemical compound N=1C(N)=C2C=C(OC)C(OC)=CC2=NC=1N(CC1)CCN1C(=O)C1=CC=CO1 IENZQIKPVFGBNW-UHFFFAOYSA-N 0.000 description 1
- 229960001289 prazosin Drugs 0.000 description 1
- 230000035935 pregnancy Effects 0.000 description 1
- 230000036316 preload Effects 0.000 description 1
- 230000002335 preservative effect Effects 0.000 description 1
- 238000002203 pretreatment Methods 0.000 description 1
- MVFGUOIZUNYYSO-UHFFFAOYSA-N prilocaine Chemical compound CCCNC(C)C(=O)NC1=CC=CC=C1C MVFGUOIZUNYYSO-UHFFFAOYSA-N 0.000 description 1
- 229960001807 prilocaine Drugs 0.000 description 1
- 229960005179 primaquine Drugs 0.000 description 1
- FYPMFJGVHOHGLL-UHFFFAOYSA-N probucol Chemical compound C=1C(C(C)(C)C)=C(O)C(C(C)(C)C)=CC=1SC(C)(C)SC1=CC(C(C)(C)C)=C(O)C(C(C)(C)C)=C1 FYPMFJGVHOHGLL-UHFFFAOYSA-N 0.000 description 1
- 229960003912 probucol Drugs 0.000 description 1
- MFDFERRIHVXMIY-UHFFFAOYSA-N procaine Chemical compound CCN(CC)CCOC(=O)C1=CC=C(N)C=C1 MFDFERRIHVXMIY-UHFFFAOYSA-N 0.000 description 1
- 229960004919 procaine Drugs 0.000 description 1
- 229940089949 procardia Drugs 0.000 description 1
- 238000012545 processing Methods 0.000 description 1
- 230000000750 progressive effect Effects 0.000 description 1
- JWHAUXFOSRPERK-UHFFFAOYSA-N propafenone Chemical compound CCCNCC(O)COC1=CC=CC=C1C(=O)CCC1=CC=CC=C1 JWHAUXFOSRPERK-UHFFFAOYSA-N 0.000 description 1
- 229960000203 propafenone Drugs 0.000 description 1
- 229960003712 propranolol Drugs 0.000 description 1
- 210000004129 prosencephalon Anatomy 0.000 description 1
- 150000003815 prostacyclins Chemical class 0.000 description 1
- 208000018299 prostration Diseases 0.000 description 1
- 239000003223 protective agent Substances 0.000 description 1
- 150000003834 purine nucleoside derivatives Chemical class 0.000 description 1
- ILVXOBCQQYKLDS-UHFFFAOYSA-N pyridine N-oxide Chemical compound [O-][N+]1=CC=CC=C1 ILVXOBCQQYKLDS-UHFFFAOYSA-N 0.000 description 1
- 238000000718 qrs complex Methods 0.000 description 1
- 229960001404 quinidine Drugs 0.000 description 1
- 108700016586 rat AIM Proteins 0.000 description 1
- 230000009257 reactivity Effects 0.000 description 1
- 230000036279 refractory period Effects 0.000 description 1
- 210000001567 regular cardiac muscle cell of ventricle Anatomy 0.000 description 1
- 230000004346 regulation of heart rate Effects 0.000 description 1
- 210000005000 reproductive tract Anatomy 0.000 description 1
- 238000011160 research Methods 0.000 description 1
- 230000036391 respiratory frequency Effects 0.000 description 1
- 230000003938 response to stress Effects 0.000 description 1
- 230000036390 resting membrane potential Effects 0.000 description 1
- 230000000717 retained effect Effects 0.000 description 1
- 229960003312 retigabine Drugs 0.000 description 1
- 206010039073 rheumatoid arthritis Diseases 0.000 description 1
- 239000002342 ribonucleoside Substances 0.000 description 1
- 229960004181 riluzole Drugs 0.000 description 1
- 230000000630 rising effect Effects 0.000 description 1
- 229960000311 ritonavir Drugs 0.000 description 1
- NCDNCNXCDXHOMX-XGKFQTDJSA-N ritonavir Chemical compound N([C@@H](C(C)C)C(=O)N[C@H](C[C@H](O)[C@H](CC=1C=CC=CC=1)NC(=O)OCC=1SC=NC=1)CC=1C=CC=CC=1)C(=O)N(C)CC1=CSC(C(C)C)=N1 NCDNCNXCDXHOMX-XGKFQTDJSA-N 0.000 description 1
- CVHZOJJKTDOEJC-UHFFFAOYSA-N saccharin Chemical compound C1=CC=C2C(=O)NS(=O)(=O)C2=C1 CVHZOJJKTDOEJC-UHFFFAOYSA-N 0.000 description 1
- 229940081974 saccharin Drugs 0.000 description 1
- 235000019204 saccharin Nutrition 0.000 description 1
- 239000000901 saccharin and its Na,K and Ca salt Substances 0.000 description 1
- 210000003752 saphenous vein Anatomy 0.000 description 1
- PGKXDIMONUAMFR-AREMUKBSSA-N saredutant Chemical compound C([C@H](CN(C)C(=O)C=1C=CC=CC=1)C=1C=C(Cl)C(Cl)=CC=1)CN(CC1)CCC1(NC(C)=O)C1=CC=CC=C1 PGKXDIMONUAMFR-AREMUKBSSA-N 0.000 description 1
- 230000002000 scavenging effect Effects 0.000 description 1
- 229910052711 selenium Inorganic materials 0.000 description 1
- 239000011669 selenium Substances 0.000 description 1
- 230000001953 sensory effect Effects 0.000 description 1
- 230000011664 signaling Effects 0.000 description 1
- 210000001013 sinoatrial node Anatomy 0.000 description 1
- 210000002027 skeletal muscle Anatomy 0.000 description 1
- 230000008326 skin blood flow Effects 0.000 description 1
- 230000008454 sleep-wake cycle Effects 0.000 description 1
- 210000002460 smooth muscle Anatomy 0.000 description 1
- 235000010413 sodium alginate Nutrition 0.000 description 1
- 239000000661 sodium alginate Substances 0.000 description 1
- 229940005550 sodium alginate Drugs 0.000 description 1
- 229910000030 sodium bicarbonate Inorganic materials 0.000 description 1
- 239000008354 sodium chloride injection Substances 0.000 description 1
- 239000000176 sodium gluconate Substances 0.000 description 1
- 235000012207 sodium gluconate Nutrition 0.000 description 1
- 229940005574 sodium gluconate Drugs 0.000 description 1
- 229910000162 sodium phosphate Inorganic materials 0.000 description 1
- 239000002689 soil Substances 0.000 description 1
- 210000001082 somatic cell Anatomy 0.000 description 1
- 230000000392 somatic effect Effects 0.000 description 1
- 239000001593 sorbitan monooleate Substances 0.000 description 1
- 235000011069 sorbitan monooleate Nutrition 0.000 description 1
- 229940035049 sorbitan monooleate Drugs 0.000 description 1
- 238000001228 spectrum Methods 0.000 description 1
- DUYSYHSSBDVJSM-KRWOKUGFSA-N sphingosine 1-phosphate Chemical compound CCCCCCCCCCCCC\C=C\[C@@H](O)[C@@H](N)COP(O)(O)=O DUYSYHSSBDVJSM-KRWOKUGFSA-N 0.000 description 1
- 239000002708 spider venom Substances 0.000 description 1
- 238000013319 spin trapping Methods 0.000 description 1
- 239000007921 spray Substances 0.000 description 1
- 238000005507 spraying Methods 0.000 description 1
- 230000007480 spreading Effects 0.000 description 1
- 238000003892 spreading Methods 0.000 description 1
- 230000037351 starvation Effects 0.000 description 1
- 230000003068 static effect Effects 0.000 description 1
- 238000007619 statistical method Methods 0.000 description 1
- 239000008174 sterile solution Substances 0.000 description 1
- 230000000638 stimulation Effects 0.000 description 1
- 239000011550 stock solution Substances 0.000 description 1
- 238000005728 strengthening Methods 0.000 description 1
- 210000003270 subclavian artery Anatomy 0.000 description 1
- 238000010254 subcutaneous injection Methods 0.000 description 1
- 208000011117 substance-related disease Diseases 0.000 description 1
- 238000011477 surgical intervention Methods 0.000 description 1
- 230000031068 symbiosis, encompassing mutualism through parasitism Effects 0.000 description 1
- 208000037905 systemic hypertension Diseases 0.000 description 1
- 230000028016 temperature homeostasis Effects 0.000 description 1
- 125000005329 tetralinyl group Chemical class C1(CCCC2=CC=CC=C12)* 0.000 description 1
- CFMYXEVWODSLAX-QOZOJKKESA-N tetrodotoxin Chemical compound O([C@@]([C@H]1O)(O)O[C@H]2[C@@]3(O)CO)[C@H]3[C@@H](O)[C@]11[C@H]2[C@@H](O)N=C(N)N1 CFMYXEVWODSLAX-QOZOJKKESA-N 0.000 description 1
- 229950010357 tetrodotoxin Drugs 0.000 description 1
- CFMYXEVWODSLAX-UHFFFAOYSA-N tetrodotoxin Natural products C12C(O)NC(=N)NC2(C2O)C(O)C3C(CO)(O)C1OC2(O)O3 CFMYXEVWODSLAX-UHFFFAOYSA-N 0.000 description 1
- 230000001732 thrombotic effect Effects 0.000 description 1
- 230000036962 time dependent Effects 0.000 description 1
- 230000000287 tissue oxygenation Effects 0.000 description 1
- 229960002872 tocainide Drugs 0.000 description 1
- 229930003799 tocopherol Natural products 0.000 description 1
- 239000011732 tocopherol Substances 0.000 description 1
- 125000002640 tocopherol group Chemical class 0.000 description 1
- 235000019149 tocopherols Nutrition 0.000 description 1
- 238000011200 topical administration Methods 0.000 description 1
- 229940041677 topical spray Drugs 0.000 description 1
- 230000001988 toxicity Effects 0.000 description 1
- 231100000419 toxicity Toxicity 0.000 description 1
- ZCIHMQAPACOQHT-ZGMPDRQDSA-N trans-isorenieratene Natural products CC(=C/C=C/C=C(C)/C=C/C=C(C)/C=C/c1c(C)ccc(C)c1C)C=CC=C(/C)C=Cc2c(C)ccc(C)c2C ZCIHMQAPACOQHT-ZGMPDRQDSA-N 0.000 description 1
- KBPHJBAIARWVSC-XQIHNALSSA-N trans-lutein Natural products CC(=C/C=C/C=C(C)/C=C/C=C(C)/C=C/C1=C(C)CC(O)CC1(C)C)C=CC=C(/C)C=CC2C(=CC(O)CC2(C)C)C KBPHJBAIARWVSC-XQIHNALSSA-N 0.000 description 1
- 230000009466 transformation Effects 0.000 description 1
- 238000000844 transformation Methods 0.000 description 1
- 230000005945 translocation Effects 0.000 description 1
- 229960001288 triamterene Drugs 0.000 description 1
- 125000002023 trifluoromethyl group Chemical group FC(F)(F)* 0.000 description 1
- 230000010024 tubular injury Effects 0.000 description 1
- 208000037978 tubular injury Diseases 0.000 description 1
- 210000005239 tubule Anatomy 0.000 description 1
- 230000006433 tumor necrosis factor production Effects 0.000 description 1
- 102000003298 tumor necrosis factor receptor Human genes 0.000 description 1
- 238000002604 ultrasonography Methods 0.000 description 1
- 210000000689 upper leg Anatomy 0.000 description 1
- 229940116269 uric acid Drugs 0.000 description 1
- 230000003191 uterotonic effect Effects 0.000 description 1
- 230000009677 vaginal delivery Effects 0.000 description 1
- 230000025033 vasoconstriction Effects 0.000 description 1
- 230000000982 vasogenic effect Effects 0.000 description 1
- 230000001457 vasomotor Effects 0.000 description 1
- 229960003726 vasopressin Drugs 0.000 description 1
- 238000009564 veno-arterial ECMO Methods 0.000 description 1
- 238000009423 ventilation Methods 0.000 description 1
- 230000035899 viability Effects 0.000 description 1
- 206010047470 viral myocarditis Diseases 0.000 description 1
- 230000003612 virological effect Effects 0.000 description 1
- 210000001835 viscera Anatomy 0.000 description 1
- 230000000007 visual effect Effects 0.000 description 1
- 235000019155 vitamin A Nutrition 0.000 description 1
- 239000011719 vitamin A Substances 0.000 description 1
- 235000019154 vitamin C Nutrition 0.000 description 1
- 239000011718 vitamin C Substances 0.000 description 1
- 229940045997 vitamin a Drugs 0.000 description 1
- 102000038650 voltage-gated calcium channel activity Human genes 0.000 description 1
- 108091023044 voltage-gated calcium channel activity Proteins 0.000 description 1
- 238000010792 warming Methods 0.000 description 1
- 229920003169 water-soluble polymer Polymers 0.000 description 1
- 239000002023 wood Substances 0.000 description 1
- FJHBOVDFOQMZRV-XQIHNALSSA-N xanthophyll Natural products CC(=C/C=C/C=C(C)/C=C/C=C(C)/C=C/C1=C(C)CC(O)CC1(C)C)C=CC=C(/C)C=CC2C=C(C)C(O)CC2(C)C FJHBOVDFOQMZRV-XQIHNALSSA-N 0.000 description 1
- 239000011701 zinc Substances 0.000 description 1
- 229910052725 zinc Inorganic materials 0.000 description 1
- 229950006967 zoxazolamine Drugs 0.000 description 1
- OENHQHLEOONYIE-JLTXGRSLSA-N β-Carotene Chemical compound CC=1CCCC(C)(C)C=1\C=C\C(\C)=C\C=C\C(\C)=C\C=C\C=C(/C)\C=C\C=C(/C)\C=C\C1=C(C)CCCC1(C)C OENHQHLEOONYIE-JLTXGRSLSA-N 0.000 description 1
- 108020001612 μ-opioid receptors Proteins 0.000 description 1
Classifications
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/70—Carbohydrates; Sugars; Derivatives thereof
- A61K31/7042—Compounds having saccharide radicals and heterocyclic rings
- A61K31/7052—Compounds having saccharide radicals and heterocyclic rings having nitrogen as a ring hetero atom, e.g. nucleosides, nucleotides
- A61K31/706—Compounds having saccharide radicals and heterocyclic rings having nitrogen as a ring hetero atom, e.g. nucleosides, nucleotides containing six-membered rings with nitrogen as a ring hetero atom
- A61K31/7064—Compounds having saccharide radicals and heterocyclic rings having nitrogen as a ring hetero atom, e.g. nucleosides, nucleotides containing six-membered rings with nitrogen as a ring hetero atom containing condensed or non-condensed pyrimidines
- A61K31/7076—Compounds having saccharide radicals and heterocyclic rings having nitrogen as a ring hetero atom, e.g. nucleosides, nucleotides containing six-membered rings with nitrogen as a ring hetero atom containing condensed or non-condensed pyrimidines containing purines, e.g. adenosine, adenylic acid
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/045—Hydroxy compounds, e.g. alcohols; Salts thereof, e.g. alcoholates
- A61K31/05—Phenols
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/16—Amides, e.g. hydroxamic acids
- A61K31/165—Amides, e.g. hydroxamic acids having aromatic rings, e.g. colchicine, atenolol, progabide
- A61K31/167—Amides, e.g. hydroxamic acids having aromatic rings, e.g. colchicine, atenolol, progabide having the nitrogen of a carboxamide group directly attached to the aromatic ring, e.g. lidocaine, paracetamol
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/185—Acids; Anhydrides, halides or salts thereof, e.g. sulfur acids, imidic, hydrazonic or hydroximic acids
- A61K31/19—Carboxylic acids, e.g. valproic acid
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/185—Acids; Anhydrides, halides or salts thereof, e.g. sulfur acids, imidic, hydrazonic or hydroximic acids
- A61K31/19—Carboxylic acids, e.g. valproic acid
- A61K31/194—Carboxylic acids, e.g. valproic acid having two or more carboxyl groups, e.g. succinic, maleic or phthalic acid
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/33—Heterocyclic compounds
- A61K31/395—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins
- A61K31/495—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins having six-membered rings with two or more nitrogen atoms as the only ring heteroatoms, e.g. piperazine or tetrazines
- A61K31/505—Pyrimidines; Hydrogenated pyrimidines, e.g. trimethoprim
- A61K31/519—Pyrimidines; Hydrogenated pyrimidines, e.g. trimethoprim ortho- or peri-condensed with heterocyclic rings
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/70—Carbohydrates; Sugars; Derivatives thereof
- A61K31/7004—Monosaccharides having only carbon, hydrogen and oxygen atoms
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K33/00—Medicinal preparations containing inorganic active ingredients
- A61K33/06—Aluminium, calcium or magnesium; Compounds thereof, e.g. clay
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K45/00—Medicinal preparations containing active ingredients not provided for in groups A61K31/00 - A61K41/00
- A61K45/06—Mixtures of active ingredients without chemical characterisation, e.g. antiphlogistics and cardiaca
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K47/00—Medicinal preparations characterised by the non-active ingredients used, e.g. carriers or inert additives; Targeting or modifying agents chemically bound to the active ingredient
- A61K47/06—Organic compounds, e.g. natural or synthetic hydrocarbons, polyolefins, mineral oil, petrolatum or ozokerite
- A61K47/26—Carbohydrates, e.g. sugar alcohols, amino sugars, nucleic acids, mono-, di- or oligo-saccharides; Derivatives thereof, e.g. polysorbates, sorbitan fatty acid esters or glycyrrhizin
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K9/00—Medicinal preparations characterised by special physical form
- A61K9/0012—Galenical forms characterised by the site of application
- A61K9/0019—Injectable compositions; Intramuscular, intravenous, arterial, subcutaneous administration; Compositions to be administered through the skin in an invasive manner
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K9/00—Medicinal preparations characterised by special physical form
- A61K9/08—Solutions
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P17/00—Drugs for dermatological disorders
- A61P17/02—Drugs for dermatological disorders for treating wounds, ulcers, burns, scars, keloids, or the like
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P23/00—Anaesthetics
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P23/00—Anaesthetics
- A61P23/02—Local anaesthetics
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P25/00—Drugs for disorders of the nervous system
- A61P25/04—Centrally acting analgesics, e.g. opioids
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P25/00—Drugs for disorders of the nervous system
- A61P25/20—Hypnotics; Sedatives
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P29/00—Non-central analgesic, antipyretic or antiinflammatory agents, e.g. antirheumatic agents; Non-steroidal antiinflammatory drugs [NSAID]
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P41/00—Drugs used in surgical methods, e.g. surgery adjuvants for preventing adhesion or for vitreum substitution
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P7/00—Drugs for disorders of the blood or the extracellular fluid
- A61P7/02—Antithrombotic agents; Anticoagulants; Platelet aggregation inhibitors
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P7/00—Drugs for disorders of the blood or the extracellular fluid
- A61P7/08—Plasma substitutes; Perfusion solutions; Dialytics or haemodialytics; Drugs for electrolytic or acid-base disorders, e.g. hypovolemic shock
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P9/00—Drugs for disorders of the cardiovascular system
- A61P9/06—Antiarrhythmics
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P9/00—Drugs for disorders of the cardiovascular system
- A61P9/10—Drugs for disorders of the cardiovascular system for treating ischaemic or atherosclerotic diseases, e.g. antianginal drugs, coronary vasodilators, drugs for myocardial infarction, retinopathy, cerebrovascula insufficiency, renal arteriosclerosis
Definitions
- a method for treating haemorrhage, shock and brain injury A method for treating haemorrhage, shock and brain injury
- the invention relates to a method of increasing blood pressure to an optimal level in a subject that has suffered a life threatening hypotension or shock.
- the invention also relates to a method of increasing blood pressure in a subject that is in a shocked state, particularly after circulatory collapse or infection or burn shock or disease.
- the methods of the invention relates to protecting the brain of a subject following injury.
- the invention also relates to a method for reducing the harmful effects of hypoperfusion in the whole body prior to further resuscitation or definitive care.
- the invention also includes a method for reducing the harmful effects brain injury without biood loss prior to definitive care.
- the present application claims priorit from Australian Provisonal Patent Application Nos. 2013902650, 2013902857, 2013902658, 2013902659 and 2013903844, the entire disclosures of which are incorporated into the present specification by this cross-reference.
- MAP mean arterial blood pressur
- TBI In addition to the adverse effects of hypotension, if TBI is associated with hemorrhagic, cardiogenic and septic shock, cardiac instability, CNS biorhythm disorders (heart rate variability), o coagulation, inflammatory imbalances the condition is worsened with increased mortality.
- hypertonic saline In some resuscitation therapies for brain protection have used hypertonic saline. Usually hypertonic saline has been used to reduce brain swelling. The literature suggests all hypertonic solutions from 3% to 23,5% NaCI have favourable effects when administered as either a bolus or continuous infusion (drip) and appear to be more effective than mannitol in reducing acute episodes of elevated intracranial pressure. However, it was shown in a pre-hospita! human trauma and hemorrhage shock trial that 7.5% NaCI hypertonic solutions led to a higher early-mortality rate compared with the group receiving 0,9% sodium chloride injection and the trial was halted. Another recent study assessed the effect of hypertonic resuscitation on outcome for patients with both hypotension and severe TBI.
- the present invention is directed toward overcoming or at least alleviating one or more of the difficulties of the prior art.
- the present invention provides a method of increasing blood pressure in a subject that has suffered a life threatening hypotensio or shock comprising the administration of (i) a compound selected from at least one of a potassium channel opener, a potassium channel agonist and an adenosine receptor agonist; and (ii) an antiarrhythmic agent or a local anaesthetic to the subject.
- a compound selected from at least one of a potassium channel opener, a potassium channel agonist and an adenosine receptor agonist e.g., a compound selected from at least one of a potassium channel opener, a potassium channel agonist and an adenosine receptor agonist
- an antiarrhythmic agent or a local anaesthetic e.g., a compound selected from at least one of a potassium channel opener, a potassium channel agonist and an adenosine receptor agonist
- an antiarrhythmic agent or a local anaesthetic e.g., a local anaesthetic to
- the method 7 includes administration of an elevated source of magnesium ions.
- the method may also include the administration of an anti-inflammatory agent and/or metabolic fuel
- the present invention is also directed to use of (i) a compound selected from at least one of a potassium channel opener, a potassium channel agonist and an adenosine receptor agonist; and (ii) an antiarrhythmic agent or a local anaesthetic in the manufacture of a medicament for increasing blood pressure in a subject that has suffered a life threatening hypotension or shock.
- the present invention is also directed to use of (i) a compound selected from at least one of a potassium channel opener, a potassium channel agonist and an adenosine receptor agonist; and (ii) an antiarrhythmic agent or a local anaesthetic for increasing blood pressure in a subject that has suffered a life threatening hypotension or shock.
- the present invention is also directed to (i) a compound selected from at least one of a potassium channel opener, a potassium channel agonist and an adenosine receptor agonist; and (ii) an antiarrhythmic agent or a local anaesthetic for use in increasing blood pressure in a subject that has suffered a life threatening hypotension or shock.
- the composition is administered by bolus followed by iv drip.
- the anti-inflammatory agent is BOH.
- the metabolic fuel is citrate.
- the antiarrhythmic agent is lidocaine.
- the potassium channel opener or agonist and/or adenosine receptor agonist is adenosine.
- the present invention aiso provides a composition which may be used in increasing blood pressure in a subject that has suffered a life threatening hypotension or shock comprising (i) a compound selected from at least one of a potassium channel opener, a potassium channel agonist and an adenosine receptor agonist; and (ii) an antiarrhythmic agent or a iocal anaesthetic.
- a compound selected from at least one of a potassium channel opener, a potassium channel agonist and an adenosine receptor agonist; and (ii) an antiarrhythmic agent or a iocal anaesthetic Preferably the composition includes an elevated source of magnesium ions.
- the composition may also include or be administered with an anti- inflammatory agent and/or metabolic fuel.
- the present invention is directed to a method of inducing a low pain or analgesic state in a subject that has suffered a life threatening hypotension or shock comprising the administration of (i) a potassium channel opener or agonist and/or adenosine receptor agonist; (ii) an antiarrhythmic agent or a Iocal anaesthetic; and (in) an elevated source of magnesium ions to the subject.
- the composition may also include or be administered with an anti-inflammatory agent and/or metabolic fuel.
- the present invention is directed to a method of inducing hypotensive anaesthesia in a subject that has suffered a life threatening hypotension or shock comprising the administration of (i) a potassium channel opener or agonist and/or adenosine receptor agonist; (ii) an antiarrhythmic agent or a local anaesthetic; and (iii) an elevated source of magnesium ions to the subject.
- the composition may also include or be administered with an a nti- inflammatory agent and/or metabolic fuel.
- the present invention is directed to a method for reducing hypofusion in the whole body of a subject, particularly prior to further resuscitation or definitive care comprising the administration of (i) a compound selected from at least one of a potassium channel opener, a potassium channel agonist and an adenosine receptor agonist; and (ii) an antiarrhythmic agent or a local anaesthetic to the subject.
- a compound selected from at least one of a potassium channel opener, a potassium channel agonist and an adenosine receptor agonist; and (ii) an antiarrhythmic agent or a local anaesthetic to the subject.
- the method also includes administration of an elevated source of magnesium ions.
- the method may also include the administration of an antiinflammatory agent and or metabolic fuel
- the present invention is also directed to use of (i) a compound selected from at least one of a potassium channel opener, a potassium channel agonist and an adenosine receptor agonist; and (ii) an antiarrhythmic agent or a local anaesthetic in the manufacture of a medicament for inducing a low pain or analgesic state or hypotensive anaesthesia or reducing hypofusion in the whole bod of a subject that has suffered a life threatening hypotension or shock.
- the present invention is also directed to (i) a compound selected from at least one of a potassium channel opener, a potassium channel agonist and an adenosin receptor agonist; and (ii) an antiarrhythmic agent or a local anaesthetic for use in inducing a low pain or analgesic state or hypotensive anaesthesia or reducing hypofusion in the whole body of a subject that has suffered a life threatening hypotension or shock.
- the present invention is also directed to use of (i) a compound selected from at least one of a potassium channel opener, a potassium channel agonist and an adenosine receptor agonist; and (ii) an antiarrhythmic agent or a local anaesthetic for inducing a low pain or analgesic state o hypotensive anaesthesia or reducing hypofusion in the whole body in a subject that has suffered a life threatening hypotension or shock.
- the present invention also provides a composition which may be used in inducing a low pain or analgesic state or hypotensive anaesthesia or for reducing hypofusion in the whole body of a subject that has suffered a life threatening hypotension or shock comprising (i) a compound selected from at least one of a potassium channel opener, a potassium channel agonist and an adenosine receptor agonist; and (ii) an antiarrhythmic agent or a local anaesthetic.
- the method also includes administration of an elevated source of magnesium tons.
- the method may also include the administration of an anti-inflammatory agent and/or metabolic fuel.
- compositions described above further comprise a pharmaceutically acceptable carrier.
- the composition is a pharmaceutical composition.
- the composition may be in the form of a kit in which components (i) and (ii) are held separately.
- the kit may be adapted to ensure simultaneous, sequential or separate administration of components (i) and (ii) when used in the methods described above.
- the invention relates to methods of increasing blood pressure to an optimal level in a subject that has suffered a life threatening hypotension or shock.
- the invention also relates to compositions for use in these methods and pharmaceutical preparations suitable for such treatments.
- the present invention provides a method of increasing blood pressure in a subject that has suffered a life threatening hypotension or shock comprising the administration of (i) a compound selected from at least one of a potassium channel opener, a potassium channel agonist and an adenosine receptor agonist; and (ii) an antiarrhythmic agent or a local anaesthetic.
- a compound selected from at least one of a potassium channel opener, a potassium channel agonist and an adenosine receptor agonist; and (ii) an antiarrhythmic agent or a local anaesthetic Preferably the method also includes administration of an elevated source of magnesium tons.
- the method may also include the administration of an anti-inflammatory agent and/or metabolic fuel.
- composition or composition useful in methods according to the invention, although there are a number of combinations of components embodying the invention which are compositions useful in the invention.
- the composition is administered in two stages. First by bolus followed by iv drip.
- the present invention with the a bolus and dri therap is designed to treat uncontrolled hemorrhage (life threatening hypotension) in patients with or without suspected TBI, and along with its whole body protection properties would also be applicable for widespread potential medical preparedness efforts and capabilities in mass casualty situations such as train accidents, plane crashes, natural disasters or from terrorist attacks.
- the new resuscitation fluid has the potential to fill a major capability gap for military and public purpose.
- Ischemic cerebrovascular disease without blood loss is also a leading cause of mortality and the major cause of chronic disability in the adult population in the western world today.
- Ischemic heart disease (which includes myocardial infarction, angina pectoris and heart failure when preceded by myocardial infarction) also can all occur without blood loss is the leading cause death worldwide.
- the present invention with a bolus and drip therapy can also be used for inj ry states without blood loss.
- the invention can treat any serious injury of a traumatic or non-traumatic origin that results in a life threatening shocked state that affects normal brain and whole body function. Conversely, it can treat the shocked state that is the result of brain injury or neural disease.
- the invention can treat both the shocked state, the brain and the whole body. In addition the invention can treat brain injury without hemorrhage or blood loss.
- hypothermia is believed to be protective for the body, particularly the brain, and is used commonly in major surgery and coma-tike states. Although the mode, timing and rate of cooling and rewarming remain controversial, mild therapeutic hypothermia has shown to beneficial but deep hypothermia may in some critically til states be preferred, and extreme below 10°C may be life-saving in other extreme forms of near-death or death.
- a proposed mechanism of the invention includes a whole body improvement of circulation, improved local and CMS control of blood pressure, improved inflammatory and coagulation states and improved tissue oxygenation with multi-organ protection including the brain. Since the medulla in the brainstem is responsible for breathing, heart rate, blood pressure, arrhythmias and the sleep-wake cycle, part of the mechanism may reside in the composition's action in this region of the brain. The specific area may be the nucleus tractus solitaris (NTS), which is the first nucleus in the medulla that receives and integrates sensory information from cardiovascular and pulmonary signals in the body.
- NTS nucleus tractus solitaris
- the NTS receives afferent projections from the arterial baroreceptors, carotid chemoreceptors, volume receptors and cardiopulmonary receptors for processing and makes autonomic adjustments along with higher orders of the brain to maintain arteria! biood pressure within a narrow range of variation.
- cardiovascular and pulmonary systems are primarily controlled by the brainstem, other 'higher' areas in the central autonomic network (e.g. in the forebrain) are known to be involved, and the invention is not limited to the brain stem but also to these higher control centers.
- This central autonomic network consists of three hierarchically ordered circuits or loops: 1) the short-term brainstem-spinal loops, 2 ⁇ the limbic brain-hypotha!amic-brainstem-spinal cord loops mediating anticipatory and stress responses, and 3) the intermediate length hypothalamic-brainstem-spinal cord loops mediating longer-term autonomic reflexes (e.g. involved in temperature regulation).
- the paraventricular nucleus (PVN) is one of the most important hypothalamic nucleus of the central autonomic network.
- the PVN comprises approximately 21,500 neurones is the "autonomic master controller" and a critical regulator of numerous endocrine and autonomic functions.
- Regulation of body temperature is also under hypothalamic control of brainstem and spinal autonomic nuclei related to longer-term autonomic reflexes.
- Activation of sympathetic nervous system is involved in the increase of heat generation and decrease of heat loss: control of thermoregulation muscle tone, shivering, skin blood flow and sweating may b affected.
- the parvocellufar neurons of the PVN are known to be involved in the control of central autonomic outflow. Cholinergic activation of PVN decreases bod temperature and cholinergic activation of SON increases body temperature.
- heart rate variability Another aspect of the mechanism underpinning the invention is improved heart rate variability, which also indicates CNS protection and improved balance of electrical homeostasis. Improvement of heart rate variability during resuscitation from shock also supports the concept of improved CNS function. However, local control of the heart function and blood pressure cannot be ruled out. Acute brain injury results in decreased heart beat oscillations and baroreflex sensitivity indicative of uncoupling of the autonomic and cardiovascular systems. Brain vagal and sympathetic cardiac influences operate on the heart rate in different frequenc bands. While vagal regulation has a relatively high cut-off frequency, modulating heart rate both at low and high frequencies, up to 1.0 Hz, sympathetic cardiac control operates onl 0.15 Hz.
- heart rate variability The clinical relevance of the information on autonomic cardiac control provided by heart rate variability parameters is supported by the evidence that reduced heart rate variability and baroreflex control of heart rate is associated with increased mortality after myocardial infarction as well as in heart failure patients, and with increased risk of sudden arrhythmic death.
- the invention may act to bring balance to these intricate interactions between the periphery and brain and restore homeostasis.
- NO nitric oxide
- glutamate in the brainstem nuclei are involved in centra! cardiovascular regulation, Activation of the NO system in the lower brainstem modulates a variety of neuronal pathways; NO was shown to induce GABA. and g!utamate releases within the medulla.
- NO is involved in the modulation of the baroreflex within the nucleus tractus sQlitarius (NTS) and can be activated in the brain is activated in the states of homeostatic imbalances, including hypertension and stress. Further NO has been linked to vagal afferent input to th NTS in the medulla oblongat, which may help regulate inflammation and therefore coagulation.
- compositions, methods of treatment, and methods of manufacturing a medicament for treatment involving a composition which comprises (i) a compound selected from at least one of a potassium channel opener, a potassium channel agonist and an adenosine receptor agonist; and (ii) antiarrhythmic agent or a local anaesthetic.
- a composition which comprises (i) a compound selected from at least one of a potassium channel opener, a potassium channel agonist and an adenosine receptor agonist; and (ii) antiarrhythmic agent or a local anaesthetic.
- the composition includes an elevated source of magnesium ions.
- the composition ma also include or be administered with an anti-inflammatory agent and/or metabolic fuel
- Traumatic Brain injury is defined as damage to the brain resulting from an external physical or mechanical force, such as that caused by rapid acceleration or deceleration, blast waves, crush, an impact or penetration by a projectiie. It can lead to temporary or permanent impairment of cognitive, physical and psychosocial function.
- damage to nerve tissue is usually focused in one or more areas of the brain at first, although tearing can result in diffuse injury.
- Non-traumatic Brain injury is any injury to the brain that does not result from any cause that does not injure the brain using physical force, but rather occurs via infection, poisoning, tumor, or degenerative disease.
- Causes include Sack of oxygen, glucose, or blood are considered non-traumatic.
- Infections can cause encephalitis (brain swelling), meningitis (meningeal swelling), or cell toxicity, as can tumors or poisons.
- These infections can occur through stroke, heart attack, near-drowning, strangulation or a diabetic coma, poisoning or other chemical causes such as alcohol abuse or drug overdose, infections or tumors and degenerative conditions such as Alzheimer's disease and Parkinson's disease.
- Non-traumatic injury, damage is usually spread throughout the brain and exceptions include tumors and an infection that may remain localised or spreads evenly from one starting point.
- Traumatic Event is cell, tissue, organ or whole body damage that can occur from a traumatic or non-traumatic event.
- Injury may appear as the primary injury from the initial traumatic event, and secondary injury which is a time- dependent process progressing from the primary event and may include, but not limited to. injuries from infection, ischemic injury, reperfusion injury with an inflammatory, coagulation and central nervous system regulatory dysfunction.
- primary injuries ⁇ wounds and burns) for war are distinct from peacetime traumatic injuries because these higher velocity projectiles arid/or blast devices cause a more severe injury and accompanying wounds are frequently contaminated by clothing, soil, and environmental debris.
- the secondary injuries share many similarities to the civilian setting with the exception of long evacuation times where complications can arise.
- Injuries can also occur from a primary non-traumatic (not from a physical or mechanical force) and includes damage resulting from infection, poisoning, tumor, or degenerative disease. Lack of oxygen, glucose, or blood can be considered non-traumatic arising from these causes. Infections can cause encephalitis (brain swelling), meningitis (meningeal swelling), or cell toxicity, as can tumors or poisons. These infections can occur through stroke, heart attack, near- drowning, strangulation or a diabetic coma, poisoning or other chemical causes such as alcohol abuse or drug overdose, infections or tumors and degenerative conditions such as Alzheimer's disease and Parkinson's disease.
- Haemorrhage Bleeding from a break in the wall of one or more blood vessels from an injury or trauma, and it will continue as long as the vessel remains open and the pressure inside the vessel exceeds that pressure on the outside of the vessel waif.
- Non-Compressible Hemorrhage Hemorrhage that cannot be stopped with direct compression. Over 80% of hemorrhagic deaths on the battlefield are attributed to non-compressible interna! hemorrhage that is not accessible to a tourniquet or direct compression. Non-compressible torso hemorrhage is the ieading cause of potentially survivable trauma in the battlefield. Most deaths occur in first hour
- Uncontrolled Hemorrhage Same as non-compressible bleeding from one or more blood vessels that cannot be controlled.
- Hypertonic saline is defined as a saline concentration greater than normal isotonic saline which is 0.9% NaC! (0.1 ⁇ 4 ),
- Shock is defined as a severe hypotensive state when the arterial blood pressure is too low to maintain an adequate supply of blood and oxygen to the body's cells, organs and tissues. Shock is the result of "circulatory collapse" which can be causes from many interna! and external sources, it can be caused by a heart attack or heart failure, stroke, cardiac arrest from heart or a respiratory origin (choking, drowning, hanging), internal or external bleeding (hypovolemic shock), infection (septie shock), dehydration, severe burns (burn shock), or severe vomiting and/or diarrhea, all of which involve the loss of large amounts of bodily fluids. Shock can be caused by severe allergic reaction or injury (traumatic or non-traumatic) such as brain injury and bleeding.
- Systolic arterial blood pressure is the maximum amount of work or force exerted on the arterial wal! by the blood (usually measured by a sphygmomanometer) during the contraction of the left ventricle of the heart.
- Systolic pressure is the highest reading of blood pressure measurement (systolic/diastolic)>
- a palpable pulse refers to feeling the highest or systolic pressure at various arterial locations in the body (radial, carotid, femoral) (Lamia et a!., 2005).
- Diastolic arterial blood pressure is the minimum amount of work or force exerted by the blood on the arterial wall as the heart relaxes, it is the lower number of the blood pressure reading (systolic/diastoiic).
- MAP Mean Arterial Pressure
- Normotensive Resuscitation Conventional treatment of the shocked trauma patient involves intravenous fluid administration to bring the blood pressure back to "normal".
- the rational for normotensive resuscitation has been to maintain tissue perfusion and vital organ function while diagnostic and therapeutic procedures are being performed.
- 3 L of crystalloid has been recommended if complete fluid resuscitation is to be achieved. This method is controversial because it produces inflammatory and coagulopathy disturbances.
- the choic of resuscitation fluid to produce optimal outcome is aiso highly controversial
- Hypotensive resuscitation in the trauma setting is defined as a small volume of fluid(s) to resuscitate a patient's MAP from a shocked state (MAP ⁇ 40 mmHg) to a higher value to support life until any active bleeding is controlled.
- Hypotensive refers to a range of pressures below the normal arterial biood pressure (130/80), Hypotensive resuscitation is different from “permissive" hypotensive resuscitation because it encompasses a wider pressure range of low-pressure resuscitation.
- the term "permissive" refers to the return of a palpable pulse.
- Permissive hypotensive resuscitation is defined as a small volume of f!uid(s) to resuscitate a patient's MAP from a shocked state (MAP 40 mmHg) to a systoiic biood pressure of 60 to 80 mmHg required to establish a radial pulse.
- ATD Advanced Trauma Life Support
- SBP systolic blood pressure
- hypotensive anaesthesia is the controlled regulation of mean arterial pressures (MAP) that reduces biood loss during surgery or c!inicai interventions. Studies have shown that if MAP is reduced to 50 mmHg during surgery or intervention t e Wood loss can reduce by over 50%, which may reduce the need for fluid or blood products. The reduced blood loss also limits dilution and consumption of coagulation factors and subsequent postoperative rebound hypercoagulability. If MAP is maintained at 60 mmHg rather than 50 mmHg, bfood loss is about 40% greater. Hypotensive anaesthesia can be induced using either general or regional anaesthesia and enhanced using vasodilators to improve cardiac output.
- MAP mean arterial pressures
- Therapeutic Hypothermia or "targeted hypothermia” is the active "controlled” cooling of a ceil, organ or whole body to reduce injury. It has clinicai applications for arrest, protection and preservation of the brain and heart during cardiac surgery, and has shown to be useful after cardiac arrest or treating an unconscious or coma patient in the out-of-hospital environment. The rate and degree of cooling and targeted body temperature is controversial. Deep Hypothermic Circulatory Arrest (DHCA) or hypothermic cardiac standstill is a surgical technique that involves cooling the body of the patient and stopping blood circulation, ivliid hypothermia is a core body temperature of 33 to 36 C. moderate is 28 to 32 C. severe is 25 to 28 and deep hypothermia is 20 to 25°C or below. Extreme therapeutic hypothermia would be below 10°C.
- DHCA Deep Hypothermic Circulatory Arrest
- ivliid hypothermia is a core body temperature of 33 to 36 C. moderate is 28 to 32 C. severe is 25 to 28 and deep hypotherm
- Trauma can be broadly characterised as reversible and irreversible cell injury.
- reversible cell injury can lead to heart dysfunction usually from arrhythmias and/or stunning.
- Stunning is normally characterised as loss of left pum function during restoration of blood flow following periods of ischemia. If severe, it can lead to the death of the heart, usually from arrhythmias, even though the heart cells themselves are not initially dead.
- Irreversible injury by definition arises from actual cell death which may be fatal depending upon the extent of the injury. The amount of cell death can be measured as infarct size.
- the heart can be restored substantially to normal function of the tissue by reperfusion, with minimal infarct size.
- the syndromic illness resulting from a characteristic relatively minor sting, develops after about 30 minutes.
- the mechanisms of actions of their toxins appear to include modulation of neuronal sodium channels leading to massive release of endogenous catecholamine (C. barnesi, A. mordens and M, maxima) and possibly stress-induced cardiomyopathy.
- endogenous catecholamine C. barnesi, A. mordens and M, maxima
- systemic hypertension and myocardial dysfunction are associated with membrane leakage of troponin indicating heart ceil death.
- Clinical management includes parenteral analgesia, antihypertensive therapy, oxygen and mechanical ventilation. The present invention may alleviate some of these symptoms.
- Brain injury without blood loss includes traumatic brain injury and stroke.
- the goal of therapy in patients with severe head injury is to avoid secondary brain damage including reducing brain swelling.
- Hemmorhagic shock Traumatic brain injury (TBI) from injury and trauma is often complicated by hemorrhagic shock (HS) and visa versa. Combination of TBI and HS is highly lethal, and the optimal resuscitation strategy for this combined insult remains unclear. Most studies of HS after experimental TBI have focused on intracranial pressure; few have explored the effect of HS on neuronal death after TBI. Valproic acid (VPA), a histone deacetylase inhibitor, can improve survival after hemorrhagic shock (HS), protect neurons from hypoxia- induced apoptosis, and attenuate the inflammatory response.
- VPA histone deacetylase inhibitor
- Sepsis and septic shock Sepsis affects the brain, and the impairment of brain function resulting from sepsis is often associated with severe infectious disease.
- the effects of sepsis on the brain are detectable in previously healthy brains but are amplified in cases with concomitant brain injury, as after traumatic brain injury or subarachnoid haemorrhage. Previous injuries, in fact, increase brain vulnerability to the complex cascade of events summarized in the term "septic encephalopathy". Brain and sepsis remains a difficult and relatively unexplored topic with no treatments.
- Cardiogenic Shock occurs in 5% to 8% of patients hospitalized with ST- elevation myocardial infarction.
- CS is a state of end-organ hypoperfusion including brain damage due to cardiac failure.
- the definition of CS includes hemodynamic parameters: persistent hypotension (systolic blood pressure ⁇ 80 to 90 mm Hg or mean arterial pressure 30 mm Hg lower than baseline) with severe reduction in cardiac index and adequate or elevated filling pressure or right ventricular [RV] end-diastoltc pressure >10 to 15 mm Hg.
- Mortality can range from 10% to SG% depending on demographic, clinical, and hemodynamic factors. These factors include age, clinical signs of peripheral hypoperfusion and anoxic brain damage.
- Obstructive Shock is due to obstruction of blood flow outside of the heart.
- Pulmonary embolism and cardiac tamponade are examples of obstructive shock. Similar to cardiogenic shock.
- Vasogenic Shock is shock resulting from peripheral vascular dilation produced by factors such as toxins that directly affect the blood pressure to fall; and includ anaphylactic shock (allergic reaction) and septic shock (bacterial, viral or fungal).
- Neurogenic shock is a hypotension that is attributed to the disruption of the autonomic pathways within the spinal cord. Hypotension can lead to brain injury or result from brain, spinal cord or cervical injury,
- Burn Shock is defined as tissue damage caused by a variety of agents, such as heat, chemicals, electricity, sunlight, or nuclear radiation.
- the injury a 3-dimensional mass of damaged tissue and can produce massive inflammatory response and coagulopathy and can lead to shock and organ failure including brain damage.
- Diabetic Shock Diabetic coma is a reversible form of coma found in people with diabetes mellitus.
- Maintaining normog!ycemia of a casualty is of great importance during an medical treatment to reduce mortality and improve outcome whether on the battlefield, evacuation or in the prehospital, surgical and medical intensive care unit.
- Normally glucose is the primary fuel for the brain but in the critically ill from injury, infection, trauma and disease, glucose uptake and metabolism can be impaired.
- Hyperglycemia aggravates underlying brain damage and influences both morbidity and mortality in critically ill patients by inducing tissue acidosis oxidative stress, and cellular immunosuppression, which, in turn, promote the development of multiorgan failure.
- Hypoglycemia impairs energy supply causing metabolic perturbation and inducing cortical spreading depolarizations.
- both hyperglycemia and hypoglycemia need to be avoided to prevent aggravation of underlying brain damage.
- Both hyper- and hypoglycemia have been associated with poor outcome in traumatic brain injury (TBI).
- Stress insulin resistance high blood glucose
- the present invention with alternative fuels for metabolism in life threatening situations or in the critical ill such a diabetes may reduce tissue acidosis oxidative stress, and cellular immunosuppression.
- Alternative energy sources that can bypass glucose as a fuel include ketones (acetone or acetoacetate) or carboxylic acids (D-beta-hydroxybutryate).
- ketones acetone or acetoacetate
- carboxylic acids D-beta-hydroxybutryate
- Natural hibernating animals produce ketones (and carboxylic acids) during hibernation to repienish the energy currency of the cell (adenosine-S'-triphosphatei ATP) and humans do the same during starvation.
- D-beta-hydroxybutryate was reported to suppress lactic acidemia and hyperglycemia via alleviation of glycolysis during hemorrhagic shock in rats.
- D-beta-hydroxybutryate is converted to acetyl-GoA through pathways separate than glycolysis before entering the the Krebs Cycle and preferential utilization of D- beta-hydroxybutr ate rather than glucose as an energy substrate might reduce the deleterious accumulation of rising glucose or maintain a normoglycemic state.
- Ketones have been successfully applied to both rapldfy developing pathologies (seizures, giutamate excitotoxicity, hypoxia/ischemia) and neurodegenerative conditions (Parkinson's disease, Alzheimer's disease) and more recently TBI.
- the brain's ability to increase its reliance on ketone bodies appears to be a form of cerebral metabolic adaptation. Cerebral shifting to ketone metabolism requires (1) increasing the availability of ketones, (2) increasing cerebral uptake of ketones, and (3) potentially increasing the activity of the necessary enzymes for ketone metabolism.
- Acetyl CoA the main substrate that fuels the Krebs cycle to replenish ATP in the cell's powerhouse, the mitochondria.
- Acetyl CoA comes from glucose metaboiism (glycolysis) however Acetyl CoA can alternatively come from other pathways such as ketone metabolism, which forms acetyl CoA primes the cycle by forming citrate. Citrate administration may also bypass glucose requirement during insulin resistance and improve outcome.
- Ketones and citrate have the advantage of not needing insulin to enter the cell and generate ATP in the mitochondria, and thus ma replenish the Krebs cycle if acetyl CoA is limiting or when Krebs cycle intermediates are limiting as a result of sepsis. Citrate can also act by lowering the cellular burden of non-esterified fatty acids that have been implicated in mitochondrial dysfunction during sepsis.
- Another aspect of the invention is to improve neuroautonomic regulation of heart rate and blood pressure oscillations by reducing dangerous oscillations in the body's normal biorhythms such as in heart rate and blood pressure which implies improved whole boyd and brain function.
- HR variability, infection, inflammation and coagulation outside the brain may improve brain function including postoperative cognitive decline.
- Postoperative delirium are a major cause of morbidity associated with surgery.
- POCD occurs in 7-26% of patients undergoing surgery. The possibility exists that elevations of TNF in the periphery lead to cognitive decline.
- Efferent nerve connections from the vagal nerve to the spleen can be modulated to block experimental septic shock and autoimmune immune models of rheumatoid arthritis.
- Im roves brain swelling and intra-cranial pressure Another aspect of the invention may be to reduce on brain swelling, reduce intracranial pressure, improve biood flow to the brain, reduce brain inflammation, brain coagulopathy and secondary injury in the brain, and the benefit this has in the body's circulation and multiple organ function.
- the invention improves "Integration" on how nervous system can perform high level functions to improve whole body function.
- ECMO venoarterial extracorporeal membrane oxygenation
- ECMO can provide partial or total support, is temporary (days to weeks but in children following heart surgery may be months), and requires systemic anticoagulation.
- ECMO controls gas exchange and perfusion, stabilizes the patient physiologically, decreases the risk of ongoing iatrogenic injury, and allows ample time for diagnosis, treatment, and recovery from the primary injury or disease.
- ECMO is used in a variety of clinical circumstances and the results depend on the primary indication.
- ECMO provides life support but is not a form of treatment (Bartlett and Gattinoni, 2010 ).
- Our invention could be used to rescue the critically ill or wounded prior to ECMO as a treatment and continued after ECMO has been connected for stabilization. A similar case would occur with cardiopulmonary bypass.
- tissue is used herein in its broadest sense and refers to any part of the body exercising a specific function including organs and cells or parts thereof, for example, ceil lines or organelle preparations.
- Other examples include conduit vessels such as arteries or veins or circulatory organs such as the heart, respiratory organs such as the lungs, urinary organs such as the kidneys or bladder, digestive organs such as the stomach, liver, pancreas o spleen, reproductive organs such as the scrotum, testis, ovaries or uterus, neurological organs such as the brain, germ cells such as spermatozoa or ovum and somatic ceils such as skin cells, heart cells (ie, myocytes), nerve ceils, brain ceils or kidney cefis.
- conduit vessels such as arteries or veins or circulatory organs such as the heart, respiratory organs such as the lungs, urinary organs such as the kidneys or bladder, digestive organs such as the stomach, liver, pancreas o spleen, reproductive organ
- Organ The term "organ” is used herein in its broadest sense and refers to any part of the body exercising a specific function including tissues and cells or parts thereof, for example, endothelium, epithelium, blood brain barrier, cell lines or organelle preparations.
- circulatory organs such as the blood vessels, heart, respiratory organs such as the lungs, urinary organs such as the kidneys or bladder, digestive organs such as the stomach, liver, pancreas or spleen, reproductive organs such as the scrotum, testis, ovaries or uterus, neurological organs such as the brain, germ cells such as spermatozoa or ovum and somatic cells such as skin cells, heart cells i.e., myocytes, nerve ceils, brain cells or kidney cells.
- the subject may be a human or an animal such as a livestock animal (eg, sheep, cow or horse), laboratory test animal (eg, mouse, rabbit or guinea pig) or a companion animal (eg, dog or cat), particularly an animal of economic importance.
- a livestock animal eg, sheep, cow or horse
- laboratory test animal eg, mouse, rabbit or guinea pig
- a companion animal eg, dog or cat
- the subject is human.
- Body The body is the body of a subject defined above.
- composition The term “pharmaceutical composition” as used in this specification also includes “veterinary composition”.
- the term derivative refers to variations in the structure of compounds.
- the derivatives are preferably "pharmaceutically acceptable derivative” which includes any pharmaceutically acceptable salt, hydrate, ester, ether, amide, active metabolite, analogue, residue or any other compound which is not biologically or otherwise undesirable and induces the desired pharmacological and/or physiological effect.
- Salts Salts of the compounds are preferably pharmaceutically acceptable, but it will be appreciated thai non-pharmaceutically acceptable salts also fall within the scope of the specification, since these are usefui as intermediates in the preparation of pharmaceutically acceptable salts.
- Examples of pharmaceutically acceptable salts include salts of pharmaceutically acceptable cations such as sodium, potassium, lithium, calcium, magnesium, ammonium and alkyiammonium; acid addition salts of pharmaceutically acceptable inorganic acids such as hydrochloric, orthophdsphoric, sulphuric, phosphoric, nitric, carbonic, boric, sulfamic and hydrobromic acids; or salts of pharmaceutically acceptable organic acids such as acetic, propionic, butyric, tartaric, maleic, hydroxymaleic, fumaric, citric, lactic, mucic, gluconic, benzoic, succinic, oxalic, phenyiacetic, methanesulphonic, trihalomethanesulphonic, to!uenesu!phonic, benzenesulphonic, salicylic, suiphaniltc, aspartic, glutamic, edetic, stearic, palmitic, oleic, (auric, pantothe
- the methods and compositions according to the invention further include magnesium ions, preferably elevated magnesium ions i.e. over normal plasma concentrations.
- the magnesium is divalent and present at a concentration of 800mM or !ess, O.SrnM to 800m , 10m Ml to 600m , 15mM to SOQmM, 20mM to 400m M, 20mM or 400mM, more preferably 20mM.
- Magnesium sulphate and magnesium chloride are suitable sources in particular magnesium sulphate.
- the inventor has also found that the inclusion of the magnesium ions with (i) a compound selected from at least one of a potassium channel opener, a potassium channel agonist and an adenosine receptor agonist; and (it) an antiarrhythmic agent or a local anaesthetic may also reduce injury.
- the effect of the particular amounts of magnesium ions is to control the amount of ions within the intracellular environment. Magnesium ions tend to be increased or otherwise restored to the levels typically found in a viable, functioning cell.
- composition useful in the methods according to the invention may further include a source of magnesium in an amount for increasing the amount of magnesium in a cell in body tissue.
- a method of increasing blood pressure in a subject that has suffered a life threatening hypotension or shock including the administration of a composition including i) a compound selected from at least one of a potassium channel opener, a potassium channel agonist and an adenosine receptor agonist; and (ii) an antiarrhythmic agent or a local anaesthetic and an elevated source of magnesium tons.
- the composition may also include or be administered with an anti-inflammatory agent and/or metabolic fuel.
- Potassium If potassium is present in the composition it will typicall be present in an amount at physiological levels to ensure that the blood concentration of the subject is less than 10mM or 3 to 6m . This means that when the composition is administered, the cell membrane remains in a more physiological polarised state thereby minimising potential damage to the cell, tissue or organ. High concentrations or concentrations above physiological levels of potassium would result in a hyperkaiemic composition. At these concentrations the heart would fee arrested alone from the depo!arisation of the cell membrane.
- One advantage of using physiological concentrations of potassium is that it renders the present composition less injurious to the subject, in particular paediatric subjects such as neonates/infants.
- High potassium has been linked to an accumulation of calcium which may be associated with irregular heart beats during recovery, heart damage and cell swelling. Neonates/infants are even more susceptible than adults to high potassium damage during cardiac arrest. After surgery a neonate/infant's heart may not return to normal for many days, sometimes requiring intensive therapy or life support.
- Adenosine receptor agonist Adenosine receptor agonist
- component (i) of the composition ma be an adenosine receptor agonist.
- adenosine receptor agonist may be replaced or supplemented by a compound that has the effect of raising endogenous adenosine levels. This may be particularly desirable where the compound raises endogenous adenosine levels in a local environment within a body.
- the effect of raising endogenous adenosine may be achieved by a compound that inhibits cellular transport of adenosine and therefore removal from circulation or otherwise slows its metabolism and effectively extends its half-life (for example, dipyridamole) and/or a compound that stimulates endogenous adenosine production such as purine nucleoside analogue AcadesineTM or AICA- riboside (5-amino-4-irnidazo!e carboxamide ribonucleoside).
- a compound that inhibits cellular transport of adenosine and therefore removal from circulation or otherwise slows its metabolism and effectively extends its half-life for example, dipyridamole
- a compound that stimulates endogenous adenosine production such as purine nucleoside analogue AcadesineTM or AICA- riboside (5-amino-4-irnidazo!e carboxamide ribonucleoside).
- AcadesineTM is desirably administered to produce a plasma concentration of around 50 ⁇ but may range from 1 ⁇ to 1 mM or more preferably from 20 to 200 M.
- AcadesineTM has shown to be safe in humans from doses given orally and/or intravenous administration at 10, 5, 50, and 00 mg/kg body weight doses.
- Suitable adenosine receptor agonists may be selected from: N 6 - cydopentyladenosine (CPA), N-ethylcarboxamido adenosine (NECA), 2-[p-(2- carboxyethyl)phenethyl-amino- 5'- -ethylcarboxamido adenosine (CGS-21680), 2- chloroadenosine, N 8 -[2- ⁇ 3,5- demethoxyphenyi)-2- ⁇ 2-methox phenyl]ethyladenosine, 2-chloro-N s - cydopentyladenosine (CCPA), N-(4-aminobenzyi)-9- [5-(methylcarbonyi)- beta-D- robofuranosyl]-adenine (AB-MECA), ([IS-[1 3 ⁇ 3(8*)]]-4-[7 [2 ⁇ (3 ⁇ ! ⁇ -
- AMP579 N 8 -(R)-phenylisopropyladenosine (R-PLA), aminophenylethyladenosine (APNEA) and_cyclohexyladenosine (CHA).
- Others include full adenosine A1 receptor agonists such as N-[3- ⁇ R)-tetrahydrofuranyl]-6-aminopurine riboside (CVT-510), or partial agonists such as CVT-2759 and allosteric enhancers such as PQ81723.
- agonists include N6-cycfopenty!-2-(3- phenylaminocarbonyltriazene-l -yl)adenosine (TCPA), a ver selective agonist with high affinity for the human adenosine A1 receptor, and allosteric enhancers of A1 adenosine receptor includes the 2-amino-3- naphthoyithiophenes,
- the A1 adenosine receptor agonist is CCPA.
- the concentration of adenosine receptor agonist in the composition maybe 0.0000001 to 100 mM, preferably 0.001 m to 50 mM and most preferably 0.1 mM to 25 m . In one embodiment, the concentration of the adenosine receptor agonist in the composition is about 19 mM,
- the contact concentration of adenosine receptor agonist may be the same or less than the composition concentration set out above
- composition is diluted with a pharmaceutically acceptable carrier, including but not limited to blood, saline or a physiological ionic solution, the dosage of the composition may be adapted to achieve the most preferred contact concentrations.
- a pharmaceutically acceptable carrier including but not limited to blood, saline or a physiological ionic solution
- component (i) of the composition may be a potassium channel opener.
- Potassium channel openers are agents which act on potassium channels to open them through a gating mechanism. This results in efflux of potassium across the membrane along its electrochemical gradient which is usually from inside to outside of the cell.
- potassium channels are targets for the actions of transmitters, hormones, or drugs that modulate cellular function
- the potassium channel openers include the potassium channel agonists which also stimulate the activity of the potassium channel with the same result
- there are diverse classes of compounds which open or modulate different potassium channels for example, some channels are voltage dependent, some rectifier potassium channels are sensitive to ATP depletion, adenosine and opioids, others are activated by fatty acids, and other channels are modulated by ions such as sodium and calcium (ie. channels which respond to changes in cellular sodium and calcium). More recently, two pore potassium channels have been discovered and thought to function as background channels involved in the modulation of the resting membrane potential.
- Potassium channel openers may be selected from the group consisting of: nicorandil, diazoxide, minoxidil, pinacidil, aprikalim, cromokulim and derivative U- 89232, P-1075 (a selective plasma membrane KATP channel opener), emaka!im, YM- 934, (+)-7,8- dihydro-6, 6-dimethyt-7-hydroxy-8-(2-oxo-1-pipendinyl)-6H-pyrano[2,3-1] benz-2, 1, 3- oxadiazole (NIP- 121), RG316930, RV 29009, SDZPCQ400, rimakalim, symakalim, YM099, 2-(7,8-dihydro-6,e-dimethyl-6H-[1 ,4]oxazino[2,3- f][2,1 ,3]benzoxadiazol-8-yl) pyridine N-oxide,
- potassium channel openers may be selected from BK-activators (also called BK-openers or 8K(Ca)-type potassium channel openers or large-conductance calcium- activated potassium channel openers) such as benzimidazoione derivatives NS004 (5- tnfluoromethyl-1-(5-chloro-2-hydroxyphenyf ⁇ -1,3- dihydro-2H-benzfmidazo!e-2-one), NS1819 (1 ,3-dihydro-1-[2-hydroxy-5- (trifluoromethyl)phenyi3-5-(trifluoromethyl)-2H- benzimidazol-2-one), NS1608 (N-(3- ⁇ (thfluoromethyl)phenyl)-N , -(2-hydroxy-5- chlorophenyl)urea), B S-204352, retigabine (also GABA agonist).
- BK-activators also called BK-openers or 8K(Ca)-type potassium channel openers or large-conductance calcium
- Diazoxide and nicorandil are particular examples of potassium channel openers or agonists.
- Diazoxide is a potassium channel opener and in the present invention it is believed to preserve ion and volume regulation, oxidative phosphorylation and mitochondrial membrane integrity (appears concentration dependent). More recently, diazoxide has been shown to provide cardioprotection by reducing mitochondrial oxidant stress at reoxygenation. At present it is not known if the protective effects of potassium channel openers are associated with modulation of reactive oxygen species generation in mitochondria.
- concentration of the diazoxide is between about 1 to 200uM. Typically this is as an effective amount of diazoxide. More preferably, the contact concentration of diazoxide is about 10 ⁇ .
- Nicorandil is a potassium channel opener and nitric oxide donor which can protect tissues and the microvascular integrity including endothelium from ischemia and reperfusion damage. Thus it can exert benefits through the dual action of opening KATP channels and a nitrate-like effect. Nicorandil can also reduce hypertension by causing blood vessels to dilate which allows the heart to work more easily by reducing both preload and afterload. it is also believed to have anti-inflammatory and antiproliferative properties which may further attenuate ischemia/reperfusion injury.
- potassium channel openers may act as indirect calcium antagonists, ie they act to reduce calcium entry into the cell by shortening the cardiac action potential duration through the acceleration of phase 3 repolarisation, and thus shorten the plateau phase. Reduced calcium entry is thought to involve L-type calcium channels, but other calcium channels may also be involved.
- Some embodiments of the invention utilise direct calcium antagonists, the principal action of which is to reduce calcium entr into the cell. These are selected from at least five major classes of calcium channel blockers as explained in more detail below. It will foe appreciated that these calcium antagonists share some effects with potassium channel openers, particularly ATP-sensitiv ⁇ potassium channel openers, by inhibiting calcium entry into the cell.
- Adenosine as well as functioning as an adenosine receptor agonist is also particularly preferred as the potassium channel opener or agonist.
- Adenosine is capable of opening the potassium channel, hyperpolarising the cell, depressing metabolic function, possibly protecting endothelial cells, enhancing preconditioning of tissue and protecting from ischaemia or damage.
- Adenosine is also an indirect calcium antagonist, vasodilator, antiarrhythmic, antiadrenergic, free radical scavenger, arresting agent, anti- inflammatory agent (attenuates neutrophil activation), analgesic, metabolic agent and possible nitric oxide donor. More recently, adenosine is known to inhibit several steps which can lead to slowing the blood clotting process. In addition, elevated levels of adenosine in the brain has been shown to cause sleep and may be involved in different forms or dormancy. An adenosine analogue, 2-chloro-adenosine, may be used.
- the concentration of potassium channel opener or agonist in the composition may be 0.00QQ0Q1 to 100 mM, preferably 0.001 mM to 50 m and most preferably 0.1 mM to 25 mM. In one embodiment, the concentration of the potassium channel opener in the composition is about 19 mM.
- the contact concentration of potassium channel opener or agonist may be the same or less than the composition concentration set out above
- the dosage of the composition may be adapted to achieve the most preferred contact concentrations.
- the potassium channel opener, potassium channel agonist and/or adenosine receptor agonist has a blood half-life of less than one minute, preferably less than 20 second.
- composition useful in methods according to the invention also includes an antiarrhythmic agent.
- Antiarrhythmic agents are a group of pharmaceuticals that are used to suppress fast rhythms of the heart (cardiac arrhythmias). The following table indicates the classification of these agents.
- the antiarrhythmic agent may induce local anaesthesia (or otherwise be a local anaesthetic), for example, mexiletine, diphenylhydantoin, prilocaine, procaine, mepivocaine, quinidine, disopyramide and Class 1 B antiarrhythmic agents.
- local anaesthesia or otherwise be a local anaesthetic
- mexiletine for example, mexiletine, diphenylhydantoin, prilocaine, procaine, mepivocaine, quinidine, disopyramide and Class 1 B antiarrhythmic agents.
- the antiarrhythmic agent is a class l or class Hi agent
- Amiodarone is a preferred Class III antiarrhythmic agent.
- the antiarrhythmic agent blocks sodium channels.
- the antiarrhythmic agent is a class IB antiarrhythmic agent.
- Class 1 B antiarrhythmic agents include iidocaine or derivatives thereof, for example, QX-314 is a quaternary Iidocaine derivative (i.e., permanently charged) and has been shown to have longer-lasting local anesthetic effects than lidocaine-HCI alone.
- the class 1 B antiarrhythmic agent is lidocaine.
- lidocaine is also known to be capable of acting as a local anaesthetic probably by blocking sodium fast channels, depressing metabolic function, lowering free cytosolic calcium, protecting against enzyme release from ceils, possibly protecting endothelial cells and protecting against myofilament damage. At lower therapeutic concentrations lidocaine normally has little effect on atrial tissue, and therefore is ineffective in treating atria! fibrillation, atrial flutter, and supraventricular tachycardias.
- Lidocaine is also a free radical scavenger, an antiarrhythmic and has anti-inflammatory and anti-hypercoagulable properties. It must also be appreciated that at non-anaesthetic therapeutic concentrations, local anaesthetics like lidocaine would not completely block the voltage-dependent sodium fast channels, but would down-regulate channel activity and reduce sodium entry. As antiarrhythmic, lidocaine is believed to target small sodium currents that normally continue through phase 2 of the action potential and consequently shortens the action potential and the refractory period.
- sodium channel blockers include compounds that act to substantially block sodium channels or at least downregulate sodium channels.
- suitable sodium channel blockers include venoms such as tetrodotoxin and the drugs primaquine, QX, HNS-32 (CAS Registry # 186086-10-2), NS-7, kappa- opioid receptor agonist U50 488, crobenetine, pilsicainide, phenytoin, tocainide, mexiletine, N -1029 (a benzylamino propanamide derivative), RS100642, riluzole, carbamazepine, flecainide, propafenone, amiodarone, sotaloi, imipramine and moricizine, or any of derivatives thereof.
- Other suitable sodium channel blockers include: Vinpocetine (ethyl apovincaminate); and Beta-carboline derivative, nootropic beta-carboline (ambocarb, AMB).
- the composition according to the invention comprises (!) a compound selected from at least one of a potassium channel opener, a potassium channel agonist and an adenosine recepto agonist; and (it) an antiarrhythmic agent or local anaesthetic.
- a compound selected from at least one of a potassium channel opener, a potassium channel agonist and an adenosine recepto agonist e.g., a potassium channel opener, a potassium channel agonist and an adenosine recepto agonist; and (it) an antiarrhythmic agent or local anaesthetic.
- the composition includes an elevated source of magnesium tons.
- the antiarrhythmic agent is a local anaesthetic such as lidocaine.
- the concentration of antiarrhythmic agent or local anaesthetic in the composition may be 0.0000001 to 100 mM, preferablyO.001 mM to 50 mM and most preferably 0.1 mM to 40 mM. In one embodiment, the concentration of antiarrythmic agent or local anaesthetic in the composition is about 37 mm.
- the contact concentration of antiarrhythmic agent of local anaesthetic may be the same or less than the composition concentration set out above.
- composition is diluted with a pharmaceutically acceptable carrier, including but not limited to blood, saline or a physiological ionic solution, the dosage of the composition may be adapted to achieve the most preferred contact concentration, Anti-inflammatory agent
- the composition according to the invention further includes an anti-inflammatory agent.
- Anti-inflammatory agents such as beta-hydroxybutyrate (BOH), niacin and GPR109A can act on the GPR109A receptor (also referred to as hydroxyl-carboxylic acid receptor 2 or HCA-2). This receptor is found on immune cells (monocytes, macrophages), adipocytes hepatocytes, the vascular endothelium, and neurones.
- Valproic acid is also a suitable anti-inflammatory agent
- VPA is a short-chain branched fatty acid with anti-inflammatory n euro- rotective and exon-remodelling effects.
- Valproic acid (VPA) is a histone deacetyiase inhibitor that may decrease cellular metabolic needs foilowing traumatic injury.
- Valproic acid (VPA) has proven to be beneficial after traumatic injury and has been shown to improve survival in lethal models of hemorrhagic shock.
- VPA also is known to have cytoprotective effects from an increase acetylation of nuclear histones, promoting transcriptional activation of deregulated genes, which may confer multi-organ protection. It may also have beneficial effects in preventing or reducing the cellular and metabolic sequelae of ischemia-reperfusion injury and reduce injury to the endothelium through the TGF- ⁇ and VEGF functional pathways.
- the composition according to the invention includes (i) a compound selected from at least one of a potassium channel opener, a potassium channel agonist and an adenosine receptor agonist; (ii) an antiarrhythmic agent or local anaesthetic; and (iii) an anti-inflammatory agent.
- a compound selected from at least one of a potassium channel opener, a potassium channel agonist and an adenosine receptor agonist e.g., an antiarrhythmic agent or local anaesthetic
- an anti-inflammatory agent e.g., an anti-inflammatory agent.
- the anti-inflammatory agent activates a HCA-2 receptor such as beta-hydroxybutyrate (BOH).
- BOH beta-hydroxybutyrate
- heparin low-molecular- weight heparin
- non-steroidal anti-inflammatory agents anti- platelet drugs and glycoprotein (GP) ilb/lila receptor inhibitors, statins, angiotensin converting enzyme (ACE) inhibitor, angiotensin blockers and antagonists of substance P.
- ACE angiotensin converting enzyme
- protease inhibitors are indinavir, nelfinavir, ritonavir, lopinavir, amprenavir or the broad- spectrum protease inhibitor aprotinin, a low- mo ecular-weight heparin (LMWH) is enoxaparin, non-steroida!
- anti-inflammatory agent are indomethacin, ibuprofen, rofeco ib, naproxen or fluoxetine, an anti-platelet drug such as aspirin, a glycoprotein (GP) lib/Ilia receptor inhibitor is abciximab, a statin is pravastatin, an angiotensin converting enzyme (ACE) inhibitor is captopril and an angiotensin blocker is valsartin.
- GP glycoprotein
- lib/Ilia receptor inhibitor is abciximab
- a statin is pravastatin
- an angiotensin converting enzyme (ACE) inhibitor is captopril
- an angiotensin blocker is valsartin.
- compositions useful in the methods according to the invention to deliver improved management of inflammation and dotting in order to reduce injury to cells, tissues or organs.
- composition according to the invention may be administered together with any one or more of these agents.
- protease inhibitors attenuate the systemic inflammatory response in patients undergoing cardiac surgery with cardiopulmonary bypass, and other patients where the inflammatory response has been heightened such as AIDS or in the treatment of chronic tendon injuries.
- Some broad spectrum protease inhibitors such as aprotinin are also reduce blood loss and need for blood transfusions in surgical operations such as coronary bypass.
- composition according to the invention comprises (i) a compound selected from at least one of a potassium channel opener, a potassium channel agonist and an adenosine receptor agonist; (ii) an antiarrhythmic agent or a local anaesthetic; (iii) at least one of a citrate and a general anaesthetic; and (iv) an anti-inflammatory agent.
- the composition includes an elevated source of magnesium.
- the anti-inflammatory agent activates a HCA-2 receptor such as beta- hydroxy butyrate (BOH).
- BOH beta- hydroxy butyrate
- Valproic acid is also a suitable anti-inflammatory agent.
- Valproic acid (VPA) is a histone deacetylase inhibitor that may decrease cellular metabolic needs following traumatic injury.
- Valproic acid (VPA) has proven to be beneficial after traumatic injury and has been shown to improve survival in lethal models of hemorrhagic shoek.
- VPA also is known to have cytoprotecttve effects from an increase acetylation of nuclear histones, promoting transcriptional activation of deregulated genes, which may confer multi-organ protection. It may also have beneficial effects in preventing or reducing the cellular and metabolic sequelae of ischemia-reperfusion injury and reduce injury to the endothelium through the TGF- ⁇ and VEGF functional pathways,
- Sphingosine-1 -phosphate (S1 ) is also a suitable anti-inflammatory agent.
- concentration of anti-inflammatory agent in the composition may be O.OQ00001 to 300 mM, preferably 0.001 m . to 50 m and most preferably 0.1 mM to 10 mM,
- the contact concentration of anti-inflammatory agent may be the same or less than the composition concentration as set out above.
- composition is diluted with a pharmaceutically acceptable carrier, including but not limited to blood, saline or a physiological ionic solution, the dosage of the composition may be adapted to achieve the most preferred contact concentrations.
- a pharmaceutically acceptable carrier including but not limited to blood, saline or a physiological ionic solution
- the composition according to the invention further includes a metabolic fuel.
- the metabolic fuel is a citrate.
- a citrate include citrate and derivatives, thereof such as citric acid, salts of citrate, esters of citrate, polyatomic anions of citrat or other ionic or drug complexes of citrate.
- citrate in ts various forms is not included in the compositio it can be administered separately in a blood, blood:crystalioid ratio or crystalloid solution and mixed to the preferred level in the composition prior to administration to the body, organ, tissue or cell.
- the form of citrate includes citrate phosphate detrose (CPD) solution, magnesium citrate, sodium citrate, potassium citrate or sildenafil citrate, more preferably CPD.
- CPD citrate phosphate detrose
- the composition according to the invention includes (i) a compound selected from at least one of a potassium channel opener, a potassium channel agonist and an adenosine receptor agonist; (ii) an antiarrhythmic agent or a local anaesthetic; and (iii) a metabolic fuel.
- a compound selected from at least one of a potassium channel opener, a potassium channel agonist and an adenosine receptor agonist e.g., an antiarrhythmic agent or a local anaesthetic
- a metabolic fuel e.g., a compound selected from at least one of a potassium channel opener, a potassium channel agonist and an adenosine receptor agonist.
- an antiarrhythmic agent or a local anaesthetic e.g., a local anaesthetic
- a metabolic fuel e.g., a compound selected from at least one of a potassium channel opener, a potassium channel agonist and an adenosine receptor agonist.
- the composition according to the inventio may include (i) a compound selected from at least one of a potassium channel opener, a potassium channel agonist and an adenosine receptor agonist; (ii) an antiarrhythmfc agent or a local anaesthetic; (iii) a metabolic fuel; and (iv) an anti-inflammatory agent.
- the composition includes an elevated source of magnesium ions.
- the concentration of metabolic fuel in the composition may be 0.0000001 to 100 mM, preferably 0.001 mM to 50 mM and most preferably 0.1 mM to 0 mM. In one embodiment, the concentration of citrate in the composition is about 2.1 mM.
- the contact concentration of metabolic fuel may be the same or less than the composition concentration set out above. It will be appreciated if the composition is diluted with a pharmaceutically acceptable carrier, including but not limited to blood, saline or a physiological ionic solution, the dosage of the composition may be adapted to achieve the most preferred contact concentrations.
- a pharmaceutically acceptable carrier including but not limited to blood, saline or a physiological ionic solution
- anti-adrenergics such as beta-blockers, for example, esmolol, atenolol, metoprolol and propranolol could be used in combination with the potassium channel opener, potassium channel agonist and/or adenosine receptor agonist to reduce calcium entry into the cell.
- the beta- blocker is esmolol.
- alpha(1)-adrenoceptor-antagonists such as prazosin, could be used instead in combination with the potassium channel opener, potassium channel agonist and/or adenosine receptor agonist to reduce calcium entry into the cell and therefore calcium loading.
- the antiadrenergic is a beta-blocker.
- the beta-blocker is esmolol.
- Na7Ca 2+ exchange inhibitors may include benzamyt, KB-R7943 (2-[4-(4- Nitrobenzyloxy)phenyl]ethy!3isothiourea mesylate) or SEA0400 (2-[4-[(2,5- difluorophenyl)methoxy]phenoxy]-5 ⁇ ethoxyaniline).
- Some embodiments of the invention utilise calcium channel blockers which are direct calcium antagonists, the principal action of which is to reduce calcium entry into the cell.
- Such calcium channel blockers may be selected from three different classes: 1 ,4- dihydropyridines (eg. nitrendipine), phenylalkylamines (eg, verapamil), and the benzodiazepines (e.g. diltiazem, nifedipine). It will be appreciated that these calcium antagonists share some effects with potassium channel openers, particularly ATP- sensitive potassium channel openers, by inhibiting calcium entry into the cell.
- Calcium channel blockers are also called calcium antagonists or calcium blockers. They are often used clinically to decrease heart rate and contractility and relax blood vessels. They may be used to treat high blood pressure, angina or discomfort caused by ischaemia and some arrhythmias, and they share many effects with beta-blockers (see discussion above).
- Benzodiazepines eg Diltiazem.
- Dihydropyridines eg nifedipine, Nicardipine, nimodipine and many others, 3.
- Phenylalkylamines eg Verapamil, Diarylaminopropylamine ethers; eg Bepridil, 5.
- Benzimtdazole-substituted tetra lines eg ibef radii.
- L-type calcium channels L-type calcium channels
- a!pha2, beta, gamma, delta subunits are also present.
- Different sub-classes of L-type channel are present which may contribute to tissue selectivity.
- Bepridil is a drug with Na+ and K+ channel blocking activities in addition to L-type calcium channel blocking activities.
- Mibef radii is a drug with T-type calcium channel blocking activity as well as L- type calcium channel blocking activity.
- Nifedipine and related dihydropyridines do not have significant direct effects on the atrioventricular conduction system or sinoatrial node at normal doses, and therefore do not have direct effects on conduction or automaticity. While other calcium channel blockers do have negative chronotropic/dromotropic effects (pacemaker activity/conduction velocity). For example, Verapamil (and to a lesser extent diltiazem) decreases the rate of recovery of the slow channel in AV conduction system and SA node, and therefore act directly to depress SA node pacemaker activity and slow conduction.
- Verapamil is also contraindicated in combination with beta-blockers due to the possibility of AV block or severe depression of ventricular function.
- mibefradil has negative chronotropic and dromotropic effects.
- Calcium channel blockers (especially verapamil) may also be particularly effective in treating unstable angina if underlying mechanism involves vasospasm.
- Omega conotoxin MVS I A (S X-111) is an N type calcium channel blocker and is reported to be 100-1000 fold more potent than morphine as an analgesic but is not addictive. This conotoxin is being investigated to treat intractible pain.
- SNX-482 a further toxin from the venom of a carnivorous spider venom, blocks R-type calcium channels. The compound is isolated from the venom of the African tarantula, Hysterocrates gigas, and is the first R-type calcium channel blocker described. The R- type calcium channel is believed to play a role in the body's natural communication network where it contributes, to the regulation of brain function.
- Calcium channel blockers from animal kingdom include Kurtoxin from South African Scorpion, SNX-482 from African Tarantula, Taicatoxin from the Australian Taipan snake, Agatoxin from the Funnel Web Spider, Atracotoxin from the Blue Mountains Funnel Web Spider, Conotoxin from the Marine Snail, HWTX-i from the Chinese bird spider, Grammotoxin SIA from the South American Rose Tarantula. This list also includes derivatives of these toxins that have a calcium antagonistic effect.
- Direct ATP-sensitive potassium channel openers eg nicorandil, aprikalem
- indirect ATP-sensitive potassium channel openers eg adenosine, opioids
- One mechanism believed for ATP-sensitive potassium channel openers also acting as calcium antagonists is shortening of the cardiac action potential duration by accelerating phase 3 repoiarisation and thus shortening the plateau phase.
- the enhanced phase 3 repoiarisation may inhibit calcium entry into the cell by blocking or inhibiting L-type calcium channels and prevent calcium (and sodium) overload in the tissue cell.
- Calcium channel blockers can be selected from nifedipine, nicardipine, nimodipine, nisoldipine, iercanidipine, telodipine, angizem, a!tiazem, bepridil, amlodipine, felodipine, isradipine and cavero and other racemic variations.
- calcium entry could be inhibited by other calcium blockers which could be used instead of or in combination with adenosine and include a number of venoms from marine or terrestrial animals such as the omega-conotoxin QVIA (from the snail conus geographus) which selectively blocks the N-type calcium channel or omega-agatoxin MIA and IVA from the funnel web spider Ageletnopsis aperta which selectively blocks R- and P/Q-type calcium channels respectively.
- mixed voltage-gated calcium and sodium channel blockers such as NS-7 to reduce calcium and sodium entry and thereby assist cardioprotection.
- the calcium channel blocker is nifedipine.
- the methods and compositions according to the invention further include an opioid.
- an opioid particularly D-Pen[2,5]enkephalin (DPDPE), may also result in significantly less damage to the cell, tissue or organ.
- DPDPE D-Pen[2,5]enkephalin
- composition according to the invention further includes an opioid.
- Opioids also known or referred to as opioid agonists, are a grou of drugs that inhibit opium (Gropion, poppy juice) or morphine-like properties and are generally used clinically as moderate to strong analgesics, in particular, to manage pain, both peri- and post-operatively. Other pharmacological effects of opioids include drowsiness, respiratory depression, changes in mood and mental clouding without loss of consciousness. Opioids are also believed to be involved as part of the 'trigger' in the process of hibernation, a form of dormancy characterised by a fail in normal metabolic rate and normal core body temperature. In this hibernating state, tissues are better preserved against damage that may otherwise be caused by diminished oxygen or metabolic fuel supply, and also protected from ischemia reperfusion injury.
- opioid peptides There are three types of opioid peptides: enkephalin, endorphin and dynorphin.
- Opioids act as agonists, interacting with stereospectfic and saturable binding sites, in the heart, brain and other tissues.
- Three main opioid receptors have been identified and cloned, namely mu, kappa, and deita receptors. All three receptors have consequently been classed in the G-protein coupled receptors family (which class includes adenosine and bradykinin receptors).
- Opioid receptors are further subtyped, for example, the delta receptor has two subtypes, delta- 1 and delta-2.
- opioid agonists include for example TA -67, 8W373U86, SNC80 ([(+)-4-[alpha(R)- aipha-[(2S,5R)-4-allyl-2,5- dimethyl-1-piperazinyi3-(3-methoxybenzyl)-N,N- diethy!benzamide), (+)BW373U86, DADLE, ARD-353 [4-((2R5S) ⁇ 4-(R ⁇ 4 ⁇ diethyicarbamoyiphenyl)(3- hydroxyphenyl)methyl)-2, 5-dimethylpiperazin- 1- ylmethyl)benzoic acid], a nonpepttde delta receptor agonist, DPI-221 [4-((a!pha- S) ⁇ alpha-((2S,5R)-2,5-dimethyl-4-(3- fSuorobenzy!-1-pfperazinyi)benzyl)-N,N- diethy
- Cardiovascular effects of opioids are directed within the intact body both centrally (ie, at the cardiovascular and respiratory centres of the hypothalamus and brainstem) and peripherally (ie, heart myocytes and both direct and indirect effects on the vasculature).
- opioids have been shown to be involved in vasodilation.
- Some of the action of opioids on th heart and cardiovascular system may involve direct opioid receptor medtated actions or indirect, dose dependent non-opioid receptor mediated actions, such as ion channel blockade which has been observed with antiarrhythmic actions of opioids, such as aryiacetamide drugs.
- the heart is capable of synthesising or producing the three types of opioid peptides, namely, enkephalin, endorphin and dynorphin.
- opioid peptides namely, enkephalin, endorphin and dynorphin.
- delta and kappa opioid receptors have been identified on ventricular myocytes.
- opioids are considered to provide cardioprotective effects, by limiting ischaemic damage and reducing the incidence of arrhythmias, which are produced to counter-act high levels of damaging agents or compounds naturally released during ischemia. This may be mediated via the activation of ATP sensitive potassium channels in the sarcolemma and in the mitochondrial membrane and involved in the opening potassium channels. Further, it is also believed that the cardioprotective effects of opioids are mediated via the activation of ATP sensitive potassium channels in the sarcolemma and in the mitochondrial membrane. It will be appreciated that the opioids include compounds which act both directly and indirectly on opioid receptors.
- Opioids also include indirect dose dependent, non- opioid receptor mediated actions such as ion channel blockade which have been observed with the antiarrhythmic actions of opioids.
- Opioids and opioid agonisis may be peptidic or non-peptidic
- the opioid is selected from enkephalins, endorphins and dynorphins.
- the opioid is an enkephalin which targets delta, kappa and/or mu receptors. More preferably the opioid is selected from delta-1 -opioid receptor agonists and de!ta-2-opioid receptor agonists, D ⁇ Pen [2, 5]enkephaiin (DPDPE) is a particularly preferred Delta-1 -Opioid receptor agonist.
- the opioid is administered at 0.001 to 10 mg/kg body weight, preferabl 0.01 to 5 mg/kg, or more preferably 0.1 to 1,0 mg/kg.
- compositions according to the invention may further include the use of at least one compound for minimizing or reducing the uptake of water by a cell in the cell, tissue or organ.
- a compound for minimizing or reducing the uptake of water by a ceil in the tissue tends to control water shifts, ie, the shift of water between the extracellular and intracellular environments. Accordingly, these compounds are involved in the control or regulation of osmosis.
- a compound for minimizing or reducing the uptake of water by a cell in the tissue reduces ceil swelling that is associated with Oedema, such as Oedema that can occur during ischemic injury.
- An impermeant according to the present invention may be selected from one or more of the group consisting of: sucrose, pentastarch, hydroxyethyi starch, rafftnose, mannitol, gluconate, lactobionate. and colloids.
- Suitable colloids include, but not limited to, Dexfran-70, 40, 50 and 60, hydroxyethyi starch and a modified fluid gelatin.
- a colloid is a composition which has a continuous liquid phase in which a solid is suspended in a liquid. Colloids can be used clinically to help restore balance to water and ionic distribution between the intracellular, extracellular and blood compartments in the body after an severe injury. Colloids can also be used in solutions for organ preservation Administration of crystalloids can also restore water and ionic balance to the body but generally require greater volumes of administration because they do not have solids suspended in a liquid. Thus volume expanders may be colloid-based or crystalloid- ased.
- Colloids include albumin, hetastarch, polyethylene glycol (PEG), Dextran 40 and Dextran 60.
- Other compounds that could be selected for osmotic purposes include those from the major classes of osmolytes found in the animal kingdom including polyhydric alcohols (poiyols) and sugars, other amino acids and amino-acid derivatives, and methylated ammonium and sulfonium compounds.
- Substance P an important pro- inflammatory neuropeptide is known to lead to ceil oedema and therefore antagonists of substance P may reduce cell swelling.
- antagonists of substance P (-specific neurokinin-1) receptor (NK-1) have been shown to reduce inflammatory liver damage, i.e., oedema formation, neutrophil infiltration, hepatocyte apoptosis, and necrosis.
- NK-1 antagonists include CP-96,345 or [(2S,3S)-cis-2- (d(phenyimethyl)-N-((2-methoxyphenyl)-methyS)-1-azabicyciQ(2.2,2.)-octan-3-amine (CP-96,345)] and L-733,06O or [(2S,3S)3-([3,5-bis(trifluoromethyl)phenyl]methoxy)-2- phenylpiperidine .
- NK(1)> receptor antagonist with subnanomolar affinity for the human N (1) receptor (K(i): 0.45 nM) and over 200-fold selectivity toward K(2) and NK(3) receptors.
- Antagonists of neurokinin receptors 2 that may also reduce cell swelling include SR48968 and NK-3 include SR142801 and SB-222200.
- Blockade of mitochondria! permeability transition and reducing the membrane potential of the inner mitochondrial membrane potential using cyclosporin A has also been shown to decrease ischemia-induced cell swelling in isolated brain slices.
- g!utamate-receptor antagonists (AP5/CNQX) and reactive oxygen species scavengers (ascorbate, Troiox(R), dimethylthiourea, tempol(R)) also showed reduction of cell swelling.
- the compound for minimizing or reducing the uptake of water by a cell in a tissue can also be selected from any one of these compounds.
- Suitable energy substrate can be selected from one or more from the group consisting of: glucose and other sugars, pyruvate, lactate, giutamate, g!utamine, aspartate, arginine, ectoine, taurine, N-acetyl-beta-lysine, alanine, proline, beta- hydroxy butyrate and other amino acids and amino acid derivatives, trehalose, floridoside, glycerol and other polyhydric alcohols (poiyols), sorbitol, myo-innositol, pinitol, insulin, alpha-keto glutarate, malate, succinate, triglycerides and derivatives, fatty acids and carnitine and derivatives.
- the at least one compound for minimizing or reducing the uptake of water by the cells in the tissue is an energy substrate.
- the energy substrate helps with recovering metabolism.
- the energy substrate can be selected from one or more from the group consisting of: glucose and other sugars, pyruvate, lactate, glutamate, glutamtne, aspartate, arginine, ectoine, taurine, N-acetyl- beta- lysine, alanine, proline and other amino acids and amino acid derivatives, trehalose, floridoside, glycerol and other polyhydric alcohols (poiyols), sorbitol, myo- innositol, ptnitoi, insulin, alpha-keto glutarate, malate, succinate, triglycerides and derivatives, fatty acids and carnitine and derivatives.
- energy substrates are sources of reducing equivalents for energy transformations and the production of ATP in a cell, tissue or organ of the body
- a direct supply of the energy reducing equivalents could be used as substrates for energy production.
- a supply of either one or more or different ratios of reduced and oxidized forms of nicotinamid adenine dinucleotide (e.g. NAD or NADP and NADH or NADPH) or flavin adenine dinucleotides (FADH or FAD) could be directly used to supply bond energy for sustaining ATP production in times of stress, Beta- hydroxy butyrate is a preferred energy substrate.
- H 2 S hydrogen sulphide
- H2S donors eg NaHS
- the presence of hydrogen sulphide (H 2 S) or H2S donors (eg NaHS) may help metabolise these energy substrates by lowering energy demand during arrest, protect and preserve the whole body, organ, tissue or cell during periods of metabolic imbalance such ischemia, reperfusion and trauma.
- Concentrations of hydrogen sulfide above 1 microivl (10-6 ) concentration can be a metabolic poison that inhibits respiration at Respiratory Comple t V, which is part of the mitochondrial respiratory chain that couples metabolising the high energy reducing equivalents from energy substrates to energ (ATP) generation and oxygen consumption.
- Respiratory Comple t V which is part of the mitochondrial respiratory chain that couples metabolising the high energy reducing equivalents from energy substrates to energ (ATP) generation and oxygen consumption.
- ATP energ
- the presence of a vestig sulphur cycle would be consistent with current ideas on the evolutionary origin of mitochondria and their appearance in eukaryote cells from a symbiosis between a sulfide-producing host cell and a suifide-oxidizing bacterial symbiont.
- hydrogen sulphide (H 2 S) or H 2 S donors may be energy substrates themselves in addition to improving the metabolism of other energy substrates.
- the invention provides a composition as described above further including hydrogen sulphide or a hydrogen sulfide donor.
- the compound for minimizing or reducing the uptake of water by the cells in the tissue is PEG
- PEG reduces water shifts as an impermeant but also may preserve cells from immune recognition and activation.
- Irrtpermeant agents such as PEG, sodium gluconate, sucrose, !actobionate and raffinose, trehalose, are too large to enter the cells and hence remain in the extracellular spaces within the tissue and resulting osmotic forces prevent cell swelling that would otherwise damage the tissue, which would occur particularly during storage of the tissue.
- the concentration of the compound for minimizing or reducing the uptake of water by the cells in the tissue is between about 5 to 500m . Typically this is an effective amount for reducing the uptake of water by the cells in the tissue. More preferably, the concentration of the compound for reducing the uptake of water by the cells in the tissue is between about 20 and 200mSVl. Even more preferably the concentration of the compound for reducing the uptake of water by the cells in the tissue is about 70m M to 140 mM.
- the contact concentration of the compound for minimizing or reducing the uptake of water by the cells in the tissue is the same or less than the composition concentration set out above.
- composition is diluted with a pharmaceuticall acceptable carrier, including but not limited to blood, saline or a physiological ionic solution, the dosage of the composition may be adapted to achieve the most preferred contact concentrations,
- the composition useful in the methods according to the invention may include more than one compound for minimizing or reducing the uptake of water by the cells in the tissue.
- a combination of impermeants raffinose, sucrose and pentastarch
- a combination of colloids, and fuel substrates may be included in the composition.
- the methods and compositions according to the invention may further include a surfactant that has rheologic, antt-thrombotic, anti-inflammatory and cytoprotective properties.
- a surfactant that has rheologic, antt-thrombotic, anti-inflammatory and cytoprotective properties.
- surfactants are HCO-80, sodium dodecyl sulfate (SDS), Tween 80, PEG 400, 0.1 to 1% Pluronic 68, F 127 and poloxamer 188 (P188).
- P188 is a surface acting agent with cytoprotective effects of cells, tissues and organs and has been shown to be protective against trauma, electric shock, ischemia, radiation, osmotic stress, heart attack, stroke, burns and haemorrhagic shock.
- Poloxamer 188 was also associated with potentially beneficial changes in membrane protein expression, reduced capillary leakage, and less hemodi!ution in pediatric cardiac surgery.
- Other surfactant-protecting agents such as prostacyclin analog iloprost are also protective and has shown to improve preservation of surfactant function in transplanted lungs.
- the non-ionic surfactant for minimizing or reducing cell damage for the present invention is F 88.
- the methods and compositions according to the invention may further include a reversible myofilament inhibitor such as 2,3-butanedione monoxime (BD ) to arrest, protect and preserve organ function.
- BD 2,3-butanedione monoxime
- Myosin-actin interactions are present in nearly every cell for transport, trafficking, contraction, cytoskeleton viability, BDM has been shown to improve preservation in skeletal muscle, kidney and renal tubules, lung, and heart.
- the myosin inhibitor BDM is the choice for reducing cellular demand and minimizing cell damage during injury or ischemia-reperfusion injury.
- the inventor has also found that the inclusion of a compound for inhibiting transport of sodium and hydrogen ions across a plasma membrane of a cell in the tissue with (i) a compound selected from at least one of a potassium channel opener, a potassium channel agonist and an adenosine receptor agonist; and (ii) a antiarrhythmic agent or local anaesthetic assists in reducing injur and damage.
- composition useful in the methods according to the invention further includes a compound for inhibiting transport of sodium and hydrogen ions across a plasma membrane of a cell in the tissue.
- the compound for inhibiting transport of sodium and hydrogen across the membrane of the cell n the tissue is also referred to as a sodium hydrogen exchange inhibitor.
- the sodium hydrogen exchange inhibitor reduces sodium and calcium entering the cell.
- the compound for inhibiting transport of sodium and hydrogen across the membrane of the cell in the tissue may be selected from one or more of the grou consisting of Amiloride, EIPA ⁇ 5-(N-entyi-N-isopropyi)-amiioride) ( cariporide (HOE-642), eniporide, Triamterene (2,4,7-tnamino-6-phenylteride), EMD 84021 , EMD 94309, EMD 96785, EMD 85131 and HOE 694.
- B11 B-513 and T-162559 are othe inhibitors of the isoform 1 of the N.a+/H+ exchanger.
- the sodium hydrogen exchange inhibitor is Amiloride ⁇ N-amidino- 3,5- diamino-6-chloropyrzi e-2-carboximide hydrochloride di hydrate). Amiloride inhibits the sodium proton exchanger (Na+/H+ exchanger also often abbreviated NHE-1 ) and reduces calcium entering the cell. During ischemia excess ceil protons (or hydrogen ions) are believed to be exchanged for sodium via the Na+/H+ exchanger.
- the concentration of the sodium hydrogen exchange inhibitor in the composition is between about 1.0 nM to 1 ,0 m , More preferably, the concentration of the sodium hydrogen exchange inhibitor in the composition is about 2 ⁇ .
- the contact concentration of the sodium hydrogen exchange inhibitors is the same or less than the composition concentration set out above. It will be appreciated if the composition is diluted with a pharmaceutically acceptable carrier, including but not limited to blood, saline or a physiological ionic solution, the dosage of the composition may be adapted to achieve the most preferred contact concentrations.
- a pharmaceutically acceptable carrier including but not limited to blood, saline or a physiological ionic solution
- composition useful in the methods according to the invention may also include an antioxidant.
- Antioxidants are commonly enzymes or other organic substances that are capable of counteracting the damaging effects of oxidation in the tissue.
- the antioxidant may be selected from one or more of the group consisting of: altopurinol, carnosine, histidine, Coenzyme Q 10, n-acetyl-cysteine, superoxide dismutase (SOD), glutathione reductase (GR), glutathione peroxidase (GP) modulators and regulators, catalase and the other metai!oenzymes, MADPH and NAD(P)H oxidase inhibitors, glutathione, U-74QQ6F, vitamin E, Trolo (soluble form of vitamin E), other tocopherols (gamma and alpha, beta, delta), tocotrtenols, ascorbic acid, Vitamin C, Beta-Carotene (plant form of vitamin A), selenium, Gamma Lino!eie Acid (GLA), alpha-lipoic acid,
- antioxidants include the ACE inhibitors (captopri!, enalapril, iisinopril) which are used for the treatment of arterial hypertension and cardiac failure on patients with myocardial infarction, ACE inhibitors exert their beneficial effects on the reoxygenated myocardium by scavenging reactive oxygen species.
- Other antioxidants that could also be used include beta- mercaptopropionyigiycine, G-phenanthroline, dithiocarbamate, selegilize and desferoxamine (Desferal), an iron chelator, has been used in experimental infarction models, where it exerted some level of antioxidant protection.
- antioxidants include: nitrone radical scavenger alpha-phenyl-tert-N-butyl nitrone (PBN) and derivatives PBN (including disulphur derivatives); N -2-m ercaptopro p i ony I glycine ( PG) a specific scavenger of the OH free radical; lipooxygenase inhibitor nordihydroguaretic acid (NDGA): Alpha Lipoic Acid; Chondroitin Sulfate; L-Cysteine; oxypurinol and Zinc.
- PBN nitrone radical scavenger alpha-phenyl-tert-N-butyl nitrone
- PBN nitrone radical scavenger alpha-phenyl-tert-N-butyl nitrone
- PBN nitrone radical scavenger alpha-phenyl-tert-N-butyl nitrone
- PBN including disulphur derivatives
- the antioxidant is al!opurinol (1H-Pyrazolo[3,4-a]pyrimidine-4-ol).
- Allopurino is a competitive inhibitor of the reactive oxygen species generating enzym xanthin oxidase. Allopurino s antioxidative properties may help preserve myocardial and endothelial functions by reducing oxidative stress, mitochondrial damage, apoptosis and cell death.
- the methods and compositions according to the invention include a cellular transport enzyme inhibitor, such as a nucleoside transport inhibitor, for example, dipyridamole, to prevent metabolism or breakdown of components in the composition such as adenosine.
- a cellular transport enzyme inhibitor such as a nucleoside transport inhibitor, for example, dipyridamole
- the half life of adenosine in the blood is about 10 seconds so the presence of a medicament to substantially prevent its breakdown will maximise the effect of the composition of the present invention.
- Dipyridamole is advantageously included in the composition a concentration from about 0.01 ⁇ to about 10m , preferably 0.05 to 100 ⁇ . Dipyridamole and has major advantages with respect to cardioprotection. Dipyridamole may supplement the actions of adenosine by inhibiting adenosine transport and breakdown leading to increased protection of cells, tissues and organs of the body during times of stress. Dipyridamole may also be administered separately for example by 400mg daily tablets to produce a plasma level of about 0,4 ,ug/m!, or 0.8 ⁇ concentration.
- compositions may be suitable for administration to the tissue in liquid form for example, solutions, syrups or suspensions, or alternatively they may be administered as a dry product for constitution with water or other suitable vehicle before use. Alternatively, the composition may be presented as a dry product for constitution with water or other suitable vehicle.
- Such liquid preparations may be prepared by conventional means with pharmaceutically acceptable additives such as suspending agents, emulsifying agents, non-aqueous vehicles, preservatives and energy sources.
- the invention comprises a composition in tablet form, including nutraceutical or supplement applications and in another form, the invention comprises an aerosol which could be administered via oral, skin or nasal routes.
- composition useful in the methods according to the invention may be suitable for topical administration to the tissue.
- Such preparation may be prepared by conventional means in the form of a cream, ointment, jelly, solution or suspension.
- Aqueous suspensions contain the active materials in admixture with excipients suitable for the manufacture of aqueous suspensions.
- excipients are suspending agents, for example sodium carboxymethyicellulose, methyice!lulose, hydropropyl methylcellulose, sodium alginate, polyvinylpyrrolidone, gum tragaeanth and gum acacia; dispersing or wetting agents may be a naturally-occurring phosphatide, for example, lecithin, or condensation products of an aikylene oxide with fatty acids, for example polyoxyethylene stearate, or condensation products of ethylene oxide with long chain aliphatic alcohols, for example heptadecaethyleneoxycetanol, or condensation products of ethylene oxide with partial esters derived from fatty acids and a hexitoi such as polyoxyethylene sorbitol monooleate, or condensation products of ethylene oxide with partial esters derived from fatty acids and hexitoi anhydrides,
- Aqueous suspensions may also contain one or more preservatives, for example benzoates, such as ethyl, or n-propyl p- hydroxybenzoate, one or more colouring agents, one or more flavouring agents, and one or more sweetening agents, such as sucrose or saccharin.
- preservatives for example benzoates, such as ethyl, or n-propyl p- hydroxybenzoate, one or more colouring agents, one or more flavouring agents, and one or more sweetening agents, such as sucrose or saccharin.
- Dispersible powders and granules suitable for preparation of an aqueous suspension by the addition of water provide the active ingredient in admixture with a dispersing or wetting agent, suspending agent and one or more preservatives.
- a dispersing or wetting agent e.g., kaolin, kaolin, kaolin, kaolin, kaolin, kaolin, kaolin, kaolin, kaolin, kaolin, kaolin, kaolin, kaolin, kaolin, kaolin, kaolin, sorbitol, sorbitol, sorbitol, sorbitol, sorbitol, sorbitol, sorbitol, sorbitol, sorbitol, mannitol, mannitol, mannitol, mannitol, mannitol, mannitol, mannitol, mannitol, mannitol, mannitol,
- Syrups and elixirs may be formulated with sweetening agents, for example glycerol, propylene glycol, sorbitol or sucrose. Such formulations may also contain a demulcent, a preservative and flavouring and colouring agents.
- sweetening agents for example glycerol, propylene glycol, sorbitol or sucrose.
- Such formulations may also contain a demulcent, a preservative and flavouring and colouring agents.
- compositions may also be formulated as depot preparations. Such long acting formulations may be administered by implantation ⁇ eg, subcutaneously or intramuscularly) or by intramuscular injection.
- composition according to the invention may be formulated with suitable polymeric or hydrophobic materials (eg, as an emulsion in an acceptable oil or ion exchange resins, or as sparingly soluble derivatives, for example, as a sparingly soluble salt.
- compositions may also be in the form of a veterinar composition, which may be prepared, for example, by methods that are conventional in the art,.
- veterinary compositions include those adapted for:
- oral administration external application, for example drenches (e.g. aqueous or non-aqueous solutions or suspensions); tablets or boluses; powders, granules or pellets for admixture with feed stuffs; pastes for application to the tongue;
- drenches e.g. aqueous or non-aqueous solutions or suspensions
- tablets or boluses e.g. aqueous or non-aqueous solutions or suspensions
- pastes for application to the tongue for example drenches (e.g. aqueous or non-aqueous solutions or suspensions); tablets or boluses; powders, granules or pellets for admixture with feed stuffs; pastes for application to the tongue;
- parenteral administration for example by subcutaneous, intramuscular or intravenous injection, e.g. as a sterile solution or suspension; or (when appropriate) by intramammary injection where a suspension or solution is introduced in the udder via the teat;
- topical applications e.g. as a cream, ointment or spray applied to the skin;
- compositions of the composition While it is possible for each component of the composition to contact the tissue alone, it is preferable that the components of the composition be provided together with one or more pharmaceutically acceptable carriers.
- Each carrier must be pharmaceutically acceptable such that they are compatible with the components of the composition and not harmful to the subject.
- the pharmaceutical composition is prepared with liquid carriers, such as an ionic solution, for example NaCl or a buffer.
- a preferred pharmaceutically acceptable carrier is a buffer having a pH of about 6 to about 9, preferably about 7, more preferably about 7.4 and/or low concentrations of potassium.
- the composition has a total potassium concentration of up to about lOmM, more preferably about 2 to about 8 mi, most preferably about 4 to about 6mM.
- the composition according to the invention is hypertonic.
- the composition has a saline concentration greater than normal isontic saline which is 0.9% NaCl (0.154M).
- buffering compounds that exist in muscle that could be also used in a suitable ionic environment are ca nosine, hisfidine, anserine, ophidine and balenene, or their derivatives.
- magnesium may be used for cell, tissue or organ contact concentrations if desired without substanttally affecting the activity of the composition.
- body fluids e.g. blood or body cavity
- magnesium will undergo immediate dilution and substantially lower ceil, tissue or organ contact concentrations.
- th magnesium concentration in the composition may be as high as 2.0M (2000mM) prior to administration into the body. .
- typical buffers or carriers (as discussed above) in which the composition of the invention is administered typically contain calcium at concentrations of around 1 mM as the total absence of calcium has been found to be detrimental to the cell, tissue or organ, in one form, the invention may also include using carriers with low calcium (such as for example less than 0.5 mM) so as to decrease the amount of calcium within a cell in body tissue, which may otherwise build up during injury / trauma stunning.
- the calcium present is at a concentration of between 0.1 mM to 0.8 mM, more preferably about 0.3 mM.
- elevated magnesium and low calcium has been associated with protection during ischemia and reoxygenation of an organ. The action is believed to be due to decreased calcium loading.
- the pharmaceutically acceptable carrier is a bodily fluid such as blood or plasma, in another embodiment, the pharmaceutically acceptable carrier is crystalloid or blood substitute.
- composition useful in the methods according to the invention includes (i) a potassium channel opener or agonist and/or an adenosine receptor agonist; and (ii) an antiarrhythmic agent or a local anaesthetic and one or more of:
- antioxidant sodium hydrogen exchange inhibitor; antioxidant;
- a source of magnesium in an amount for increasing the amount of magnesium in a cell in body tissue
- a pharmaceutically acceptable carrier such as an ionic solution for example NaCI or a buffer.
- this composition has two, three or fou of the above components.
- Preferred additional components include one or more of an anti-inflammator agent, a metabolic fuel such as a citrate, source of magnesium and a pharmaceutically acceptable carrier such as a buffer, it is also contemplated that this composition may include more than one of the same component, for example two different potassium channel openers may be present in the composition. It is also contemplated that one component may have more than one function. For example, some calcium antagonists share effects with potassium channel openers.
- composition useful in the methods according to the invention further including an effective amount of elevated magnesium.
- the composition useful in the methods according to the invention includes adenosine and lidocaine.
- This composition may optionally include a metabolic fuel such as a citrate for example CPD.
- the composition according to the invention includes adenosine and lidocaine.
- This composition may optionally include an anti-inflammatory agent, such as beta-hydroxybutyrate,
- compositions according to the invention are a combination of adenosine and lidocaine.
- the composition may also include an anti-inflammatory agent, such as beta-hydroxybutyrate, and/or a metabolic fuel, such as a citrate for example CPD.
- the composition contains 0.1 to 40 mM of adenosine, 0.1 to 80 mM of lidocaine or a salt thereof such as a HCI salt, 0.1 to 2000 mM of a source of magnesium such as MgS0 > 0. to 20 mM of a citrate such as CPD and 0.9 to 3% of an ionic solution, such as a buffer or NaCI.
- compositions When the composition is used to increase blood pressure in a subject that has suffered a life threatening hypotension or shock; or to induce a low pain or analgesic state or a hypotensive state in a subject that has suffered a life threatening hypotension or shock; or to reduce hypofusion in the whole body of a subject, lower concentrations of magnesium are used, such as 30 mM or less than 20 mM.
- the method of the present invention involves contacting a tissue with the composition for a time and under conditions sufficient for reducing injury to the cell, tissue or organ.
- the composition may for example be infused or administered as a bolus intravenous, intracoronary or any other suitable delivery route as pre-treatment for protection during a cardiac intervention such as open heart surgery (on-pump and off-pump), angioplast (balloon and with stents or other vessel devices) and as with clot-busters (anti-clotting drug or agents).
- the composition may be administered intravenously or be administered both intravenously and intraperitoneaily or directly accessing a major artery such as the femoral artery or aorta in patients who have no pulse from massive exsanguination, or in the carotid artery or another artery during aortic dissection to protect the brain from hypoxia or ischemia.
- the composition may be administered intravenously and intraperitoneaily simultaneously, the perineum acting as, in effect, a reservoir of composition for the bloodstream as well as acting on organs in the vicinity with which it comes into contact.
- Anothe rapid route of administration is intraosseously (into the bone). This is particularly suitable for a trauma victim, such as one suffering shock.
- the composition contains two or more components, these may be administered separately but simultaneously. Substantially simultaneous delivery of the component to the target site is desirable. This may be achieved by pre-mixing the components for administration as one composition, but that is not essential
- the invention is directed towards the simultaneous increase in local concentration (for example an organ such as the heart) of the components of the composition.
- local concentration for example an organ such as the heart
- the invention may be practised by administering the composition using a perfusion pump, often associated with a procedure known as "miniplegia” or “microp!egia", in which minimal amount of components are titrated by means of a finely adjustable pump directly via a catheter.
- a protocol utilises miniplegia as described above, where micro amounts are titrated directly to the heart, using the patient's own oxygenated blood.
- the reference to a "setting" is a measure on the pump, such as a syringe pump, of the amount of substance being delivered directly to the organ, such as a heart.
- composition may be administered by aerosol.
- composition can also be infused or administered as a bolus intravenous, intracoronary or any other suitable delivery route for protection during cardiac intervention such as open heart surgery (on-pump and off-pump), angioplasty (balloon and with stents or other vessel devices) and as with clot-busters to protect and preserve the cells from injury.
- open heart surgery on-pump and off-pump
- angioplasty balloon and with stents or other vessel devices
- clot-busters to protect and preserve the cells from injury.
- the tissue may be contacted by delivering the composition intravenously to the tissue.
- the composition may be used for blood cardioplegia.
- the composition may be administered directly as a bolus by a puncture (eg, by syringe) directl to the tissue or organ, particularly useful when blood flow to a tissue or organ is limiting.
- the composition for arresting, protecting and preserving a tissue may also be administered as an aerosol, powder, solution or paste via oral, skin or nasal routes.
- composition may be administered directly to the tissue, organ or cell or to exposed parts of the internal body to reduce injury.
- composition according to the invention may be used with crystalloid cardioplegia to minimise injury to a tissue.
- a composition could be administered to provide localised arrest of the target tissue as well as protection during reperfusion and postconditiontng.
- composition may be delivered according to one of or a combination of the following deliver protocols: intermittent, continuous and one-shot. Accordingly, in another aspect of the invention, the composition may be administered as a single dose of the composition.
- the composition may be administered by intermittent administration.
- a suitable administration schedule is a 2 minute induction dose every 20 minutes throughout the arrest period. The actual time periods can be adjusted based on observations by one skilled in the art administering the composition, and the animal/human model selected.
- the invention a!so provides a method for intermittently administering a composition for reducing injury to the cell, tissue or organ.
- composition can of course also be used in continuous infusion with both normal and injured tissues or organs, such as heart tissue.
- Continuous infusion also includes static storage of the tissue, whereby the tissue is stored in a composition according to the invention, for example the tissue may be placed in a suitable container and immersed in a composition (or solution) for transporting donor tissues from a donor to recipient
- the composition according to the invention is administered in two steps (referred to as "one-two step iv infusion").
- the first administration is by bolus followed by drip infusion.
- the composition is administered in one shot as a bolus or in two steps as a bolus followed by infusion.
- the dose and time intervals for each deliver protocol may be designed accordingly.
- the components of the composition according to the invention may be combined prior to administration or administered substantially simultaneously or co- administered.
- composition may be administered by intravenous, intraosseous, intracardiac, intraperitoneal, spina! or cervical epidural.
- the composition useful in the methods according to the invention may be administered with or contain blood or blood products or artificial blood or oxygen binding molecules or solutions to improve the body's oxygen transport ability and survival b helping to reduce hypoxic and ischemic damage from blood loss.
- the oxygen-containing molecules, compounds or solutions may be selected from natural or artificial products.
- an artificial blood-based product is peril uorocarbon- based or other haemoglobin-based substitute.
- Some of the components may be added to mimic human blood's oxygen transport ability such HemopureTM, GelenpolTM, OxygentTM, and PolyHemeTM. Hemopore is based on a chemically stabilized bovine hemoglobin.
- Gelenpol is a polymerized hemoglobin which comprises synthetic water- soluble polymers and modified heme proteins.
- Oxygent is a perflubron emulsion for use as an intravenous oxygen carrier to temporarily substitute for red blood cells during surgery,
- Polyheme is a human hemoglobin-based solution for the treatment of life- threatening blood loss.
- oxygenation of the bod from a variety of ways including but not limited to oxygen gas mixture, biood, blood products or artificial blood or oxygen binding solutions maintains mitochondrial oxidation and this helps preserve the myocyte and endothelium of the organ. Without being bound by any particular mode or theory, the inventor has found that gentle bubbling with 95%Q 2 f % CO 2 helps maintains mitochondrial oxidation which helps preserve the myocyte and coronary vasculature.
- composition useful in the methods according to the invention is aerated with a source of oxygen before and/or during administration.
- the source of oxygen may be an oxygen gas mixture where oxygen is the predominant component.
- the method according to the invention includes:
- nutrient molecules selected from the group consisting of blood, blood products, artificial blood and a source of oxygen;
- compositions optionally aerating the composition with the oxygen (for example, in the case of isolated organs) or combining the nutrient molecules with the composition, or both; and placing the tissue, cell or organ in contact with the combined composition under conditions sufficient to reduce injury.
- oxygen for example, in the case of isolated organs
- nutrient molecules for example, in the case of isolated organs
- This method may include the further step of postconditioning the cell, tissue or organ.
- the oxygen source is an oxygen gas mixture.
- oxygen is the predominant component.
- the oxygen may be mixed with, for example CG 2 . More preferably, the oxygen gas mixture is 95% 0 2 and 5% C0 2 -
- composition useful in the methods of the invention is highly beneficial at about 10°C but can also be used to prevent injury over a wider temperature range u to about 37°C. Accordingly, the composition may be administered to the cell, tissues or organs at a temperature range selected from one of the following: from about OX to about 5°C, from about 5°C to about 20°C, from about 20°C to about 32°G and from about 32°C to about 38 . It is understood that “profound hypothermia” is used to describe a tissue at a temperature from about 0°C to about 5°C. "Moderate hypothermia” is used to describe a tissue at a temperature from about 5°C to about 20°C.
- Normal hypothermia is used to describe a tissue at a temperature from about 2CTC to about 32 a C
- Normal body temperature is used to describe a tissue at a temperature from about 32 C to about 38°0, though the normal body temperature is around 37 to 38°C.
- compositions would also find use as a topical spray or soaked in a gauze soaked and applied to an organ, tissue or cell of the body and has application for surgery and clinical interventions.
- This applicatio may include a topical aerosol for spraying on surgical incisions or wounds, and around the area of these wounds.
- the composition could be used for applying to a median sternotomy (sternal incision) in cardiac surgery, and applied during and after the operation to reduce or prevent adhesions from occurring between the underside of sternum area to the underlying heart and other tissues after the operation.
- sternal incision median sternotomy
- the composition cou!d be applied to the internal organs during and prior to closing the incision to reduce or prevent adhesions from occurring in the abdominal cavity after surgery.
- the composition could also be used for incisions made for artery or venous catheterizations.
- the area could be sprayed or soaked and the surgical well with the composition to prevent adhesions from occurring after the incision is closed.
- Another application would be for harvesting veins or arteries to be used for cardiac surgery as conduits to replace the blocked arteries on the heart in a coronary artery bypass operation.
- composition 15 saphenous vein is exposed from a long incision in the leg and harvested for cardiac surgery, and the area could be sprayed or topically applied on a gauze.
- the composition would also have an application for less invasive endoscopic harvesting of blood vessels. Topical applications of the composition would also find applications on areas of the heart itself particularly where potential cell fibrosis or injury ma occur
- the whole heart could also be sprayed topically to protect it from any adhesions or dysfunction.
- the amount of active ingredients present in the 25 composition will depend on the nature of the subject (whole body, isolated organ circuit in the body or isolated cell, organ or tissue ex vivo) and the proposed method of treatment or use. The amount should be effective for the end use, for example, one or more of the components should be present "in an amount sufficient to increase blood pressure".
- IV, IA, Arrest preferr preferr 4 blood A, 1 mg L, 50
- IO or IC ed ed ed mM 1 5% or mg M, 1 mg/kg mM
- Rat 1 ml/kg/hr
- Isolated human brain circuit perfusion via a cerebral ml/kg/hr artery such as carotid
- aortic, endarterectorny or other brain Brain Circuit protection surgery and interventions; 1 to 100 ml/kg/min 10-30 mf/kg/min
- Cardiac perfusion 1 to 500 mi/mirt (0.01 to 10 ml min/kg human) Arrest: flow 4-7 ml/kg/min (A; 1.4 mg/kg; L: 2.9 mg/kg;
- Lung injury may higher A: 12
- 3% NaCi may be used if brain injury suspected
- Infusio 1 to 40 1 to 1 to 50 0.01 to 0 m!/kg/ rwith n-Drip preferr 80 preferr 5
- A 12 mg/kg; ed preferr ed mg/kg/m L;24 mg/kg; ed in :12 mg/kg or more hypotension
- A 18 mg/kg; L:36 mg/ kg; :20 mg/kg
- the concentrations of each component in the composition may be diluted by body fluids or other fluids that may be administered together with the composition.
- the composition will be administered such that the concentration of each component in the composition contacts the tissue about 100- fold less.
- containers such as vials that house the composition may be diluted 1 to 100 parts of blood, plasma, crystalloid or blood substitute for administration.
- Fig, 1 shows graphs showing measurement of (A) Heart Rate; (B) MAP; (C) Systolic Pressure; (D) Diastolic Pressure; (E) Temperature against Time (min) in Rat Polymicrobial Bacterial Infection Model: Single Bolus Intravenous Treatment only for Rat AIM Bolus v's Control.
- Fig. 2 shows graphs showing measurement of (A) Heart Rate; (B) MAP; (C) Systolic Pressure; .(D) Diastolic Pressure; (E) Temperature against Time (min) in Rat Polymicrobial Bacterial Infection Model: One-Two Intravenous Treatment Delivery over 5 hours for Rat ALM Bolus v's Control, (see example 1)
- Fig 3 shows a graph comparing TNF-Alpha versus ALM infusion dose.
- the X-axis refers to the dose of adenosine (A) in the ALM dose with the following combinations being tested: 1) Control animal TNF-alpha with LPS alone infusion; 2) 5 pg A/10 pg Lidocaine/ 5.6 pg MgS0 4 /kg/min; 3)10 pg A/20 pg Lidocaine/ 5.6 pg MgS0 4 /kg/min; 4) 300 pg A/600 pg Lidocaine/ 336 pg MgSGykg/rnin. (see example 2)
- Fig 4 shows a flow diagram of videomicroscopy procedure described in Example 4.
- Fig 5 shows graphs measuring the effect of Adenosine (A), lidocaine (L) and adenosine and lidocaine (AL) on % relaxation (Y axis) of isolated guinea-pig mesenteric artery when added in the lumen (luminal - square) or in the bathing solution (abluminai - diamond).
- Fig ⁇ shows graphs measuring the effect of Adenosine (A), lidocaine (L) and adenosine and lidocaine (AL) on % relaxation (Y axis) of isolated guinea-pig mesenteric artery when intact (square) or denuded (endothelium removed) (diamond)
- Fig 7 shows ROTEM traces for the different groups asphyxia! cardiac hypoxia and arrest (AB), 0.9% NaCI at 120 min (CD), 0.9% NaCI ALM at 120 min (EF), and in four controls that failed to achieve return of spontaneous circulation (ROSC) (GH). (See example 5)
- Fig 9 shows a Graph showing MAP resuscitation following single 3% NaCI ALM single bolus (Group 1); bolus alone compared to one-two-step (bolus-infusion) for MA and heart rate (Grou 2); and bolus-boius (Group 3). (See example 7)
- Fig 10 shows a graph showing the effect of addition of valproic acid
- Fig 11 shows a graph showing MAP resuscitation following single NaCI ALM bolus in the presence of L-NAME.
- Fig 12 shows ECG traces (A, C, D, E, F, H, I, J, M, O and Q) and b!ood pressure traces (6, G, K, L, N, P) showing the effect of ALSVt with a genera! anaesthetic from a normal state to whole body arrest.
- Fig 13 shows ECG traces A and B demonstrating the effect of hemodynamic stabilization with adenosine agonist plus fidocaine and magnesium after extreme blood loss.
- Fig. 14 shows graphs showing the effect of adenosine and lidocaine solution with different forms of citrate (citrate phosphate dextrose CPD and sodium citrate) and elevated magnesium.
- Graphs showing measurement of (A) heart aortic flow; (8) heart coronary flow; and (C) heart rate against 60 min of reperfusion time after 2 hours tepid arrest (heart temperature ⁇ 29°C) in the isolated working rat heart. Hearts were flushed with normothermic cardioplegia every 18 min for 2 minutes (n ⁇ 8 each group) (see example 1)
- Fig. 15 shows graphs showing the effect of adenosine and lidocaine solution with different forms of citrate (citrate phosphate dextrose CPD and sodium citrate) and elevated magnesium.
- Fig 16 shows graphs showing the effect of 8 hours of cold (4 C C) continuous perfusion of adenosine and lidocaine solution with and without gentle bubbling (95% Oa/5% CO 2 ) on functional recovery in the isolated working rat heart
- Fig 17 shows graphs showing the effect of adding insulin and melatonin wit high and low MgSCu to bubbled adenosine and lidocaine solution during 8 hours of constant perfusion at 4°C in the isolated working rat heart.
- Fig 18 shows graphs showing the effect of adenosine and lidocaine solution with sildenafil citrate over 2 hours warm arrest (2£TC) given every 20 minutes (2 min infusion) and 60 min reperfusion.
- Fig 19 shows ECG and blood pressure traces before and after inducing hypotensive anesthesia using AL -CPD (A and B before, C and D after) and ECG and blood pressure traces before and after inducing whole body arrest using AL -CPD (E and F before, J-L after).
- Fig 20 shows graphs of the results of the experiments described in Example 46.
- Fig 21 shows graphs of the results of the experiments described in Example 46.
- Fig 22 shows graphs of the results of the experiments described in Example 46.
- Fig 23 shows graphs of the results of the experiments described in Example 46.
- Fig 24 shows graphs of the results of the experiments described in Example 46.
- Fig 25 shows graphs of the results of the experiments described in Example 46.
- Fig 26 shows a schematic diagram of the experimental protocol for Example 47.
- Fig 2? shows graphs showing the effect of treatment with adenosine, lidocaine, and g2+ (ALMJ adenosine and lidocaine (AL) on mean arterial pressure (MAP) (A) and heart rate (HR) (B).
- MAP mean arterial pressure
- HR heart rate
- Fig 28 shows graphs showing cardiac index (A), stroke volume (B), ejection time (C), and oxygen consumption (Vo 2 ) (D) during both hypotensive resuscitation and after infusion blood.
- Fig 29 shows graphs showing cardiac function data during the experiment Left ventricular (LV) end-systolic pressure (A) and LV end-diastolic pressure (B) measured throughout the course of the experiment.
- LV left ventricular
- A left ventricular
- B LV end-diastolic pressure
- C The maximum positive deveiopment of ventricular pressure over time (dP/dtmax) as a marker of cardiac systolic function.
- D The maximum negative development of ventricular pressure over time (dP/dtmtn) as a marker of cardiac diastolic function.
- Fig 30 shows graphs showing the renal variables urine output, plasma creatinine, urine protein to creatinine, and urine n-acetyl- ⁇ -d-glucosaminide (NAG) to creatinine ratio throughout the course of the experiment.
- A Urine output measured after 90 min of hemorrhagic shock and then every hour during the remainder of the experiment.
- B Plasma creatinine as a marker of global kidney function.
- C Urine protein to urinary creatinine ratio as a marker of glomerular injury.
- D Urine NAG to urinary creatinine ratio as a marker of proximal tubular injury. Data presented as median ⁇ 95% CI),
- Fig 31 shows a schematic representation of the in vivo rat protocol of severe polymicrobial sepsis.
- Fig 32 shows a table showing the effect of 0.9% NaCI AL on hemodynamics and recta! temperature during 5 Hours following CLP in a rat model of severe sepsis
- Fig 33 shows graphs showing the effect of 0.9% NaCI ALM on the MAP (A) and without the effect of shams (B); SAP (C) and without th effect of shams (D) during 5 hours of CLP in a rat model of polymicrobial sepsis.
- Fig 34 shows graphs showing the effect of 0.9% NaCI ALM treatment on HR (A) and without the effect of shams (B). Rectal temperature (C) and without the effect of shams (D) during 5 hours of CLP in a rat model of polymicrobial sepsis.
- PT A
- aPTT BJ
- representative photographs C of gross pathophysiologic examinations of the cecum in the shams, saline controls, and ALM-treated rats after 5 hours.
- Example 1 One-two IV injection administration protocol of AL
- the cecal ligation and puncture model is considered the gold standard for sepsis research.
- toll receptor agonists such as lipopo!ysaccharide (LPS) toxin model which is only detectible in only a minority of patients with sepsis
- LPS lipopo!ysaccharide
- the cecal ligation model mimics the human disease of ruptured appendicitis or perforated diverticulitis.
- the cecal model also reproduces the dynamic changes in the cardiovascular system seen in humans with sepsis. In addition, the model recreates the progressive release of pro-inflammatory mediators.
- the gastrointestinal tract often can be damaged directly from penetrating or blunt trauma, but also from ischemic injury from any kind of major surgery, cardiac arrest, bums, haemorrhage and shock.
- Ischemic injury poses a significant risk of infection and sepsis because the gut wall becomes leaky and bacteria translocates into the peritoneal cavity resulting in a medical emergency.
- Reducing the impact of infection from Gl injury would also reduce adhesions as infection is one cause of adhesions as the body attempts to repair itself.
- Adhesions may appear as thin sheets of tissue similar to plastic wrap, or as thick fibrous bands. Up to 93 per cent of people who have abdominal surgery go on to develop adhesions.
- mice Male Sprague Dawley rats (300-450 g) were fed ad libitum with free access to water and housed in a 12-hr light-dark cycle. Animals were not heparinized and anesthetized with an intraperitoneal injection of 100 mg/kg sodium thiopentone (Thiobarb). Anesthetized animals were positioned in the supine position on a custom designed cradle. A tracheotomy was performed and animals were artificiaiiy ventilated (95-100 strokes min ' ) on humidified room air using a Harvard Small Animal Ventilator (Harvard Apparatus, Mass., USA).
- a rectal probe was inserted 5.0 cm and the temperature ranged between 37 and 34 °C.
- the caecum was isolated through midline laparotomy and ligated below ileocaecal valve. It was punctured with 18G needle four times through-and-th rough (8 holes).
- the abdominal cavity was surgically closed in 2 layers. Rats were randomly assigned into either control or groups for Example 1 (bolus only) and Example 2 (bolus plus drip infusion).
- Example 1a One-bolus of ALM is insufficient to support hemodynamics
- Example 1a Control animals receive intravenous 0.3 ml bolus 0.9% NaCI and treatment groups was 0.3 ml bolus 0.9% NaC! with 1 miVS Adenosine (0.24 mg/kg), 3 m Lidocaine (0.73 mg/kg), and 2.5 mM IVigSO* (0.27 mg/kg), in 0.9% NaCI.
- ALM bolus stabilized the cardiovascular system for about 60 min then failed to protect against collapse and SEPTIC SHOCK over 5 hours of polymicrobial infection.
- Example 1b One bolus plus drip infusion (One-Two IV injection strategy) showed hemodynamic support and avoidance of septic shock.
- Control animals receive intravenous 0,3 mi bolus 0,9% NaCI and drip infusion (0,4 ml/hr) 0,9% NaCI.
- Treatment animals received 0.3 ml bolus 0.9% NaCI with 1 m Adenosine (0.24 mg/kg) confront 3 mM Lidoeaine (0.73 mg/kg, and 2.5 mM MgS0 4 (0.27 mg/kg), and a different composition for drip infusion (0.4 ml/hr) comprising 12 mg kg/hr Adenosine, 34 mg/kg/hr Lidoeaine, and 13.44 mg/kg hr MgS0 in 0.9% NaCI
- the control and treatment was withdrawn after 4 hr and animals monitored for further 60 min.
- Figure 2 show that ALM !V bolus infusion one-two treatment strategy stabilizes the cardiovascular system and preserves body temperature regulation during 5 hours of polymicrobial infection (sepsis).
- This hyperdynamic phase (90-225 min) in controls is well known and due to increased sympathetic activity and stress as a result of the infection.
- ALM stability implies improved heart rate variability improved central nervous system control of heart rate.
- ALM treatment also improves body temperature control and begin to increase body temperature after 150 min. This is significant as it implies improved central nervous function during 5 hour of infection compared to controls which wen into septic shock * ALM bolus and intravenous infusion prevented animal from cardiovascular collapse and avoided SEPTIC SHOCK over 5 hours of polymicrobial infection.
- Example 2 Effect of dose response of ALM infusion to reduce inflammation (Tumor necrosis Factor -alpha, TNF-alpha) during Endotoxemia in the Pig
- TNF alpha is a cytokine involved in systemic inflammation, and along with other cytokines stimulates the acute phase reaction to stress and infection. TNF-alpha also induces activation of coagulation in different pathological states including sepsis.
- Activated protein C inhibits TNF-alpha production.
- Activated protein C (and antithrombin) may inhibit the endothelial perturbation induced by cytokines.
- Antithrombin regulates TNF-alpha induced tissue factor expression on endothelial cells by an unknown mechanism.
- Activated protein C and antithrombin, and their pathways of regulation may be useful targets for treating coagulation abnormalities associated with sepsis or other inflammation diseases. These sites and pathways inhibit not only coagulation but also involved with the downregulation of anticoagulant activities of endothelial cells.
- a dose response of ALM infusion on inflammation was studied in the swine model of lipopolysaccharide (LPS, an obligatory component of Gram-negative bacterial ceil wads) endotoxemia at 90 min infusion (Infusion of LPS for 5 hours 1 pg/kg/min) into 40 kg female pigs. Pigs were fasted overnight, but allowed free access to water. Anesthesia was induced with midazolam (20 mg) and s-ketamin (25Gmg) and maintained with a continuous infusion of fentanyl (60 pg/kg/h) and midazolam (6 mg/kg/h).
- LPS lipopolysaccharide
- the animals were intubated and volume-controlled ventilated (S/5 Avance, Datex Ohmeda, Wi, USA) with a positive end- expiratory pressure of 5cm H s O, Fi02 of 0.35. and a tidal volume of 10 ml/kg. Ventilation rate was adjusted to maintain PaCC1 ⁇ 2 between 41-45 rnmHg. The body temperature was maintained around 38°C during the entire study. All animals received normal saline (NS) at a maintenance rate of 10ml/kg/ during surgery and the baseline period and was increased to 15ml/kg/h during LPS infusion.
- NS normal saline
- the results are shown in FIG 3.
- the Y-axis is TnF-alpha in plasma produced at 90 min in response to the LPS infusion and the X-axis refers to the dose of adenosine (A) in the different ALM doses with the following combinations being tested:
- the stock composition for infusion was 0.15 mM Adenosine, 0.296 mM lidocaine and 0.187 mM MgS0 4 4) 300 pg A/600 pg Iidocaine/ 336 ug MgSQ ⁇ kg/min over a 4 hour period or 18 mg Adenosine per kg/hour, 36 mg/kg/hour Iidocaine and 20 mg MgS0 4 /kg/hr.
- the stock composition for infusion was 4.5 mM Adenosine, 8.88 m Iidocaine and 11 m gSCv
- TNF alpha is a cytokine involved in systemic inflammation, and along with other cytokines stimulates the acute phase reaction to stress and infection. TNF-alpha also induces activation of coagulation in different pathological states including sepsis.
- the present invention by inhibiting TnF alpha may reduce inflammation and reduce the impact inflammation has on coagulation during infection, sepsis and septic shock. Since adhesions can be caused by infection, the present invention also may reduce the incidence of adhesions.
- the present invention since inflammation is part of any injury process (traumatic or non-traumatic) particularly as a result of traumatic brain injury, the present invention also may reduce the secondary complications of brain injury. Since inflammation is a result of disease (heart attack, stroke, cardiac arrest, auto-immune diseases, hemorrhagic shock), the present invention also may reduce the complications of disease due to local or systemic inflammation. There is a major unmet need to reduce the impact of infection in health and disease, and to modulate the immune function of the host to reduce the impact of infection or prevent it from progressing into septic shock.
- Sepsis is a very common complication of almost any infectious disease.
- severe sepsis and septic shock remain an unmet medical need.
- new drugs that modulate the immune function of the host to reduce the impact of infection or prevent it from progressing into septic shock.
- Drugs can be divided into three categories according to their mechanism of action: i) agents that block bacterial products and inflammatory mediators, ii) modulators of immune function, and Hi) immunostimulation (reduce immunosuppression). Drug development could also have an impact on many pathologies involving lo levels of inflammatory markets and immune imbalances. For example, recent studies suggest that acute and chronic cardiovascular disease is associated with a chronic low-grade inflammation that promotes adverse ventricular remodeling and correlates with disease progression. Several inflammatory mediators, .including TNF-. ⁇ , IL- 1 ⁇ , and IL-6, are involved in cardiac injury subsequent to myocardial ischemia and reperfusion, sepsis, viral myocarditis, and transplant rejection.
- Example 3 Coagulopathy changes in the Rat Polymicrobial Bacterial Infection Model during One-Two Intravenous ALM Treatment Delivery over 5 hours
- Severe sepsis defined as sepsis associated with acute organ failure, is a serious disease with a mortality rate of 30-50%. Sepsis always leads to deranged coagulation, ranging from mild alterations up to severe disseminated intravascular coagulation (DIG) (hypercoagulopathy). Septic patients with severe DIG have microvascular fibrin deposition, which often leads to multiple organ failure and death. Alternatively, in sepsis severe bleeding might be the leading symptom (hypocoagulopathy), or even coexisting bleeding and thrombosis. There are no approved drugs for sepsis and currently constitutes a major unmet medical need requiring breakthrough technologies. The deranged coagulation, particularly DIG, Is an important and independent predictor of mortality in patients with severe sepsis.
- the rat model used as an example below is a gold standard to mimic the pathophysiology of severe sepsis in humans.
- mice Male Sprague Dawley rats (300-450 g) were fed ad libitum with free access to water and housed in a 12-hr light-dark cycle. Animals were not heparinized and anesthetized with an intraperitoneal injection of 100 mg/kg sodium thiopentone (Thiobarb). Anesthetized animals were positioned in the supine position on a custom designed cradle. A tracheotomy was performed and animals were artificially ventilated (95-100 strokes min-1) on humidified room air using a Harvard Small Animal Ventilator (Harvard Apparatus, Mass., USA), A rectal probe was inserted 5.0 cm and the temperature ranged between 37 and 34 °C.
- the caecum was isolated through midline laparotomy and ligated below i!eocaecal valve. It was punctured with 18G needle four times through-and-th rough (8 holes). The abdominal cavity was surgically closed in 2 layers. Rats were randomly assigned into either control or groups for ALM Bolus and Infusion.
- Control animals receive intravenous 0.3 ml bolus 0.9% NaCI and dri infusion (0.4 mi/hr) 0.9% NaCI, Treatment animais received 0,3 ml bolus 0.9% NaCI with 1 mM Adenosine (0.24 mg/kg), 3 mM Lidocaine-HCi (0.73 mg/kg, and 2.5 mM MgS0 4 (0.27 mg/kg, and a different composition for drip infusion ⁇ 0.4 m!/hr) comprising 12 mg/kg/hr Adenosine, 34 mg/kg/hr Lidocaine, and 13.44 mg/kg/hr MgS0 4 in 0.9% NaCI
- control and treatment was withdrawn after 4 hr and animais monitored for further
- PT prothrombin times (extrinsic clotting pathway begins with tissue factor and believed to be the initiator of clotting in vivo)
- aPTT activated partial thromboplastin time in contrast to the PT, measures the activity of the intrinsic and common pathways of coagulation.
- the term 'thromboplastin' in this test refers to the formation of a complex formed from various plasma clotting factors which converts prothrom in to thrombin and the subsequent formation of the fibrin clot.
- Example 4 AL Relaxation of the mesenteric artery and increase blood flow to the GI tract to reduce injury or damage to the gut, reduce infection and reduce adhesions
- composition according to the invention to relax the mesenteric artery and potentially increase blood flow to the gastrointestinal tract.
- Adenosine, lidocaine or adenostne-iidocain together were administered 2) luminally and 2) abiuminally and concentration curves were obtained.
- Stock solutions of adenosine and lidocaine alone or adenosine-iidocaine combined were made in de ionized water to 20 mM.
- a range of volumes were pipetted to provide contact concentrations with the vessel lumen or outer wall that ranged from 0.001 to 1 mM.
- arteries were dilated using calcium-free solution to obtain 100% relaxation.
- a number of arteries were denuded by introducing 5 ml air into the lumen with flow rate 1000 ⁇ /min. The air outflow was then clamped until the intraluminal pressure reached 70 mmHg, flow rate was reduced to 2 ⁇ /min and the vessel remained pressurized for 10 minutes
- Example 4a Effect of Adenosine(A), iidocaine ⁇ L) and adenosine and lidocaine (AL) on relaxation of isolated guinea-pig mesenteric arter when added in the lumen (luminal) or in the bathing solution (ab!uminal).
- Fig. 5A shows that adenosine increased relaxation of the isolated intact mesenteric artery in a dose dependent manner, and that at 10 ⁇ and 100 ⁇ the effect of adenosine added to the bathing solution surrounding the vessel (abluminal administration) produced significantly more relaxation than if the solution was perfused through the lumen (inside the vessel).
- Fig. 5B Shows that lidocaine failed to produce relaxation in the isolated intact mesenteric artery and there was no significant difference if the lidocaine was in the lumen or on the outside bathing solution.
- Fig 5C shows that adenosine-iidocaine together increased relaxation of the isolated intact mesenteric artery in a dose dependent manner. In contrast to adenosine alone (Fig 5A) the greater relaxation from abluminal administration was not significantly different over the range of AL studied.
- Example 4b The effect of Adenosine, lidocaine and adenosine and lidocaine on relaxation of the mesenteric artery with or without an intact endothelium.
- Example S Coagulopathy after Asphyxiai-hypoxia induced Cardiac Arrest with Sepsis-like Syndrome
- This example tests the effect of 0.9% NaCl AL on correcting hypocoagulopathy (or reducing bleeding) and reducing blood clot retraction (strengthening the clot from breaking down) after asphyxial cardiac arrest with "sepsis-like" cardiac syndrome.
- Post-cardiac arrest recovery is characterized by high levels of circulating cytokines and adhesion molecules, the presence of plasma endotoxin, and dysregulated leukocyte production of cytokines: a profile similar to that seen in severe sepsis. Coagulation abnormalities occur consistently after successful resuscitation, and their severity is associated with mortality,
- a 0.5 ml bolus ALM contained 1.8 m Adenosine, 3.7 m Lidocaine-HCI and 4.0 mWI MgS ⁇ 3 ⁇ 4. In the 0.5 ml there were 0.48 mg adenosine, 1.0 mg lidocaine-HC! and 2.4 mg MgS0 . This was also equivalent to a bolus of 1.44 mg/kg adenosine, 3.0 mg/kg iidocaine-HCI and 7.2 mg/kg MgSO*.
- ROTEM (Tern International, Kunststoff, Germany) provides a real-time evaluation of the viscoelastic properties of whole blood in health and disease. Parameters include time to initiation of the clot, early clot formation kinetics, clot firmness and prolongation, clot fibrin- platelet interactions and clot lysis. Venous whole blood was obtained at baseline, following cardiac arrest, and at 120 min following ROSC or in those animals that failed to attain ROSC in the first 2 to 5 min of attempts. A volume of 1.8 ml blood was drawn into a 2.0 ml BD vacutainer containing citrate-phosphate-dextrose solution .
- EXTEM, INTEM and FIBTEM viscoelastic analysis was performed within 30 minute of blood withdrawal.
- the EXTEM test is extrinsicaily activated by thromboplastin (tissue factor) whereas INTEM test is activated by the contact phase (as in aPTT).
- FIBTEM is activated as in EXTEM with the addition of cytochalasin D, which inhibits platelet glycoprotein (GP) ll /ll!a receptors.
- GP platelet glycoprotein
- Clotting time or the time from start of measurement until a clot amplitude of 2 mm
- CFT clot formation time
- MCF maximum clot firmness
- the alpha angle (a) was also measured and represents the angle between baseline and a tangent at the maximum clot slope and clot amplitude (amplitude at 5 to 30 min) in mm over a 30 min period.
- the lysis index (LI, %) was estimated as the ratio of clot firmness (amplitude at 30 or 60 min) divided by MCF times 100.
- Prothrombin Time (PT) and Activated Partial Thromboplastin Time (aPTT) The blood remaining from ROTEM analysis was centrifuged at room temperature and the plasma removed, snap frozen in liquid nitrogen, and stored at -80°C until use. PT and aPTT were measured using a coagulometer (Trinity Biotech, Ireland) as described by Letson and colleague. These standard plasma coagulation tests reflect the kinetics of first fibrin formation with no information from platelet contributions.
- the PT is a measure of the integrity of the extrinsic and final common pathways analogous to EXTEM CT (CFT).
- the aPTT is a measure of the integrity of the intrinsic and final common pathways analogous to I NT EM CT (CFT)
- Table 2 below provides a summary of the Major Coagulation Changes over 2 hours of sustained return of spontaneous circulation (ROSC) in the rat model of 8 min asphyxia! cardiac hypoxia and arrest.
- ROSC spontaneous circulation
- Table 2 Major Coagulation Changes over 2 hours of sustained return of spontaneous circulation (ROSC) in the rat model of 8 min asphyxial cardiac hypoxia and arrest.
- ROSC spontaneous circulation
- Figure 7 shows representative ROTEM traces for the different groups asphyxial cardiac hypoxia and arrest (AB), Q.9% NaCI at 120 min (CD), 0.9% NaCI. AL at 120 min (EF), and in four controls that failed to achieve ROSC (GH).
- ALM administration prevents clot retraction (prevents a decrease in clot amplitude) thus making it a stronger clot to reduce bleeding
- ALM's ability to correct clot strength (amplitudes) may be significant because point-of-care low clot strength is an independent predictor of massive transfusion, and coagulation-related mortality within 15 min following the resuscitation of trauma patients.
- reduced or weak clot strength before hospital admission has been shown to be independently associated with increased 30-day mortality in trauma patients.
- ALM fully corrected clot strength, maximum clot elasticity (MCE) and CE piat ei e t (P ⁇ 0.05) (Table 2) compared to saline controls implies that ALM provides more favorable conditions for a stronger, denser fibrin network with higher elastic modulus (Table 1 ) and possibly higher thrombin concentrations compared with saline control.
- ALM appears to alleviate the sepsis-like changes in clot abnormalities after asphyxial cardiac hypoxia and arrest.
- Example 6a LM with general anesthetic whole body arrest (from NORMAL STATE)
- the left femoral vein and artery was cannulated using PE-50 tubing for drug infusions and biood pressure monitoring (UFI 1050 BP coupled to a MaeLab) and the right femoral artery was cannulated for bleeding.
- Lead I! electrocardiogram (ECG) leads were implanted subcutaneously on the left and right front legs and grounded to the back leg. The chest was opened and the heart was exposed to observe the effect the treatment in addition to the hemodynamic and ECG measurements. Rats were stabilized for 10 minutes prior to whole body arrest.
- Estimated blood volume of 650 g rat is -39.47 ml. The animal was not bled or in shock.
- concentrations of the actives in imM are 3.75 mM Adenosine, 7.38 m lidocaine-HCI, 833 mM MgS0 4 and 3.71 mM propofol.
- the composition When expressed in mg/kg animal the composition includes 1.5 mg/kg adenosine, 3 mg/kg lidocaine-HCI and 125 mg/kg MgS0 4 and 1 mg/kg propofol.
- the rat After an intravenous bolus of ALM/propofol the rat underwent circulatory collapse within 10 sec. The blood pressure fell to zero and the heart rate fell to zero. The heart rate returned after -4 min. Began chest compressions at 6 min for 2 min on!y then again at 15 min and pressure increased. Within 10 min the hemodynamics returned to normal. The animal was monitored for 2 hours and hemodynamics were stable and following the experiment an autopsy showed no signs of ischemia to the heart, lungs, kidneys or gastrointestinal tract.
- ECG acceleratory 'blips' see Figures 12C and 12D. More regular pattern started at 1 min 40 sec (HR -35 bpm). Still coordinated transient pressure increase (trace not shown). During this time period noticed paws twitching and twitching in abdominal region
- Example 6b Effect of whole body arrest with ALM and Thiobarb
- Rectal temperature was monitored using a rectal probe inserted 5 cm from the recta! orifice before, during and following shock and resuscitation, and previous experiments show the temperature ranges between 37 to 34 'C.
- the left femoral vein and artery was cannulated using PE-50 tubing for drug infusions and blood pressure monitoring (UFI 1050 BP coupled to a MacLab) and the right femoral artery was cannulated for bleeding.
- Lead II electrocardiogram (ECG) leads were implanted subcutaneously on the teft and right front legs and grounded to the back leg. Rats were stabilized for 10 minutes prior to b!ood withdrawal.
- Hemorrhagic shock was induced by withdrawing blood from the femoral artery at an initial rate of ⁇ 1 ml/min then decreasing to -0.4 ml/min over 20 min. Initially blood was withdrawn slowly into a 10 ml heparinized syringe (0.2 ml of 1000 U/ml heparin) to reduce MAP to between 35 and 40 mmHg. If MAP increased, more blood was withdrawn to maintain its lo value, and the process was continued ove a 20 min period. The Thiobarb animal was left in shock for 60 min with frequent checking to ensure the MAP remains between 35 to 40 mmHg. After 60 min shock the animal was injected with an IV 0.5 ml bolus of hypertonic saline with ALM.
- total volume injected IV was 0.5 mi made up to 7,5% Nad.
- concentrations i mM in 0.5 ml bolus were 1.5 mM adenosine, 1.48 mM fidocaine-HCI and 333 mM MgS0 4 , and 1270 mM NaGi.
- the composition actives in mg/kg ar 0.6 mg/kg adenosine, 0.6 mg/kg lidocaine-HCI, 80 mg kg Mg 0 and 114 mg/kg NaC! and Thiobarb was 100 mg/kg.
- Example 6a A single 0.5 ml bolus resulted in a collapse in blood pressure but not heart rate. Having a heart rate and no pressure development is termed pulseless electrical activity (PEA) or electromechanical dissociation. After 1 min 50 sec, there were electrical amplitude spikes in voltage and these occurred after every 7 seconds, and within 20 seconds the blood pressure rose and after 2 min 30 sec the pressure was surprisingly 1.7 times higher than when the treatment was first administered.
- PDA pulseless electrical activity
- NTS brainstem nucleus tractus solitaris
- Example 6b differs from Example 6a because in heart rate fell to zero after treatment in Example 6a.
- Heart rate variability is the physiological phenomenon of variation in the time interval between heartbeats. Heart rate and rhythm are largely under the control of the autonomic nervous system whereb the barorefiex continually adjusts heart rate to blood pressure via changes in vagal (parasympathetic) activity. In this way the arterial barorefie also affects arrhythmogenests and whole body hemodynamic stability. Thus sympathetic activation can trigger malignant arrhythmias, whereas vagal activity may exert a protective effect. Barorefiex sensitivity is quantified in ms of RR interval prolongation for each mmHg of arterial pressure increase. In the analysis of HR variability, there is a time domain and a frequency domain of analysis,
- Time Domain The time domain measures of HR variability as calculated by statistical analyses (means and variance) from the lengths of successive R-R intervals in the ECG and considered reliable indices of cardiac parasympathetic activity.
- the time domain indices include SDNN, SADNN, NN50, pNNSO, RMSSD, SDSD.
- SDNN standard deviation of the average R-R intervals
- SADNN standard deviation of the average R-R intervals
- the SDN mostly reflects the very- low-frequency fluctuation in heart rate behavior).
- NN50 is the number of pairs of successive beat to beat (NN) that differ by more than 50 ms or when expressed as a percentage (pNNSO),
- the RMSSD is the square root of the mean squared differences of successive R-R intervals
- the SDSD is the standard deviation of successive differences of R-R intervals.
- Frequency Domain Frequency domain analysis is traditionally understood to indicate the direction and magnitude of sympatho-vagal balance of heart rate variability. It is obtained by dividing the heart rate signal into its low and high frequency bands and analyze the bands in terms of their relative intensities (power).
- the LF or low frequency band (0.04 to 0.15 Hz) is involved with oscillations related to regulation of blood pressure and vasomotor tone.
- the HF or high frequency band (0.15 to 0,4 Hz) reflects the effects of respiration on heart rate (i.e. in respiratory frequency range).
- the LF band reflects primarily sympathetic tone
- the HF band reflects parasympathetic tone
- the ratio LF/HF is viewed as an index of sympatho-vagal balance.
- the LF/HF ratio is much more complex than originally thought and it appears to be restricted to the estimation of parasympathetic influences on heart rate.
- An increase or decrease in the LF/HF ratio appears to reflect more on the different dominating parasympathetic oscillation inputs that determine blood pressure and vagal tone relative to those inputs involved in regulating fluctuations in HR associated with breathing (respiratory sinus arrhythmia).
- Sympathetic inputs would undoubtedly contribute to in vivo sympatho- vagal balance, however, it cannot be directly interpreted from the indices that are currently used to examine the time and frequency domains of heart rate variability. Direct analysis of baroreflex sensitivity may be more informative combined with HR variability analysis.
- Rectal temperature was monitored using a rectal probe inserted 5 cm from the rectal orifice before, during and following shock and resuscitation, and previous experiments show the temperature ranges between 37 to 34 °C.
- the left femoral vein and artery was cannulated using PE-50 tubing for drug infusions and blood pressure monitoring (UFI 1050 BP coupled to a MacLab) and the right femoral artery was cannulated for bleeding.
- Lead II electrocardiogram (ECG) leads were implanted subcutaneously on the left and right front legs and grounded to the back leg. Rats were stabilized for 10 minutes prior to blood withdrawal.
- Hemorrhagic shock was induced by withdrawing blood from the femoral artery at an initial rate of -1 ml/min then decreasing to -0.4 ml/min over 20 min (40-50% blood loss). Initially blood was withdrawn slowly into a 10 mi heparinized syringe (0.2 ml of 1000 U/ml heparin) to reduce MAP to between 35 and 40 mmHg. if MAP increased, more blood was withdrawn to maintain its low value, and the process was continued over a 20 mih period. The animal was left in shock for 60 min with frequent checking to ensure the MAP remains between 35 to 40 mmHg.
- the ability of the invention to be employed for hypotensive resuscitation was examined in number of experiments, and it was found that survival for delayed retrieval times could only be achieved by an intravenous bolus followed by an intravenous infusion (one-two treatment strategy). A single intravenous bolus or a bolus followed by a bolus was not sufficient to prevent circulatory collapse and death after haemorrhagic shock.
- Group 1 Bolus alone: ALM treatment animal received intravenous 0.3 ml bolus 3.0% NaCl (508 mM, 0.045 g/kg) with 1 mM Adenosine (0.24 mg/kg), 3 mM Lidocaine (0.73 mg/kg), and 2.5 mM MgSG 4 (0.27 mg/kg).
- Figure 9 Group 2 Bolus alone vs Bolus and infusion: ALM treatment animal received intravenous 0.3 ml bolus 3.0% ⁇ NaCl with 1 mM Adenosine (0.24 mg/kg), 3 mM Lidocaine (0.73 mg/kg), and 2.5 mM MgSO* (0.27 mg/kg) and after 80 min and an infusion of 1 ml/kg/hr 0.9% NaCl + 3 mg/kg Adenosine + 6 mg/kg Lidocaine + 3.36 mg/kg MgSQ 4 .
- 1.0 mi of composition administered per kg body weight per hour comprised 11.23 mM adenosine, 22 mM lidocaine-HCI and 28 mM MgSO*.
- Group 3 Bolus-Bolus treatment This example shows that an ALM treatment animal that received an intravenous 1 ml bolus of 7.5% NaCl ALM (1 mM Adenosine, 3 mM Lidocaine HCI; 2.5 mM MgS0 ) followed b a second 0.5 ml bolus of 7.5% NaCl ALM (1mM Adenosine (0.2 mg/kg), 3 mM Lidocaine HCI (0.73 mg/kg); 2.5 mM MgSO* (0.27 mg/kg)) at 90 min did not improve survival.
- the examples provide evidence that a intravenous single bolus of 3% or 7.5% hypertonic saline with ALM treatment or a bolus-bolus administration are not adequate for sustained hypotensive resuscitation following a period of shock induced by bleeding. Survival requires the administration of a bolus followed by an intravenous infusion, which is equivalent to a bolus then a drip.
- This example is clinically (or venterinariiy) relevant because long delays can occur to reach the patient or subject in prehospital or military settings. Long delays can also occur in Rural and Remote Medical hospitals or environments. The results also pertain to the battlefield environment where small expeditionary teams routinely operate in austere and hostile environments and have access to limited medical supplies and where evacuatton times may be many hours to days depending upon location.
- RPP peak arterial systolic pressure times heart rate (index of myocardial 02 consumption)
- SDNIM indicates standard deviation of normal io normal R- intervals, where R is the peak of a QRS complex (heartbeat)
- NN50 is the number of pairs of successive beat to beat (NN) that differ by more than
- ALM In the frequency domain, ALM also reduced LF by 54% and HF by 31 % relative to 7.5% NaCI controls, again implying a reduced parasympathetic input to heart rate variability at both low and high frequencies.
- the 33% lower LF/HF ratio in the ALM treated animals than controls would suggest either the drug 1) decreased parasym athetic control of MAP and vagal tone or 2) increased the regulating the effect of respiration on heart rate, or both compared to 7.5% NaCI aione. Since the animais were actively ventilated at ⁇ 9Q strokes per min and heart rate was not different between groups, it appears the fall in LF/HF ratio is due to the drugs action to decrease the parasympathetic input on MAP and vagal tone to increase stability in heart rate.
- Example 8 Effect of beta hydroxy butyrate (BHB) and valproic acid on hypotensive resuscitation hemodynamics
- Rectal temperature was monitored using a rectal probe inserted 5 cm from the rectal orifice before, during and following shock and resuscitation, and previous experiments show the temperature ranges between 37 to 34 C
- the left femoral vein and arter was cannulated using PE-50 tubing for drug infusions and blood pressure monitoring (UFI 1050 BP coupled to a MacLab) and the right femoral artery was cannulated for bleeding.
- Lead II electrocardiogram (ECG) leads were implanted subcutaneously on the left and right front legs and grounded to the back leg. Rats were stabilized for 10 minutes prior to blood withdrawal.
- Hemorrhagic shock was induced by withdrawing blood from the femoral artery at an initial rate of H ml/min then decreasing to -0.4 mS/mtn over 20 min. Initially blood was withdrawn slowly into a 10 ml heparinized syringe (0.2 ml of 1000 U/ml heparin) to reduce MAP to between 35 and 40 mmHg. If MAP increased, more blood was withdrawn to maintain its low value, and the process was continued over a 20 min period. The animal was left in shock for 60 min with frequent checking to ensure the MAP remains between 35 to 40 mmHg.
- Group 1 ALM treatment animal received intravenous 0.3 ml bolus 3.0% NaCI with 1 mM Adenosine (0.24 mg/kg), 3 mM Lidocaine (0.73 mg/kg), and 2.5 mM MgSG 4 (0.27 mg/kg) with 50 mM beta-hydroxy butyrate (D-isomer, 4.7 mg/kg).
- ALM with BHB "kick” started around 15 min and continued through 60 min resuscitation.
- Beta-hydroxy butyrate was added to the hypotensive resuscitation fluid because it is known to bind to the GPR109A receptor on immune cells (monocytes and macrophages) and the vascular endothelium to have a direct anti-inflammatory effect. This example shows that Beta-hydroxy butyrate did not compromise hemodynamic support of hypotensive resuscitation.
- Group 2 Addition of histone deacetylase inhibitor valproic acid to ALM hypotensive resuscitation.
- This example shows that a single 0.3 mi bofus of 3% NaCI with 1 mM Adenosine (0.24 mg/kg), 3 mM Lidocaine (0.73 mg/kg), and 2.5 mM MgSC>4 (0-27 mg/kg).
- administration of valproic acid (VPA) (231 mM in 0,3 ml or 30 mg/kg body weight) raised MAP in the hypotensive range from 40 to 55 mmHg over 60 min after hemorrhagic shock.
- the example further demonstrates that administering an intravenous infusion of 0.9% NaCI ALM protected the animal from suffering circulatory collapse.
- This provides evidence that the addition of valproic acid in a bolus followed by an infusion or drip maintained hemodynamics, and that histone deacetyiase inhibitors may be useful for protecting the brain and other organs of the body during delayed retrieval from the prehospital or military setting to definitive care.
- VPA also is known to have cyto rotective effects from an increase acetylation of nuclear histones, promoting transcriptional activation of deregulated genes, which may confer multi-organ protection.
- Example 9 Effect of hemodynamic stabilization with Adenosine agonist plus l idocaine and magnesium after extreme 50% blood loss
- Rectal temperature was monitored using a rectal probe inserted 5 cm from the recta! orifice before, during and following shock and resuscitation, and previous experiments show the temperature ranges between 37 to 34 C.
- the left femoral vein and artery was cannulated using PE-50 tubing for drug infusions and blood pressure monitoring (UFI 1050 B coupled to a MacLab) and the right femoral artery was cannulated for bleeding.
- Lead II electrocardiogram (ECG) leads were implanted subcutaneously on the left and right front legs and grounded to the back leg. Rats were stabilized for 10 minutes prior to blood withdrawal.
- Hemorrhagic shock was induced by withdrawing blood from the femoral artery at an initial rate of ⁇ 1 ml/min then decreasing to ⁇ Q,4 rr min over 20 min. initially blood was withdrawn slowly into a 10 ml heparinized syringe (0.2 ml of 1000 U/ml heparin) to reduce MAP to between 35 and 40 mmHg. If MAP increased, more blood was withdrawn to maintain its low value, and the process was continued over a 20 min period. The animal was left in shock for 60 min with frequent checking to ensure the MAP remains between 35 to 40 mmHg,
- MAP mean arterial pressure
- the large pulse pressure (difference between systolic and diastolic arterial pressure) indicates a high heart stroke volume despite the body's circulation being maintained at these low arterial pressures.
- Without being limited to mechanism is appears that the addition of the adenosine agonist placed the animal in a deep sleep with protection.
- the Example suggests lowering the level of [GCPA] for and provide a bolus and further treatment in form of continuous infusion.
- Example 10 Nitric Oxide Mechanisms of the Invention for hypotensive resuscitation and other injury states including whole body arrest ⁇ data in Figure 11)
- Rectal temperature was monitored using a rectal probe inserted 5 cm from the recta! orifice before, during and following shock and resuscitation, and previous experiments show the temperature ranges between 37 to 34 C, C.
- the left femoral vein and artery was cannulated using PE-50 tubing for drug infusions and blood pressure monitoring (UFI 1050 BP coupled to a MacLab) and the right femoral artery was cannulated for bleeding.
- Lead II electrocardiogram (ECG) leads were implanted subcutaneously on the left and right front legs and grounded to the back leg. Rats were stabilized for 10 minutes prior to biood withdrawal.
- Hemorrhagic shock was induced by withdrawing blood from the femoral artery at an initial rate of H ml/min then decreasing to -0.4 ml/min over 20 min. Initially blood was withdrawn slowly into a 10 ml heparinized syringe (0.2 ml of 1000 U/ml heparin) to reduce MAP to between 35 and 40 mmHg. If MAP increased, more blood was withdrawn to maintain its low value, and the process was continued over a 20 min period. The animal was left in shock for 60 min with frequent checking to ensure the MAP remains between 35 to 40 mmHg. if MAP deviated from this range either shed blood was re-infused or further blood was withdrawn.
- L-NAME ⁇ ,,,-nitro-L-arginine methyl ester hydrochloride
- NO nitric oxide
- Fig 11 shows that the addition of 30 mg/kg L-NAME to 7.5% NaCl/ALM totally abolished MAP resuscitation during the hypotensive period.
- the addition of L-NAME led to ventricular dysrhythmia with each animal experiencing an average of 65,5 ⁇ 1,5 arrhythmic episodes, ALM cannot resuscitate in the presence of the NOS inhibitor L-NAME indicating the involvement of NOS & or NO in some way.
- ALM operates as a NO-dependent, 'pharmacological switch' which releases a natural "handbrake” on the shocked heart to gently raise MAP and improve whole body protection and stabilization, including brain.
- NO through site-specific and differential modulation of neuronal activity affects cardiac function.
- the nucleus tractus solitari (NTS) receives input from baroreceptors that is processed in this and other regions of the brain and eventually expressed with altered cardiac and whole body functions.
- ALM may modulate CNS function to improve heart and mufti-organ protection from hemodynamic, anti-inflammatory and coagulation correction mechanisms during shock states, and other forms or injury (traumatic and non-traumatic), burns, sepsis, infection and stress and disease states. This may be one of the underlying mechanisms of action of the invention.
- Example 11 Brain and whole body protection during aortic repair surgery on cardiopulmonary bypass
- CPB cardiopulmonary bypass
- hypothermic circulatory arrest temporary interruption of brain circulation
- transient cerebral hypoperfusion transient cerebral hypoperfusion
- manipulations on the frequently atheromatic aorta A combination of antegrade and retrograde cerebral perfusion has also been shown to be useful for brain protection during aortic reconstruction.
- hypothermic circulatory arrest occurs when the systemic body temperature is around 20°C for up to 30 min. It is during this time the surgeon performs the aortic repair and the brain must be protected.
- the brain is normally perfused with cold oxygenated whole blood or blood :fluid dilutions (e.g. 4 parts blood:1 part fluid) at temperatures 20 to 2B a C and as low as 6 to 15°C, Despite these standard-of-care procedures, this is a high-risk operation and there is an unmet need for improved pharmacological protection of the brain and body.
- the operative mortality for aortic arch replacement ranges from 6% to 23%, the incidence of permanent neurological dysfunction from 2% to 16%, and the incidence of temporary neurological dysfunction from 5.6% to 37.9%. Thus there is an unmet need to protect the brain and body during aortic arch procedures, and other types of circulatory arrest operations, in adults, pediatric patients and neonates.
- BHB beta- hydroxybutyrate
- the vehicle can be whole blood, whole blood; crystalloid dilutions or crystalloid alone and isotonic or hypertonic with respect to saline.
- the hypothesis that will be tested is selective cerebral perfusion with blood containing a bolus of
- Treatment belo is defined as the bolus plus infusion with propofol.
- Study Plan There will be four arms to the the study 1) whole blood alone (no treatment), 2) whole blood alone with 3% saline, 3) whole blood with 3% saline and treatment, 4) whole blood with 3% saline and treatment (replace propofol with thiopental.
- the bolus followed by the infusion will be administered 5 min before the operation and continued during the circulatory arrest and rewarming after surgery.
- Data will be compared with blood or fluid vehicle alone with no additives.
- Surgical Methods and Cerebral Perfusion 80 patients (15 per group) will be recruited after obtaining the hospital's internal review board protocol approval and patient consent for the study.
- the methods for aortic arch surgery and dissection are described by Kruger et at, ( Kruger, T., et al, 2011, Circulation 124, 434-443)and Misfield and others ( isfe!d, M., et al, 2012, Ann Thorac Surg. 93, 1502-1508.), and references therein.
- Cerebral perfusion aims for a flow of 10 ml/kg body wt min which is normally adjusted to maintain a radial arterial pressure of between 40 to 70 mm Hg.
- Cerebral monitoring is achieved by means of a right radial arterial pressure line, electroencephalography, regional oxygen saturation in the bilateral frontal lobes with near-infrared spectroscopy, and transcranial Doppler ultrasonographic measurement of the blood velocity of the middle cerebral arteries
- Primary and Secondary Endpoints will include brain damage biomarkers such as neurofilament (NF), SIOOp, glial fibrillary acidic protein (GFAP), and ubiquitin carboxyl terminal hydrolase-LI (UCH-L1) neuron-specific eno!ase (NSE)).
- Brain ischemia will be assessed using blood lactate levels and pH.
- Inflammation will be assessed using select markers (e.g. IL-1, IL-6, IL-12, tumor necrosis factor-alpha), and coagulopathy using coagulometry (aPTT, PT) and visco-elastic ROTEM analysis.
- aPTT coagulometry
- PT visco-elastic ROTEM analysis.
- the 30-day mortality will include any death that occurred from the intraoperative period until the 30 th postoperative day. Secondary end points will be perioperative complications and perioperative and postoperative times, intubation times.
- This example will demonstrate one aspect of the invention, which is to protect the brain using non-arrest levels of the composition in bolus and constant infusion. An arm may be included where the doses are raised to examine another aspect of the invention to arrest the brainstem (and higher centres) during circulatory arrest for aortic reconstructions or large intracranial aneurysm surgeries, This example would also be applicable for pediatric and neonatal circulatory arrest interventions and surgeries.
- Example 12 Brain and whole body protection for abdominal aortic aneurysm
- Study Aim and hypothesis Thirty patients will be recruited after obtaining the hospital's internal review board protocol approval and patient consent for the study.
- the aim of the study is to test the protective effect of intravenous infusion of AL with and without an inflammator such as beta-hydroxybutyrate (BHB) and brain fuel citrate 5 min before and during minimally invasive endovaseular stent grafts in the elective repair of aortic aneurysms.
- BHB beta-hydroxybutyrate
- the hypothesis that will be tested is that intravenous bolus and infusion of 3% NaC! ALM with citrate (1 m ) and BHB (4 m ) will result in 1) targeted systemic hypotension to reduce bleeding, and 2) protect the body and organs (e.g.
- ALM bolus 0.3 mg/kg adenosine;0.6 mg/kg Lidocaine-HCI and Q.03g/kg MgS0 4
- ALM Addenosine; 0.2 mg/kg/min. Lidocaine-HCI; 0.4 mg kg/min and MgSO*; 0,224 g/kg/min
- citrate 1 mM
- BHB BHB (4 mM).
- the bolus and infusion will commence 5 min before percutaneous endovasoular repair. Infusion rate will begin at 10 ml/min/kg and increased to produce hypotensive anaesthetized state to reduce blood loss.
- the primary end points will be biomarkers for the clinical diagnosis of brain injury, inflammatory markers, coagulopathy, temporary neurological deficit, 30-day mortality and mortality-corrected permanent neurological dysfunction. The 30-day mortality included any death that occurred from the intraoperative period until the 30 th postoperative day. Secondary end points will be perioperative complications and perioperative and postoperative times, intubation times.
- the data will demonstrate one aspect of the invention to protect the brain and organs of the body using non-arrest levels of the composition administered as bolus and infusion.
- Example 13 Reducing post-partum hemorrhage, coagulopathy and infection
- PPH Postpartum hemorrhage
- the first line therapy for severe PPH includes transfusion of packed cells and fresh-frozen plasma in addition to uterotonic medical management and surgical interventions.
- Obstetric haemorrhage is associated with hemodynamic instability, inflammator activation and coagulopathy and these women patients have a higher incidence of infection.
- Postpartum uterine sepsis is believed to arise from an ascending infectio caused by colonizing vaginal flora.
- the incidence of infection (post-partum endometritis or infection of the decidua) after vaginal delivery is 0.9 and 3.9% and as high as12-51 % after Caesarean section.
- ALM bolus (0,3 mg/kg adenosine;0.6 mg/kg Lidocaine-HC! and G.03g/kg MgSQ, ⁇ ) followed by intravenous infusion of ALM (Adenosine; 0.2 mg/kg/min. Lidocaine-HCI; 0.4 mg/kg/min and MgSOi; 0.224 g/kg/min) at a flow rate of 10 ml/kg/min would be investigated.
- Example 14 Brain and whole body protection for neonatal or pediatric aortic arch reconstruction
- PVL periventricular ieukomalacia
- necrosis more often coagulation
- the early postoperative period is also a highly vulnerable time for injury because of poor perfusion, free radical and oxidant damage, cyanosis, inflammation, coagulopathy, abnormal vascular reactivity, hyperthermia, endocrine abnormalities and poor g!ycemic control and insulin- resistance including pyruvate dehydrogenase inhibition.
- Postoperative variables such as cyanosis, low systolic and diastolic blood pressures, low cardiac output, and prolonged periods of poor cerebral 0 2 saturation.
- ALM therapy improves 1) brain and 2) whole body function compared to vehicle controls, including cardiac, renal and lung functional improvement.
- the therapy will reduce inflammation, reduce coagulation disturbances and lead to less whole body ischemia.
- ALM bolus and infusion will commence at least 5 min before the operation at a flow rate of -30 m!/kg/min to generate sufficient cerebral pressures for optimal protection.
- the whole body ALM bolus-intravenous infusion can be lowered and continued for further stabilization in the intensive care unit.
- intravenous bolus and infusion to whole body
- intra-arteria! bolus and infusion to brain circuit.
- the whole body infusion may have to be stopped as circulation is stopped and restarted.
- the doses would include ALM bolus (0.3 mg/kg adenosine;0.6 mg/kg Lidocaine-HCI and Q.03g/kg MgS0 4 ) followed by intravenous infusion of ALM (Adenosine; 0.2 mg/kg/min. Lidocaine-HCI; 0.4 mg kg/min and MgS0 4 ; 0.224 g/kg/min ⁇ at 10 ml/m in/kg (whole body), and arterial flow to the brain adjusted to meet the flow requirements according to surgeon preference.
- ALM bolus 0.3 mg/kg adenosine;0.6 mg/kg Lidocaine-HCI and Q.03g/kg MgS0 4
- intravenous infusion of ALM Addenosine; 0.2 mg/kg/min. Lidocaine-HCI; 0.4 mg kg/min and MgS0 4 ; 0.224 g/kg/min ⁇ at 10 ml/m in/kg (whole body), and arterial flow to the brain adjusted to meet the flow
- Brain protection in neonates will include near infrared spectroscopy (MIRS), transcranial Doppler (TCD), electroencephalography (EEG), and serum measurement of S100B protein.
- MIRS near infrared spectroscopy
- TCD transcranial Doppler
- EEG electroencephalography
- serum measurement of S100B protein Whole body protection will be assessed using routine haemodynamic measurements, cardiac output, ultrasound volume relaxation parameters of left ventricular function, troponins, inflammatory markers and coagulopathy. 30-day mortality and infection rates wil! be recorded.
- the data will demonstrate one aspect of the invention to protect the brain, heart, kidney and lungs using non-arrest levels of the composition.
- Example 15 Reducing inflammation, coagulation dysfunction, infection and adhesions during neonatal or pediatric congenital corrective heart surgery
- Post-operative infections include sepsis, wound infection, mediastinitis, endocarditis, and pneumonia and any of these conditions contributes to proionged LOS and increased hospital costs.
- Increased risk factors for major infections were age, reoperation, preoperative length of stay longer than 1 day, preoperative respiratory support or tracheostomy, genetic abnormality, and medium or high complexity score.
- Aim and hypothesis An intravenous bolus of ALM and infusion/drip will begin prior to placing the patient on CPB the cardiac surgery and continued throughout the surgery.
- the hypothesis is that the one-two ALM treatment will induce whole body protection from reducing inflammation and coagulopathy and improve cardiac function (lower troponin and lactate) and reduce infection.
- the bolus and drip will also improve brain and renal function following surgery and reduce hospital length of stay. The results will be compared with historical controls and with vehicle infusion.
- IL-6 interleukin-6
- IL-8 tumor necrosis factor alpha
- PIP polymorphonuclear elastase
- WBC white blood cell
- NG neutrophil count
- IL6 has recently been associated with acute kidney injury within the first 24 hours after pediatric cardiac surgery.
- Coagulation status will be assessed using ROTEM. Cardiac troponins will be measured during and following surgery including 12 hours and 24 hours post-operative times. Brain function will be assessed using blood markers and cerebral oximetry and transcranial Doppler ultrasonographic measurement of the blood velocit of the middle cerebral arteries.
- the data will demonstrate that the intravenous bolus and drip or infusion will confer perioperative protection including improved whole body post-operative cardiac, renal and neural function and blunting of the inflammatory response and restoring coagulation leading to lower intensive care and hospital room stays.
- the ALM therapy can be continued at a !ower dose for whole body stabilization.
- the therapy will be shown to be a centra! component in the management neonatal, paediatric and adult patients, and the critically ill suffering a traumatic and non-traumatic injury.
- Carotid endarterectomy is a procedure used to prevent stroke by correcting blockage in the common carotid artery, which delivers blood to the brain.
- Endarterectomy is the removal of material from the inside of the vessel causing the blockage.
- the surgeon opens the artery and removes the blockage.
- Many surgeons lay a temporary bypass or shunt to ensure blood supply to the brain during the procedure.
- the procedure may be performed under general or local anaesthetic.
- the shunts may take 2.5 minutes and ischemic cerebral signals (flat wave) in eiectroencephaiographic can occur soon after insertion of the shunt.
- the mean shunting time can be around 1 hour for the operation to take place. Damage the brain and other organs can occur during the procedure.
- New ischemic lesions on diffusion-weighted magnetic resonance imaging are detected in 7.5% of patients after carotid endarterectomy, Twenty patients will be recruited after obtaining the hospital's internal review board protocol approval and patient consent for the study.
- the aim of the present study is to provide an arterial ALM bolus and infusion with and without propofo! prior to placing the shunt, and continued for 60 min or as long as the operation takes.
- Diffusion-weighted magnetic resonance imaging will be conducted to examine if there are reduced lesions compared to saline or blood controls.
- the data will demonstrate one aspect of the invention to protect the brain s heart, kidney and lungs of the body using non- arrest levels of the composition involving a bolus and infusion. This is one aspect of the invention showing the clinical advantage of the bolus and drip (infusion) ALM treatment therapy on brain and whole body protection.
- Example 17 Reduced inflammation, coagulation, adhesions and blood loss following shoulder surgery
- Aim of the Study The aim of our study is: 1) to examine the effect of ALM injectable applications or topical sprays at select times within the joint to reduction of local adhesions, reduce local inflammation and reduce local coagulopathy and pain following surgical or arthroscopic repair of the rotator cuff. 2) to examine the effect of intravenous whole body ALM dose and infusion, with and without proprofol, to induce a hypotensive state to reduce bleeding during the surgery, and to protect the whole body from the trauma of surgery with reduced inflammation and coagulation and reduced pain.
- the results will show that a subacromial injection of ALM will reduce inflammation and post operative shoulder stiffness and associated adhesion complications at 6 and 12 months, and the intravenous ALM boius and infusion will lead to per-operative reduced whoie body inflammation, coagulation disturbances and less blood lost during the procedure from the coagulopathy correction and inducing a reproducible hypotensive state.
- the study will show thai ALM bolus-infusion therapy will assist in inducing a whoie body hypotensive anaesthesia to reduce bleeding, which would also be applicable for other types of interventions and surgery including knee surgery and the intravenous bolus- infusion will protect distal areas once a tourniquet at the knee is applied and released every 30 min.
- results of the study will demonstrate one aspect of the invention to protect the joint from stiffness and the whole body using non-arrest levels of the composition involving a bolus and infusion, and another aspect of the invention to facilitate hypotensive state for anesthesia with reduced blood loss.
- Example 18 Reducing infection and post-surgical pericardial adhesions
- the present invention will show that intravenous ALM bolus and infusion during the operation during or following the surgery will lower infection rate and incidence of adhesions following surgery.
- the second aim is to show that ALM in a syringe applied topically or by spray or other means of delivery to the area during, prior to closure of the wound, or following closure of the wound will reduce adhesions, promote healing and reduce infection following cardiac surgery.
- Type I infections are those thai occur within the first week after sternotomy and typically have serosanguineous drainage but no cellulitis, osteomyelitis, or costochondritis. They are typically treated with antibiotics and a single-stage operation. However, the majority of cases are type II Infections that normally occur during the second to fourth weeks after sternotomy and usually involve purulent drainage, cellulitis, and mediastinal suppuration. While it is understood that patients undergoing a median sternotomy for coronary artery bypass grafting have the highest rate of sternal wound infections compared with those for other surgeries, the above example for one aspect of the present invention would also apply to other surgeries and the problem of surgical wound infections.
- Example 19 Treating and reducing pain following marine envenomation.
- the Box Jellyfish (also known as the sea wasp or sea stinger) is the only known coelenterate that is lethal to humans.
- the venom has cardiotoxic, neurotoxic and dermatonecrotic components. It is injected by hundreds of thousands of microscopic stings over a wid area of the body and on the trunk. Absorption into the circulation is rapid. Each sting arises from the discharge of a nematocyst.
- the central rod of the microbasic mastigphore carries the venom, and is like a microscopic spear, which is impaled, on contact, into the victim by a springy protein.
- Other jellyfish may cause a similar syndrome such as Irukandji. When stung, the pain is absolutely excruciating and can lead to shock and death.
- Systemic magnesium in slow boluses of 10 - 20 mMol, may attenuate pain and hypotension.
- Aim and Hypothesis To bring pain relief and hemodynamic and pulmonary support to victims of Marine stingers.
- the hypothesis to be tested is that ALU wi!l produce greater pain relief and whole body physiological support by reducing the devastating effect of the catecholamine storm compared with magnesium alone.
- the present invention will also work by reducing the effect of the catecholamine cascade which can lead to a hypertensive state with associated cardiac and respiratory complications.
- the sam study will be repeated in patients stun by irukandji.
- the invention may apply to other marine and terrestrial envenomations.
- Example 20a ⁇ Fig. 14A-C: Effect adenosine and lignocaine solution with two forms of citrate and elevated magnesium on aortic flow, coronary flow and heart rate after 2 hours of warm (tepid) heart arrest in the working rat heart. Function monitored for 60 min reperfusion.
- mice Male Sprague-Daw!ey rats ⁇ 350-450g were obtained from James Cook University's breeding colony. Animals were fed ad libitum and housed in a 12-hour light/dark cycle. On the day of experiment, rats were anaesthetised with an intraperitoneal injection of Thiobarb (Thiopentone Sodium; 60 mg/kg body wt) and the hearts were rapidly excised as described in Dobson and Jones (Dobson, 2004). Rats were handled in compliance with James Cook University Guidelines (Ethics approval number A 1084), and with the 'Guide for Care and use of Laboratory Animals' from the National institutes of Health (NIH Publication No. 85-23, revised 1985, and PHS Publication 1996).
- Thiobarb Thiobarb
- Adenosine (A9251 >99% purity) and all other chemicals were obtained from Sigma Chemical Company (Castle Hi!l, NSW).
- Lidocaine hydrochloride was purchased as a 2% solution (ilium) from the local Pharmaceutical Supplies (Lyppard, Queensland). Hearts were rapidly removed from anaesthetised rats and placed in ice-cold heparinised modified KH buffer.
- heart preparation, attachment and perfusion are described in by Dobson and Jones (Dobson, 2004) and Rudd and Dobson (Rudd and Dobson, 2009). Briefly, hearts were attached to a Langendorff apparatus and perfused at a pressure head of 90 cm H 2 0 (68 mmHg), The pulmonary artery was cannulated for collection of coronary venous effluent and 0 2 consumption measurements. For working mode operation, a small incision was made in the left atrial appendage and a cannula inserted and sutured.
- the heart was then switched from Langendorff to the working mode by switching the supply of perfusate from the aorta to the left atrial cannula at a hydrostatic pressure of 10 cm H 2 0 (pre-load) and an afterioad of 100 em H 2 0 (76 mmHg).
- Hearts were stabilized for 15 minutes and pre-arrest data recorded before converting back to Langendorff mode prior to inducing normothermic arrest.
- Heart rate, aortic pressure, coronary flow and aortic flow were measured prior to and following 6 hour arrest and cold static storage (see Figure 14).
- Aortic pressure was measured continuously using a pressure transducer (AD! Instruments, Sydney, Australia) coupled to a MacLab 2e (ADI Instruments). Systolic and diastolic pressures and heart rate were calculated from the pressure trace using the MacLab software.
- Krebs buffer Hearts were perfused in the Langendorff and working modes with a modified Krebs-Henseleit crystalloid buffer containing 10-mmol/L glucose, 117 rnmol/L sodium chloride, 5,9-mmol/L potassium chloride, 25-mmol/L sodium hydrogen carbonate, 1.2-mmol/L sodium dihydrogenphosphate, 1 ,12-mmol/L calcium chloride (1.07- mmol/L free calcium ion), and 0.5 2-mmol/L magnesium chloride (0.5-mmol/L free magnesium ion), pH 7,4, at 37_C.
- the perfusion buffer was filtered with a 1-mrn membrane and then bubbled vigorously with 95% oxygen and 5% carbon dioxide to achieve a P02 greater than 600 mm Hg.
- the perfusion buffer was not recirculated.
- the AL solution was made fresh daily and contained 200 ⁇ (0.2 mM or 53.4 mg/L) adenosine plus 500 ⁇ (0.5 m or 136 mg/L) lidocaine-HCl in 10-mmol/L glucose-containing Krebs-Henseleit buffer (pH 7.7 at 37°C), as described by Dobson and Jones with the following modifications: 16 mlVl MgSC1 ⁇ 4 was used instead of 0.512 mM MgCI 2 in the arrest solution and two forms of citrate 1) citrate, phosphate and dextrose (CPD) commercially available solution, and 2) sodium citrate. The following groups were tested (n-8 per group):
- Adenosine lidocaine magnesium (ALM) with 2% CPD (20 ml/L cardioplegia)
- ALM with 3.6 mM Na-citrate Intermittent Delivery The heart is arrested for a total time of 2 or 4 hours and arrest is ensured by a flush of cardioplegia every 18 min.
- the method of intermittent cardioplegia delivery has been previously described by Dobson and Jones (Dobson, 2004).
- Arrest in the Langendorff mode was induced by a 5-minute infusion of cardioplegic solution (50-100 mL) comprising 200 ⁇ (0.2 mM or 53.4 mg/L) adenosine plus 500 ⁇ (0.5 mM or 136 rrig L) lidocaine-HCL
- cardioplegic solution 50-100 mL
- the amount of A and L in mg in 100 ml over a 5 min period would be 5.34 mg adenosine and 13.6 mg Lidocaine-HC! or 1.07 mg adenosine per min and 2.72 mg/min ltdocaine-HCI.
- Fig 14a After 2 hours (Fig 14a) or 4 hours (Fig 14b) of arrest with intermittent cardiopfegic delivery, the heart was switched immediately to the working mode and reperfused with oxygenated, glucose-containing Krebs-Henseleit buffer at 37°C.
- the heart temperature during intermittent arrest ranged from 35°C during delivery to about 25°C before the next delivery (average 28°-3Q D C), as directly measured and discussed by Dobson and Jones (Dobson, 2004).
- Fig 14 A-C Result and Explanation: Surprisingly, at 60 min reperfusion, hearts arrested with ALM with citrate (2% CPD) cardioplegia returned 20% higher aortic flow (AF) than AL alone after 2 hours warm intermittent arrest (Fig 14A), and a 44% higher coronary flow (CF) (Fig 14B). Since cardiac output (CO) ⁇ AF + CF in the working rat heart model, hearts arrested with ALM with citrate (2% CPD) had a 64% higher cardiac output than ALM alone.
- CO cardiac output
- Example 20a This example is the same as Example 20a but differs by arresting the heart for 4 hours not 2 hours. After 4 hours arrest ALM (2% CPD) Result and Explanation (Fig 15 A-C): At 60 min reperfusion, hearts arrested with ALM citrate (2% CPD) or with ALM 1.8 mM Na-citrate cardioplegia returned similar aortic flow as ALM alone after 4 hours warm intermittent arrest (Fig 15A), and a 20% and 0% higher coronary flow respectively than ALM alone (Fig 15B). Thus ALM with citrate (2% CPD) or 1.8 mM Na-citrate had a 20% and 10% higher cardiac output than ALM alone.
- the adenosine and lidocaine solution is also versatile as a preservation solution at both cold static storage (4°C) and warmer intermittent perfusion (28- 30° G) compared with FDA approved solution Celsior.
- the inventor published this information in the Journal of Thoracic and Cardiovascular Surgery in 2009 (Rudd and Dobson, 2009). In 20 0, the inventor also showed that reperfusing the heart for 5 min with warm, oxygenated polarizing adenosine and lidocaine arrest following 6 hours cold static storage ted to significantly higher recoveries in cold adenosine and lidocaine and Celsior hearts and it was proposed that this new reperfusion strategy may find utility during cold-to-warm c wash' transitions and implantation of donor hearts.
- the inventor further reported that the adenosine and lidocaine cardioplegia could preserve the heart over 8 hours in cold static storage with a 78% return of cardiac output using normokalemic, polarizing adenosine and lidocaine at twice their concentrations (0.4 and 1 mM respectively) in glucose- Krebs-Henseleit solution with melatonin and insulin as ancillary or additional agents.
- This new adenosine and lidocaine preservation solution with ancillary agents returned 78% of cardiac output (CO) was significantly higher than 55% CO for AL cardioplegia, 25% CO for Celsior and 4% CO for Custodial (HTK) preservation solutions after 8 hours cold static storage (4°C).
- CO cardiac output
- the buffer was filtered using a one micron (1 ⁇ ) membrane and was not recirculated.
- the concentration of adenosine in the solution was 0.4 mM.
- the concentration of lidocaine in the solution was 1 mM.
- This solution of modified Krebs Henseieit buffer, adenosine and lidocaine is referred to below as the cardioplegia preservation solution.
- the 2.5 L glass bottle with the cardioplegia preservation solution was not actively bubbled itself.
- gentle bubbling was required occurred in the vertical 30 cm long glass oxygenation chamber which delivered the cardioplegia to the isolated heart via the aorta and coronary artery ostia: ie retrograde Langendorff perfusion.
- the temperature-controlled chamber was filled with cardioplegia preservation solution and single gas tubing with a special stainless steel aerator at the end sitting at the bottom of the chamber prior to being delivered to the heart.
- Gentle bubbling was defined as a gas flow adjusted to deliver a few bubbles per sec in the chamber with 95%0 2 /5%C0 2 . In those cases were no bubbling was required the tubing was clamped off.
- the perfusion buffer was filtered using a one micron (1 ⁇ ) membrane and then bubbled vigorously 95%O a /5%C02 to achieve a p0 2 greater than 600 mmHg. The perfusion buffer was not recirculated.
- gentle bubbling reduces coronary flow to 40% recovery of baseline compared to 90% for no-bubbling, This result indicates that gentle bubbling may damage the coronary vasculature that leads to a reduced recovery of flow from vasoconstriction,
- gentle bubblin led to a cardiac output (AF+CF) of less than 10% baseline indicating major damage to the heart's ability to function as a pump, whereas no bubbling of the adenosine and iidocaine preservation cardioplegia led to around 90% full recover after 8 hours of constant perfusion at 4°C (Fig 16G).
- Example 22(b) (Fig. 17 A-D) The effect of adding melatonin and insulin with low and high MgS0 to bubbled adenosine and iidocaine solution during 8 hours of constant perfusion at 4°C in the isolated working rat heart.
- Adenosine and Iidocaine cardioplegia solution with melatonin and insulin (ALMI): Same adenosine and lidocaine preservation cardioplegia above but with 100 ⁇ melatonin and 0,01 lU/ml insulin (ALMI),
- Rewarm Solutions before 60 min reperfusion were the same solutions as the continuous infusion solutions but hearts were slowly rewarm ed for 20 min in Langendorff mode by slowly heating the solutions to 37°C and vigorously bubbled with 95% 0 2 /'5% CO 2 to achieve a p0 2 greater than 800 mmHg and the solutions were not recirculated. This vigorous bubbling is in direct contrast to the gentl bubbling during 8 hours of perfusion (few bubbles per sec).
- Custodioi or histidine-tryptophan-ltetoglutarate solution contained 15 mmol/L NaCI, 9 mmo!/L, KCI, 4.0 mmol/L gC , 0.015 mmol/L CaC , 1 ,0 mmol/L alpha-ketog!utarate, 180 mmol/L histidine, 18 mmoi/L histidjne-HCI, 30 mmol/L mannitol, and 2 mmol/L tryptophan.
- Example 21(a) Equally surprising as Example 21(a) was the finding that adding melatonin and insulin to constant perfusion adenosine and Iidocaine preservation cardioplegia largely abolished the damaging effects of gentle bubbling on aortic flow. Recall in Example 21(a) Fig 16A), perfusing the heart with a solution of adenosine and Iidocaine that had gentie bubbling resulted in zero aortic flow.
- Example 23 Effect of adenosine and Iidocaine solution with low Ca 2+ (0,22 mM.) and high Mg 2+ (2.6 mM) (ALM) with 100 ⁇ cyclosporine A (ALM CyA) during ⁇ hours cold static storage (4°C) in the isolated rat heart
- Hearts were rapidly removed from anaesthetised rats and placed in ice- cold heparinised modified KH buffer. Details of anesthesia, ethics approvals, heart preparation, attachment and perfusion are described in Rudd and Dobson (2009)-.
- the perfusion buffer was filtered using a one micron (1 ⁇ ) membrane and then bubbled vigorously with 95%0 ⁇ /5%C0 2 to achieve a p0 2 greater than 600 mmHg. The perfusion buffer was not recirculated.
- the perfusion buffer was filtered using a one micron (1 p ) membrane and then bubbled vigorously with 95% V5%COa to achieve a pQ 2 greater than 600 mrriHg. The perfusion buffer was not recirculated.
- the adenosine and lidocaine with low calcium and high magnesium (AL (Low Ga 2+ ; High Mg 2+ )) solution contained (0.2 mM) adenosine plus 0.5 mM lidocaine in 10 mmol/L glucose containing Modified Krebs Henseleit ⁇ LowCa 2+ :HighMg 2+ ) buffer (pH 7.7 at 37°CJ The solution was filtered using 0.2 ⁇ filters and maintained at 37 a C. The arrest solution was not actively bubbled with 95% C3 ⁇ 4/5% COa hence the higher pH.
- the average pQ 2 of the AL solution was 140mmHg and the pC0 2 was 5-10 mrrtHg.
- cyclosporine A improves cardiac output by 1.5 times following 6 hours cold static storage. Cyclosporine A may be a possible additive to the ALM cardioplegia/preservation solution for the arrest, protection and preservation of organs, cells and tissues.
- Example 24 (Fig 18) The effect of adenosine and lidocaine solution with 0.3 mg/L sildenafil citrate over 2 hours warm arrest (29°C) given every 20 minutes (2 min infusion) and 60 min reperfusion in the working rat heart
- Rat Hearts were rapidly removed from anaesthetised rats and placed in ice-cold heparinised modified KH buffer. Details of anesthesia, ethics approvals, heart preparation, attachment and perfusion methods are described in Dobson and Jones (Dobson, 2004).
- the adenosine and lidocaine solution was made fresh daily and contained 200 ⁇ (0.2 mM or 53.4 mg/L) adenosine plus 500 ⁇ (0.5 m or 136 mg/L) lidocaine-HCL (arrest and 2 min infusion every 20 min is the same as example 20)
- the concentration of sildenafil citrate 3 mg/L (6.3 micromolar).
- AL sildenafil produces 85% cardiac output and 100% heart rate after 2 hours warm arrest.
- Example 2S Effect of adenosine and lidocaine solution with normal Ca 2+ (1.12 mM) and normal Mg 2* (0,5 mM) with 10 mM 2,3-Butanedione Monoxime (BDM) A during 2 hours of warm arrest (29°C) in the isolated rat heart (intermittent delivery every 20 min)
- BDM 2,3-Butanedione Monoxime
- Rat Hearts were rapidly removed from anaesthetised rats and placed in ice-cold heparinised modified KH buffer. Details of anesthesia, ethics approvals, heart preparation, attachment and perfusion methods are described in Dobson and Jones (Dobson, 2004).
- the adenosine and lidocaine solution was made fresh daily and contained 200 ⁇ (0.2 mM or 53.4 mg/L) adenosine plus 500 ⁇ / ⁇ (0,5 mM or 136 mg/L) lidocaine-HCL (arrest and 2 min infusion every 20 min is the same as example 20) Results:
- Example 26 Effect of adenosine and iidocaine solution with normal Ca 2+ ⁇ 1.12 mM) and normal Mg 2+ (0.5 mlVI) with 54 ⁇ propofol (P) (1mg/L) during 2 hours of warm arrest ⁇ 29°C) in the isolated rat heart (intermittent deisvery every 20 min).
- Rat Hearts were rapidly removed from anaesthetised rats and placed in ice-cold heparinised modified KH buffer. Detatis of anesthesia, ethics approvais, heart preparation, attachment and perfusion methods are described in Dobson and Jones (Dobson, 2004), The adenosine and iidocaine solution was made fresh daily and contained 200 ⁇ (0.2 mM or 53.4 mg/L) adenosine plus 500 ⁇ (0.5 mM or 136 mg/L) lidocaine-HCL (arrest and 2 min infusion every 20 min is the same as example 20) Results:
- Example 27 Effects of polarizing ALM with Insulin microplegia vs Buckberg 1 :4 high potassium depolarizing cardioplegia on intracellular metabolism in human cardiac surgery. Pro-survival kinase, and apoptosis in humans.
- Example 28 Effect of polarizing adenosine-lidocaine-magnesium (ALM) with insulin microplegia (MA AS) vs High Potassium Depolarizing 4:1 cardioplegia in higher risk diabetics undergoing revascularization cardiac surgery for unstable angina.
- ALM adenosine-lidocaine-magnesium
- MA AS insulin microplegia
- MA AS insulin microplegia
- cardioplegia vs High Potassium Depolarizing 4:1 cardioplegia in higher risk diabetics undergoing revascularization cardiac surgery for unstable angina.
- Diabetes mellitus affects 230 million people worldwide. Diabetes is a well-recognized independent risk factor for mortality and morbidity due to coronary artery disease. When diabetic patients need cardiac surgery, either GABG or valve operations, the presence of diabetes represents an additional risk factor for these major surgical procedures.
- Diabetic patients undergoing CABP have, on the basis of the relative risk evaluation, a 5-fold risk for renal complications, a 3.5-fold risk for neurological dysfunction, a double risk of being hemotransfused, reoperated or being kept 3 or more days in the iCU in comparison with non-diabetic patients.
- diabetic patients undergoing valve operations have a 5-fold risk of being affected by major lung complications.
- Current hyperkalemic techniques of cardioplegia arrest result in increased myocardial apoptosis and necrosis in diabetics, especially during unstable angina (UA) and ischemia/reperfusion injury.
- No study has investigated the effects of microplegia addition with po!arizing-arresting substrates with adenosine and lidocaine and magnesium (AIM) with insulin (MAPAS) in this setting.
- AIM adenosine and lidocaine and magnesium
- MAPAS composition was 10.4 mg Adenosine, 43 mg Lidocaine-HCI and 3.5 g MgS0 4 in 40 ml w1 m Adenosine, 4 mM Udocaine-HCI and 350 mM gSC in 40 mi) with insulin.
- Troponin-I and lactate were sampled from coronary sinus at reperfusion (T1), and from peripheral biood preoperatively (TO), at 6 (T2), 12 (T3) and 48 (T4) hours.
- CI cardiac index
- CCE cardiac-cycle efficiency
- !SVR indexed systemic vascular resistances
- CVP central venous pressure
- Echocardiographic wall motion score index investigated the systolic function, E- wave (E), A-wave (A), E/A, peak early-diastolic TDi-mitrai annuiar-velocity (Ea), E/Ea the perioperative diastolic function preoperatively (TO) and at 96 hours (T1):, Results: Data are presented in Table 2.
- Example 29 The effect of mieroptegia AL and Insulin solution with a form of citrate (CPD or sildenafiil citrate) on cardiac function and inflammation, coagulation, and brain function during and following cardiac surgery,
- CPD citrate
- sildenafiil citrate a form of citrate
- cardiopulmonary bypass for surgical cardiac procedures is characterized by a whole-body inflammatory reaction and coagulation imbalances due to the trauma of surgery, contact of blood through nonendothelialized surfaces which can activate specific (immune) and nonspecific (inflammatory) and coaguiative responses (). These responses are then related with postoperative injury to many body systems, like pulmonary, renal or brain injury, excessive bleeding and postoperative sepsis.
- Example 30 The effect of ALM solution with a form of citrate (CPD or sildenafiil citrate) on cardiac function and the presence of microparticles (MPs) in the biood during and following cardiac surgery.
- CPD citrate
- MPs microparticles
- cardiopulmonary bypass for surgical cardiac procedures is characterized by a whole-body inflammatory reaction and coagulation imbalances due to the trauma of surgery, contact of blood through nonendothelialized surfaces which can activate specific (immune) and nonspecific (inflammatory) and coaguiative responses. These responses are then related with postoperative injury to many body systems, like pulmonary, renal or brain injury, excessive bleeding and postoperative sepsis. Microparticles are known to contribute to activation of the complement system in patients undergoing cardiac surgery and ma be linked to brain and organ injury.
- Example 31 Lung preservation with ALM with sildenafil citrate, ALM citrate phosphate dextrose (CPD), ALM citrate with cyclosporine A or ALM with erythropoietin, glyceryl trinitrate and zoniportde in the pig after 12 and 24 hour cold ischaemia.
- CPD citrate phosphate dextrose
- Pulmonary preservation for transplantation is associated with inflammation, endothelial cell injury and surfactant dysfunction. Inflammation and the induction of the primary immune response are important in arresting an organ and in lung preservation and can be assessed by measuring tumor necrosis factor alpha (T Fctj, interleukin-6 (IL-6) and receptor for advanced glycafion endproducts (RAGE) in branchoalveolar lavage fluid.
- T Fctj tumor necrosis factor alpha
- IL-6 interleukin-6
- RAGE receptor for advanced glycafion endproducts
- Aim The study's goal is to assess the effect of ALM cardioplegia preservation solutions on lung function following 12 and 24 hour cold storage and compare with Celsior and low phosphate dextran solution (e.g. Perfadex, Vitrolife) and Lifor (LifeB!ood Medical Inc. NJ ⁇ .
- Celsior and low phosphate dextran solution e.g. Perfadex, Vitrolife
- Lifor LifeB!ood Medical Inc. NJ ⁇ .
- BALF Bronchoalveolar lavage fluid
- ALM preservation solutions will lead to no deaths after storage and implantation compared to Celsior or low potassium dextran, and Lifor storage solutions after both 12 and 24 hours.
- a second finding will be that ALM groups will have significantly less pulmonary vascular resistance index, and less sequestration of neutrophils compared to Celsior or low potassium dextran, and Lifor storage solutions after both 12 and 24 hours. Improvement in surfactant activity will also be evident in the ALM solutions and improved haemodynamics over 5 hours post storage and transplant.
- ALM cardioplegia preservation with Sildenafil citrate or CPD will be superior to standard of care solutions and FDA approved Celsior and Perfadex (or Vitrolife), or Lifor for cold lung storage and implantation.
- Example 32 Effect of ALM with sildenafil citrate, ALM citrate, ALM citrate with Cyclosporine A, ALM Erythropoietin or ALM with erythropoietin, glyceryl trinitrate and zonipori.de in the ex-vivo lung perfusion (EVLP) Organ Care System (OCS).
- EVLP ex-vivo lung perfusion
- OCS Organ Care System
- EVLP ex-vivo lun perfusion
- Aim The aim of this study was to assess the feasibility of transplanting high-risk donor lungs using ALM solutions and comparing with Ceisior and Sow potassium dextran solutions (Perfadex, Vitrolife) or Lifor (LifeB!ood Medical) at 29-30*0 for lung preservation.
- Lungs will be considered suitable for transplantation if 1) during EVLP the P02:Ft02 ratio ⁇ ie. the partial pressure of oxygen e vivo (P02) to the fraction of inspired oxygen (Fi02) of 350 mm Hg or more) and 2) if deterioration from baseline levels of all three physiological measurements (pulmonary vascular resistance, dynamic compliance, and peak inspirator pressure) was less than 15% while the lungs were ventilated with the use of a tidal volume of 7 ml per kilogram of donor body weight and a rate of 7 breaths per minute during the perfusion period.
- the primary end point will be graft dysfunction 72 hours after transplantation. Secondary end points will be 30-day mortality, bronchial complications, duration of mechanical ventilation, and length of stay in the intensive c re unit and hospital.
- Example 33 Effect of ALM with sildenafil citrate, ALM citrate, ALM citrate cyclosporine A, ALM Erythropoietin or ALM with erythropoietin, glyceryl trinitrate and zoniporide for the ex-vivo lung perfusion with and without nanoparticles containing oxygen with the capacity to release 0 2 to the cells mitochondria.
- Oxygen loaded lipid-coated perfluorocarbon is required to sustain life in amounts and partial pressures that can range from small to high-energy demand states. Nanobubbles can be prepared with gas "storage" core. Perfluoropentan gas can favor oxygen entrapment. On a volume basis, Van Liew has previously shown that gaseous perfluorocarbon compounds may deliver more oxygen than liquid perfluorocarbons. Oxygen loaded lipid-coated perfluorocarbon
- microbubbles have been prepared for oxyge delivery; these oxygen-enriched microbubbles have been tested in a rat model of anemia and the results showed that it maintained the rat's survival at very low hematocrit levels.
- the oxygen release kinetics could be enhanced after nanobubble insonation with ultrasound at 2.5 MHz. It has previously been shown that oxygen-filled nanobubbles were prepared using perfluoropentan as core and dextran sulphate, a polysaccharide polymer, as shell the dextran nanobubbles were able to release oxygen In hypoxic condition.
- Aim The study is the same design as Example 31 differing only in the ALM groups with a form of citrate and oxygen loaded nanoparticie and solutions perfused lungs at normothermic (tepid) temperatures for 4 hours.
- Oxygen-filled nanobubbles were prepared using perfluoropentan as core and dextran sulphate, a polysaccharide polymer, as shell (Gavafli et al conflict 2009). Polyvinylpyrrolidone (PVP) was added to the shell as a stabilizing agent. Methods same as Example 31 and 5 ALM groups (50 lungs).
- Example 34 Effect of ALM with sildenafil citrate, ALM with citrate, ALM citrate eyclosporine - A or ALM Erythropoietin (and a separate group ALM with erythropoietin, glyceryl trinitrate and zoniporide) to treat the donor patient 5 to 15 min before organ harvest and improve donor orga viabi!ity and function.
- Transplanted lungs are subjected to injuries including the event causing death of the donor, the inflammatory cascade in brain death, resuscitation of the donor and management in the intensive-care unit and on ventilation.
- injury related to organ harvest, preservation (storage or perfusion), transport, and implantation injury Once implanted from donor to recipient, isohaemia-reperfusion injury is followed by immunological attack of the foreign organ by the recipient host. For optimum short-term and long-term results, a composition and method is needed to prevent injury at all these stages. Organ preservation thus begins in the donor. Cerebral injury and brain death also is associated with apparent hypercoagulation and poor organ outcome.
- Aim The aim of this study is to examine the effect of ALM citrate infusions in the validated pig model of intracranial hemorrhage and brain death.
- Methods Pigs wilt be divided into 8 groups of 10 pigs per group and the solutions ⁇ will be infused 5 min before organ harvest after pronounced brain death and the catecholamine storm.
- the following metrics will include inflammatory markers TnF alpha, IL6, epinephrine, lactate, pH, hemodynamics, cardiac function prior to harvest and coagulopathy. immediately following harvest; tissues will be prepared for histology and tissue fluorescence studies examining tissue injury.
- Example 35 Reducing memory loss, blood loss, coagulopathy and protecting the kidney and organs during cardiac surgery including aortic repair surgery: ALM citrate solution and drug loaded solid lipid nanoparticles for brain protection.
- Brain injury in the form of temporary or permanent neurological dysfunction also remains a major cause of morbidity and mortality following aortic arch surger or large intracranial aneurysm surgeries in both adults and pediatric and neonate patients.
- Study Aim The aim of the study is to test the protective effect of ALM with sildenafil citrate, ALM citrate beta-hydroxy butyrate and ALM citrate -propofol loaded into nanospheres and without nanospheres on brain function,
- the vehicle will include whole blood.
- ALM bolus will be ⁇ 1 trig adenosine; 2 mg Licfocaine- HCI and 0.3g MgS0 .) and ALM infusion Adenosine; 0.2 mg/kg/min.
- Lidocaine-HCI 0.4 mg/kg/min and ⁇ 3 ⁇ 430 4 ; 0.224 g/kg/min.
- Sildenafil 1 mg/L s propofol 1 mg/kg; BHB (4 m blood concentration).
- Surgical Methods and Cerebral Perfusion 72 patients (8 per group) will be recruited after obtaining the hospitaf's internal review board protocol approval and patient consent for the study.
- the methods for aortic arch surgery and dissection are described by Kruger et al., (Kruger et a!., 2011) and !V!isfield and others ( isfeld et a!., 2012), and references therein.
- Cerebral perfusion aims for a flow of 10 ml/kg body wt min which is normally adjusted to maintain a radial arterial pressure of between 40 to 70 mm Hg (Di Eusanio et al., 2003).
- Cerebrai monitoring is achieved by a right radial arterial pressure line, electroencephalography, regional oxygen saturation in the bilateral frontal lobes with near- infrared spectroscopy, and transcranial Doppler ultrasonographic measurement of the biood velocity of the middle cerebral arteries.
- Primary and Secondary Endpoints will include brain damage biomarkers such as neurofilament (NF), S100 , giiai fibrillary acidic protein (GFAP), and ubiquitin carboxyl terminal hydralase-U (UCH-L1) neuron-specific enolase (NSE)) (Yokobori et al., 2013), Brain ischemia will be assessed using blood lactate levels and pH. Inflammation wiil be assessed using select markers (e.g. iL-1, !L-6, IL-12, tumor necrosis factor-aipha), and coagulopathy using coagulometry (aPTT, PT) and visco-elastic ROTE analysis.
- NF neurofilament
- GFAP giiai fibrillary acidic protein
- UCH-L1 ubiquitin carboxyl terminal hydralase-U
- NSE neuron-specific enolase
- Temporary neurological deficit, 30-day mortality and mortality-corrected permanent neurological dysfunction will be assessed.
- the 30-day mortality will include any death that occurred from the intraoperative period until the 30 ih postoperative day.
- Secondar end points will be perioperative complications and perioperative and postoperative times, intubation times.
- This example will demonstrate one aspect of the invention, which is to protect the brain using non-arrest levels of the composition in boius and constant infusion with and without nanoparticies.
- An arm may be included where the doses are raised to examine another aspect of the invention to arrest the brainstem (and higher centres) during circulatory arrest for aortic reconstructions or large intracranial aneurysm surgeries. This example would also be applicable for pediatric and neonatal circulatory arrest interventions and surgeries,
- Example 36 Effect of AL or ALM solution with polyethylene glycol, 3-
- BDM Butanedione Monoxime
- BSA bovine serum albumin
- kidney preservation is to reduce damage to the kidney from pre-harvest to implantation, and of particular interest is the time for the kidney to provide adequate renal function, reducing the need for dialysis, the primary purpose of the transplant.
- One key factor is effective graft washout of blood remnants before ischemia cold storage. The presence of blood remnants and cellular debris may contribute to impaired blood flow and injury upon reperfusion.
- An effective washout of the kidney by the preservation solution prevents cell swelling, formation of interstitial edema, and excessive cellular acidosis, injury and potentially graft failure.
- Aim To examine the effect of a variety of AL( ) solutions in kidney washout (flush) and 12 hours cold static preservation compared to FDA approved Custodial (HTK) in adult pigs .
- Kidneys were harvested from Australian Yorkshire pigs (35 - 40Kg) from a local abattoir in Charters Towers. Animals were sacrificed using a captive bolt stunner as per the Humane Slaughter Act and then exsanguinated. Kidneys were removed surgically and placed in a dish for approximately 15 minutes of warm ischaemia for preparation. The renal artery, vein and ureter were identified and clipped to avoid accidental damage, while excess peri-renal connective tissue and the renal capsule were removed. Kidneys were then flushed with 700 - 800 mis of preservation solution held at a 1m pressure head.
- kidneys were weighed and placed in a zip-lock plastic bag containing 200 - 250ml$ of the same preservation solution then stored at 4°C for 12 hours in an ice-filled polystyrene retrieval box. Kidney weights were recorded 1) prior to, 2) following flushing and again 3) followin the 12 hour cold static storage (CSS). For quantitative evaluation of the washout, the remaining red blood cells were counted in specimens of the corticomedullary junction. I a blinded manner, counting of RBCs was performed in ten randomly selected fields of hematoxylin and eosin (HSE)-stained sections
- Example 37 Arresting, protecting and preserving stem ceils with ALM sildenafil citrate, ALM citrate phosphate dextrose (CPD), ALM with CPD and cyclosporine A or ALM with erythropoietin, glyceryl trinitrate and zoniporide.
- ALM sildenafil citrate ALM citrate phosphate dextrose (CPD)
- glyceryl trinitrate and zoniporide Arresting, protecting and preserving stem ceils with ALM sildenafil citrate, ALM citrate phosphate dextrose (CPD), ALM with CPD and cyclosporine A or ALM with erythropoietin, glyceryl trinitrate and zoniporide.
- Stem cells are pluripotent, self-renewing cells found in all multicellular organisms, in adult mammals, stem celts and progenitor cells act as a repair system for the body, replenishing tissues.
- stem cells have the potential to develo into many different kinds of human tissue ceils. They remain 'quiescent 1 as undifferentiated cells within tissues or organs as long as tissue homeostasis does not require generation of new cells. Here, they can renew themselves or differentiate into some or all major specialized cell types that make up the tissue or organ. This 'quiescent' state, one reversible cell cycle withdrawal, has long been viewed as a dormant state with minimal basal activity.
- NSC neural stem cells
- the first function is to actively maintain the quiescent state, indicating that this is not simply a state of dormancy but in fact under active regulation.
- the second is to prime the cells for activation, a process that is characterized by the upregulation of multiple cellular processes necessary for cells to enter the ceil cycle and begin the process of differentiation.
- Neural stem cells are not only a valuable tool for the study of neural development and function, but an integral component in the development of transplantation strategies for neural disease. Regardless of the source material, similar techniques are used to maintain NSC in culture and to differentiate NSC toward mature neural lineages, in addition, distinct cell membrane voltage controls are found in many precursor cell systems and cancer cells, which are known for their proliferative and differentiation capacities, respectively.
- Aim To examine stem cell 'quiescence' in different solutions after 12 and 24 hours of warm 25°G) and cold (4°C) temperature storage and characterize the fate of defined populations of neural precursor cells following transplantation. Differentiated cells will exhibit typical morphological changes and expressed neuronal (nestin, mitogen-acttvated protein-2, synaptophysin), glial (S100, glial fibrillary acid protein).
- Methods Methods for for isolating multi otent NSC and neural precursor cells ( PC) from embryonic rat CNS tissue (mostly spinal cord) are described in Bonner et a!.,.
- neural precursor cells can be separated into neuronal and glial restricted precursors and used to reliably produce neurons or glial cells both in vitro and following transplantation into the adult CNS.
- Cells will be preserved in different culture solutions with and without ALM sildenafil citrate, ALM citrate phosphate dextrose (CPD), ALM with CPD and cyclosporine A or ALM with erythropoietin, glyceryl trinitrate and zoniporide and quiescent and differentiation will be examined after 12 and 24 hours.
- Membrane potentials will be performed using the methods described in Sundeiacruz et al. (Sundelacruz et al., 2009).
- Example 38 Rat Model of Hypotensive Anesthesia and whole body arrest:
- mice Male Sprague Dawley rats (300-450 g) were fed ad libitum with free access to water and housed in a 12-hr light-dark cycle. Animals were not heparinized and anesthetized with an intraperitoneal injection of 100 mg/kg sodium thiopentone (Thiobarb). Anesthetized animals were positioned in the supine position on a custom designed cradle. A tracheotomy was performed and animals were artificially ventilated (95-100 strokes min "1 ) on humidified room air using a Harvard Small Animal Ventilator (Harvard Apparatus, Mass., USA). Femoral artery and vein cannulations were performed on the left leg for drug pressure monitoring and drug infusions. A lead II ECG was attached via ECG wires. A rectal probe was inserted 5.0 cm and the temperature ranged between 37 and 34 °C,
- a 0.2 ml bolus intravenous injection of a composition comprising 0.2 mg adenosine , 0,4 mg lidocaine-HCI and 200 mg MgSC in 0.9% saline and 0.1% citrate phosphate dextrose (CPD) was administered to a rat. No propofol was in this composition.
- the concentration of each of the components in the composition was as follows, adenosine 3.75 mM, lidocaine-HCI 7.38 mM, MgS0 4 833 mM, and citrate 3.4 mM.
- the dosage of each of the components administered to the animal was as follows, adenosine 0.6 mg/kg, lidocaine-HCI 1.2 mg/kg, MgSC 600 mg/kg, and citrate 0.6 mg/kg.
- Example 2 In the same animal as Example 1 , after 10 min, a 0.1 mi bolus intravenous injection of the composition comprising 0,1 mg adenosine , 0,2 mg iidocaine-HCI 200 mg MgSC and propofol in 0.9% saline and 0.1% citrate phosphate dextrose (CPD) was administered.
- the concentration of each of the components in the composition was as follows, adenosine 3.75 mM, iidocaine-HCI 7.38 mM, MgSC 1666 mM, citrate 3.40 m and propofol 18.5 mM.
- the dosage of each of the components administered to the animal in this step was as follows, adenosine 0.6 mg/kg, lidocaine-HCl 1.2 mg/kg, MgSO* 600 mg/kg, citrate 0.3 mg/kg and propofol 1 mg/kg.
- MAP Increased over 6 times and heart rate was 208 beats per min (HR 208 bpm, BP 109/57 mmHg, MAP 75 mmHg, Temp 36.4°C, see Figs 19 I and J), After 15 minutes there was nearly full recovery of blood pressure and heart rate (HR 308 bpm, BP 135/ ⁇ 2 mmHg, MAP 106 mmHg, Temp 36.1°C, see Figs 19 K and L).
- HR 308 bpm, BP 135/ ⁇ 2 mmHg, MAP 106 mmHg, Temp 36.1°C, see Figs 19 K and L The animal spontaneously returned hemodynamics without any chest compressions or other interventions.
- a composition comprising 1.25 g Adenosine, 2.5 g Lidocaine HCI, 1.25 g MgS0 2% CPD in 250 ml of 0.9% NaCI is provided.
- the concentration of each of the components in the composition was as follows, adenosine 18.71 mM, Iidocaine-HCI 36.92 mM, MgSC ⁇ » 20 mM, and citrate 2.1 mM.
- the adenosine base powder was added with stirring until dissolved.
- the pH of the solution was checked and adjusted if necessary to between 7,2 and 7.5 (preferably 7.4).
- the solution was made up to 250 ml with 0.9% NaCI solution and filtered through a 0.22 micron filter into a sterile bag.
- composition may be administered by IV infusion at the following rates:
- IV infusion rates Bolus 0, 1 ml/kg then 0.1-0.5 ml/kg/min during operation administered following anesthesia and maintain or change to 0.1 ml/kg/min during sternal closure for 2 hours at ICU.
- the IV administration could increase to 1 ml/kg/hr or higher, or Sower than 0.1 ml/kg/hr,
- DURING Recovery Infusion rate: 0.1 ml/kg/hr (reduced from 0.5 to 0.1 during Sternal closure and continued for 2 hours into ICU
- MgS0 - 0.1/250 X 1.25g 0.5 mg/hr/kg.
- the above mentioned dosages of adenosine used during the infusion are substantially reduced compared to the dosages of adenosine typically used during major surgery, such as when adenosine is used as an analgesic.
- the above mentioned dosages of magnesium used during the infusion are substantially reduced compared to the dosages of magnesium typically used during major surgery, such as when magnesium is used during cardiac surgery.
- a composition comprising adenosine, lidocaine, gSC 2% CPD in 250 mi of 0.9% NaCl is provided.
- the concentration of each of the components in the composition may be as follows;
- CPD contains in 100 ml
- Citric Aeid ( onohydrate), 0.327 g MW 210.14
- the pH of the solution was checked and adjusted if necessary to between 7.2 and 7.5 (preferably 7.4).
- the solution was made u to 80 ml with 0.9% NaCI solution and filtered through a 0.22 micron filter into a sterile bag.
- the composition may be administered by a bolus to the blood to provide a contact concentration at the heart.
- a bolus of the composition is diluted up to 1 L of blood to provide the following heart contact concentrations:
Landscapes
- Health & Medical Sciences (AREA)
- Life Sciences & Earth Sciences (AREA)
- Chemical & Material Sciences (AREA)
- Veterinary Medicine (AREA)
- Public Health (AREA)
- Animal Behavior & Ethology (AREA)
- General Health & Medical Sciences (AREA)
- Medicinal Chemistry (AREA)
- Pharmacology & Pharmacy (AREA)
- Epidemiology (AREA)
- General Chemical & Material Sciences (AREA)
- Chemical Kinetics & Catalysis (AREA)
- Engineering & Computer Science (AREA)
- Nuclear Medicine, Radiotherapy & Molecular Imaging (AREA)
- Organic Chemistry (AREA)
- Bioinformatics & Cheminformatics (AREA)
- Molecular Biology (AREA)
- Pain & Pain Management (AREA)
- Anesthesiology (AREA)
- Dermatology (AREA)
- Inorganic Chemistry (AREA)
- Oil, Petroleum & Natural Gas (AREA)
- Biochemistry (AREA)
- Neurosurgery (AREA)
- Neurology (AREA)
- Cardiology (AREA)
- Heart & Thoracic Surgery (AREA)
- Hematology (AREA)
- Biomedical Technology (AREA)
- Diabetes (AREA)
- Urology & Nephrology (AREA)
- Vascular Medicine (AREA)
- Rheumatology (AREA)
- Surgery (AREA)
- Pharmaceuticals Containing Other Organic And Inorganic Compounds (AREA)
- Medicines That Contain Protein Lipid Enzymes And Other Medicines (AREA)
- Acyclic And Carbocyclic Compounds In Medicinal Compositions (AREA)
- Agricultural Chemicals And Associated Chemicals (AREA)
- Measuring Or Testing Involving Enzymes Or Micro-Organisms (AREA)
Abstract
Description

























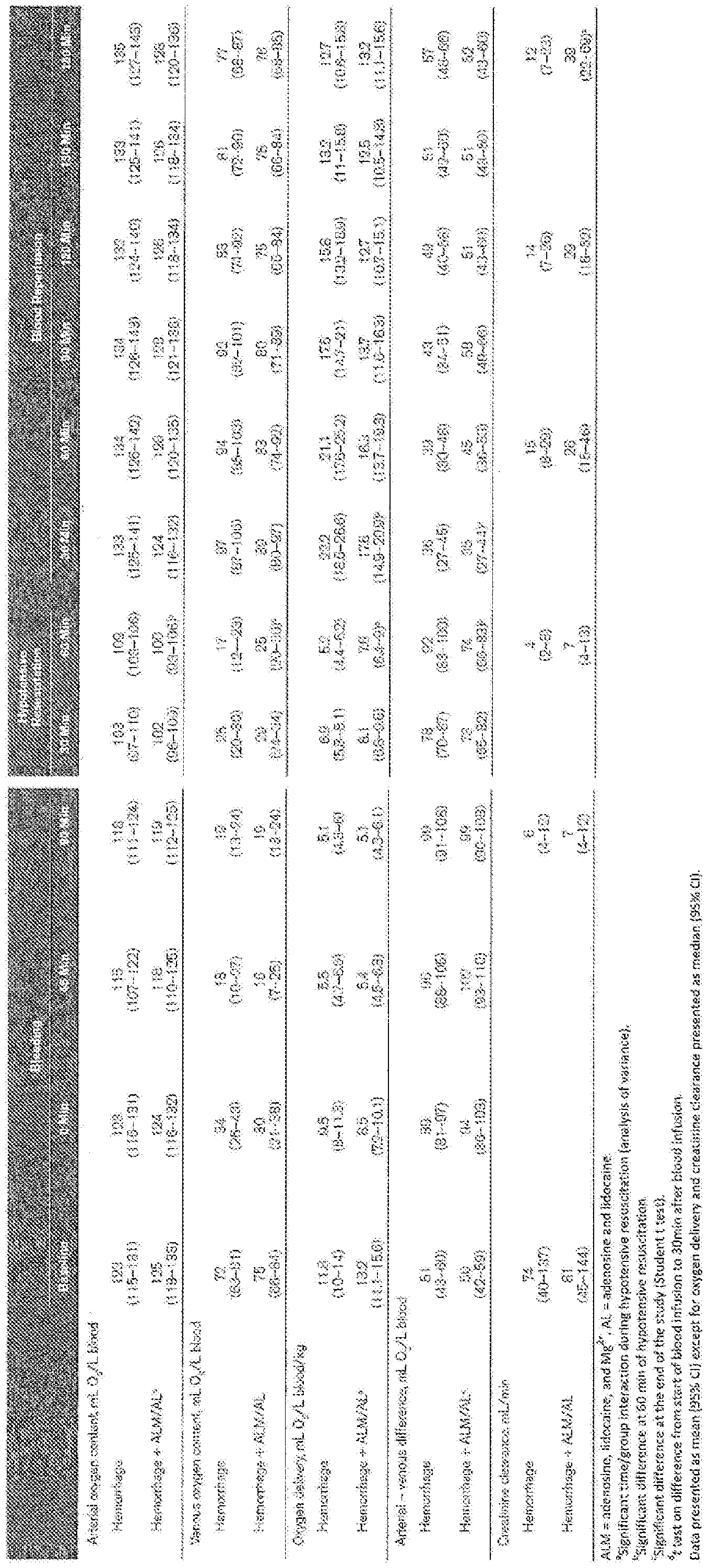

Claims
Priority Applications (7)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| EP14826665.3A EP3021855A4 (en) | 2013-07-17 | 2014-07-17 | A method for treating haemorrhage, shock and brain injury |
| CA2917629A CA2917629A1 (en) | 2013-07-17 | 2014-07-17 | A method for treating haemorrhage, shock and brain injury |
| BR112016000804A BR112016000804A2 (en) | 2013-07-17 | 2014-07-17 | METHOD TO TREAT HEMORRHAGE, SHOCK AND BRAIN INJURY |
| CN201480051011.0A CN105705151A (en) | 2013-07-17 | 2014-07-17 | A method for treating haemorrhage, shock and brain injury |
| MX2016000650A MX2016000650A (en) | 2013-07-17 | 2014-07-17 | A method for treating haemorrhage, shock and brain injury. |
| AU2014292825A AU2014292825A1 (en) | 2013-07-17 | 2014-07-17 | A method for treating haemorrhage, shock and brain injury |
| US15/000,727 US10786525B2 (en) | 2013-07-17 | 2016-01-19 | Method for treating haemorrhage, shock and brain injury |
Applications Claiming Priority (10)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| AU2013902659 | 2013-07-17 | ||
| AU2013902657A AU2013902657A0 (en) | 2013-07-17 | A method for reducing infection, sepsis and injury | |
| AU2013902658A AU2013902658A0 (en) | 2013-07-17 | A method for reducing inflammation, coagulation and adhesions | |
| AU2013902659A AU2013902659A0 (en) | 2013-07-17 | A method for treating haemorrhage, shock and brain injury | |
| AU2013902656 | 2013-07-17 | ||
| AU2013902656A AU2013902656A0 (en) | 2013-07-17 | A method for inducing whole body arrest | |
| AU2013902657 | 2013-07-17 | ||
| AU2013902658 | 2013-07-17 | ||
| AU2013903644 | 2013-09-23 | ||
| AU2013903644A AU2013903644A0 (en) | 2013-09-23 | A method for organ arrest, protection and preservation and reducing tissue injury |
Related Parent Applications (2)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| PCT/AU2014/050128 Continuation-In-Part WO2015006827A1 (en) | 2013-07-17 | 2014-07-17 | A method for inducing whole body arrest |
| PCT/AU2014/050133 Continuation-In-Part WO2015006831A1 (en) | 2013-07-17 | 2014-07-17 | A method for reducing, inflammation, coagulation and adhesions |
Related Child Applications (2)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| PCT/AU2014/050128 Continuation-In-Part WO2015006827A1 (en) | 2013-07-17 | 2014-07-17 | A method for inducing whole body arrest |
| US15/000,727 Continuation-In-Part US10786525B2 (en) | 2013-07-17 | 2016-01-19 | Method for treating haemorrhage, shock and brain injury |
Publications (2)
| Publication Number | Publication Date |
|---|---|
| WO2015006828A1 true WO2015006828A1 (en) | 2015-01-22 |
| WO2015006828A9 WO2015006828A9 (en) | 2015-03-12 |
Family
ID=52345629
Family Applications (5)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| PCT/AU2014/050131 WO2015006829A1 (en) | 2013-07-17 | 2014-07-17 | A method for treating infection, sepsis and injury |
| PCT/AU2014/050133 WO2015006831A1 (en) | 2013-07-17 | 2014-07-17 | A method for reducing, inflammation, coagulation and adhesions |
| PCT/AU2014/050130 WO2015006828A1 (en) | 2013-07-17 | 2014-07-17 | A method for treating haemorrhage, shock and brain injury |
| PCT/AU2014/050128 WO2015006827A1 (en) | 2013-07-17 | 2014-07-17 | A method for inducing whole body arrest |
| PCT/AU2014/050132 WO2015006830A1 (en) | 2013-07-17 | 2014-07-17 | A method for organ arrest, protection and preservation and reducing tissue injury |
Family Applications Before (2)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| PCT/AU2014/050131 WO2015006829A1 (en) | 2013-07-17 | 2014-07-17 | A method for treating infection, sepsis and injury |
| PCT/AU2014/050133 WO2015006831A1 (en) | 2013-07-17 | 2014-07-17 | A method for reducing, inflammation, coagulation and adhesions |
Family Applications After (2)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| PCT/AU2014/050128 WO2015006827A1 (en) | 2013-07-17 | 2014-07-17 | A method for inducing whole body arrest |
| PCT/AU2014/050132 WO2015006830A1 (en) | 2013-07-17 | 2014-07-17 | A method for organ arrest, protection and preservation and reducing tissue injury |
Country Status (8)
| Country | Link |
|---|---|
| US (3) | US20160166598A1 (en) |
| EP (3) | EP3021854A4 (en) |
| CN (3) | CN105579045A (en) |
| AU (3) | AU2014292827A1 (en) |
| BR (3) | BR112016000809A2 (en) |
| CA (3) | CA2917653A1 (en) |
| MX (3) | MX2016000651A (en) |
| WO (5) | WO2015006829A1 (en) |
Cited By (12)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US9474882B2 (en) | 2013-02-26 | 2016-10-25 | Prytime Medical Devices, Inc. | Fluoroscopy-independent balloon guided occlusion catheter and methods |
| US10111669B2 (en) | 2010-04-21 | 2018-10-30 | The Regents Of The University Of Michigan | Fluoroscopy-independent, endovascular aortic occlusion system |
| US10232142B2 (en) | 2014-06-10 | 2019-03-19 | Prytime Medical Devices, Inc. | Conduit guiding tip |
| US10368872B2 (en) | 2016-06-02 | 2019-08-06 | Prytime Medical Devices, Inc. | System and method for low profile occlusion balloon catheter |
| US10569062B2 (en) | 2013-09-09 | 2020-02-25 | Prytime Medical Devices, Inc. | Low profile occlusion catheter |
| US11135265B2 (en) | 2015-01-30 | 2021-10-05 | Par Pharmaceutical, Inc. | Vasopressin formulations for use in treatment of hypotension |
| US11596411B2 (en) | 2017-04-21 | 2023-03-07 | The Regents Of The University Of California | Aortic flow meter and pump for partial-aortic occlusion |
| US11602592B2 (en) | 2017-01-12 | 2023-03-14 | The Regents Of The University Of California | Endovascular perfusion augmentation for critical care |
| US11633192B2 (en) | 2020-03-16 | 2023-04-25 | Certus Critical Care, Inc. | Blood flow control devices, systems, and methods |
| US11672951B2 (en) | 2015-03-19 | 2023-06-13 | Prytime Medical Devices, Inc. | System and method for low-profile occlusion balloon catheter |
| US12011172B2 (en) | 2018-08-06 | 2024-06-18 | Prytime Medical Devices, Inc. | Occlusion catheter system for full or partial occlusion |
| US12102330B2 (en) | 2021-03-18 | 2024-10-01 | Prytime Medical Devices, Inc. | Vascular occlusion catheter for partial occlusion or full occlusion |
Families Citing this family (35)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| EP3371212B1 (en) * | 2015-11-06 | 2023-10-11 | The Board of Trustees of the University of Illinois | Peptides and method for treatment of cardiac arrest |
| WO2017137528A1 (en) * | 2016-02-12 | 2017-08-17 | Charité - Universitätsmedizin Berlin | Adenosine a1 receptor agonist for use in treatment of status epilepticus |
| US10707531B1 (en) | 2016-09-27 | 2020-07-07 | New Dominion Enterprises Inc. | All-inorganic solvents for electrolytes |
| WO2018226991A1 (en) | 2017-06-07 | 2018-12-13 | Shifamed Holdings, Llc | Intravascular fluid movement devices, systems, and methods of use |
| CN111556763B (en) | 2017-11-13 | 2023-09-01 | 施菲姆德控股有限责任公司 | Intravascular fluid movement device and system |
| WO2019145748A2 (en) * | 2017-12-05 | 2019-08-01 | Neuroindex Ltd. | Systems and methods for anesthesia management |
| EP4085965A1 (en) | 2018-02-01 | 2022-11-09 | Shifamed Holdings, LLC | Intravascular blood pumps and methods of use and manufacture |
| CN108753683B (en) * | 2018-05-26 | 2022-02-15 | 温州医科大学 | Solution system for promoting activity recovery of cryopreserved tissues, organs and cells |
| US12097345B2 (en) | 2018-06-01 | 2024-09-24 | Penumbra, Inc. | Infusion catheter and methods of use |
| WO2020047539A1 (en) * | 2018-08-31 | 2020-03-05 | Louisiana Tech Research Corporation | System and method for network analysis of a patient's neuro-cardio-respiratory system |
| CN110352951A (en) * | 2018-11-15 | 2019-10-22 | 崔磊 | A kind of serum-free is without DMSO tissue engineered bone frozen stock solution and its preparation and cryopreservation methods |
| CN109248173A (en) * | 2018-11-23 | 2019-01-22 | 浙江省人民医院 | A kind of cardioplegic solution |
| EP3893862B1 (en) * | 2018-12-14 | 2023-11-22 | National Taiwan University | A stable cardioplegic solution for cardiac surgery |
| CN113453547B (en) * | 2019-01-10 | 2022-09-20 | 艾克斯维沃控股有限公司 | Apparatus and method for measuring donor heart performance ex vivo |
| EP3946379A4 (en) * | 2019-03-29 | 2023-01-25 | Virginia Commonwealth University | Polymer agents for cardiopulmonary resuscitation |
| CN110057821B (en) * | 2019-04-16 | 2021-09-07 | 上海交通大学 | Low-temperature microscopic imaging system for human gamete rapid freeze-thawing process observation |
| WO2020223462A1 (en) * | 2019-04-30 | 2020-11-05 | University Of Florida Research Foundation, Inc. | Biomarker panel for sepsis encephalopathy |
| JP2022540616A (en) | 2019-07-12 | 2022-09-16 | シファメド・ホールディングス・エルエルシー | Intravascular blood pump and methods of manufacture and use |
| US11654275B2 (en) | 2019-07-22 | 2023-05-23 | Shifamed Holdings, Llc | Intravascular blood pumps with struts and methods of use and manufacture |
| WO2021051064A1 (en) * | 2019-09-12 | 2021-03-18 | The General Hospital Corporation | System and method for determining treatment outcomes for neurological disorders based on functional connectivity parameters |
| WO2021062032A1 (en) * | 2019-09-24 | 2021-04-01 | Penumbra, Inc. | Infusion catheter and methods of use |
| WO2021062270A1 (en) | 2019-09-25 | 2021-04-01 | Shifamed Holdings, Llc | Catheter blood pumps and collapsible pump housings |
| EP4034192A4 (en) | 2019-09-25 | 2023-11-29 | Shifamed Holdings, LLC | Intravascular blood pump systems and methods of use and control thereof |
| CN110692580B (en) * | 2019-11-15 | 2021-11-02 | 苑春亭 | Stichopus japonicus pond capable of going through summer and method for safely going through summer sleeping |
| CN113134116B (en) * | 2020-01-20 | 2022-09-06 | 山东威高宏瑞医学科技有限公司 | Filling composition and filling preparation for endoscopic minimally invasive surgery |
| CN111407244A (en) * | 2020-03-30 | 2020-07-14 | 上海大学 | Left ventricle end-systolic elasticity prediction method and system based on SVR algorithm |
| CN111345293B (en) * | 2020-04-08 | 2021-08-27 | 江门海关技术中心 | Mothproofing agent for insect specimen and preparation method thereof |
| CN111937861B (en) * | 2020-08-17 | 2021-10-26 | 南昌大学第二附属医院 | Sevoflurane ischemia reperfusion device and using method |
| CN112195151B (en) * | 2020-10-28 | 2022-06-21 | 范德里希(上海)生物科技有限公司 | Dental pulp mesenchymal stem cell recovery culture solution, preparation method and recovery culture method |
| CN112826463B (en) * | 2020-12-31 | 2023-11-10 | 苏州爱琴生物医疗电子有限公司 | Blood pressure regulation range determining device and related equipment |
| US20240156355A1 (en) * | 2021-03-18 | 2024-05-16 | Washington University | Hemodilution detector |
| CN113854280B (en) * | 2021-09-06 | 2022-05-31 | 创芯国际生物科技(广州)有限公司 | Low-temperature preservation solution and preparation method and application thereof |
| WO2023154844A2 (en) * | 2022-02-10 | 2023-08-17 | Workman David Henry | Compositions comprising nad+ and associated methods of treatment |
| US20230404066A1 (en) * | 2022-06-15 | 2023-12-21 | Vascular Perfusion Solutions, Inc. | Tissue perfusion and viability sensing system |
| WO2024050139A1 (en) * | 2022-09-02 | 2024-03-07 | AnaBios Corporation | Therapeutic uses of cardiac myosin inhibitors |
Citations (6)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO2000056145A1 (en) | 1999-03-23 | 2000-09-28 | James Cook University | Organ arrest, protection and preservation |
| WO2001045684A2 (en) * | 1999-12-20 | 2001-06-28 | Glaxo Group Limited | Formulations of adenosine a1 agonists |
| US6271228B1 (en) | 2000-04-28 | 2001-08-07 | Pfizer Inc. | Blood pressure stabilization during hemodialysis |
| WO2003082296A1 (en) | 2002-03-28 | 2003-10-09 | Institut De Cardiologie De Montréal / Montréal Heart Institute | Use of methylene blue and related compounds to prevent or reverse an exaggerated hemodynamic reaction |
| WO2008011670A1 (en) | 2006-07-25 | 2008-01-31 | Hibernation Therapeutics Limited | Trauma therapy |
| WO2011075391A1 (en) | 2009-12-15 | 2011-06-23 | Schering Corporation | Formulations of acadesine |
Family Cites Families (58)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US3795581A (en) * | 1971-11-01 | 1974-03-05 | American Hospital Supply Corp | Method of maintaining or restoring the 2,3-diphosphoglycerate content of human red cells |
| US4112070A (en) * | 1977-06-08 | 1978-09-05 | Research Corporation | Blood preservation system |
| SU878297A1 (en) | 1978-05-03 | 1981-11-07 | Научно-Исследовательский Институт Трансплантологии И Искусственных Органов | Composition preserving vitality of heart being operated on |
| US4798824A (en) | 1985-10-03 | 1989-01-17 | Wisconsin Alumni Research Foundation | Perfusate for the preservation of organs |
| US5006512A (en) | 1987-10-02 | 1991-04-09 | Tsuyoshi Ohnishi | Therapeutic usages of inhibitors for a potassium efflux channel |
| US4968675A (en) * | 1988-10-28 | 1990-11-06 | Upjohn | Non-hemolytic lazaroid parenteral formulation |
| US5256770A (en) | 1990-04-09 | 1993-10-26 | Schering Ag | Oxidation resistant thrombomodulin analogs |
| DE3926287A1 (en) | 1989-08-09 | 1991-02-21 | Bernhard Clasbrummel | Use of omega-conotoxin GVIA or its analogues - as pre-synaptic calcium ion antagonists in sympatholytic treatment of circulation disorders of extremities, e.g. hypoxia |
| US5145771A (en) | 1990-04-12 | 1992-09-08 | The University Of North Carolina At Chapel Hill | Rinse solution for organs and tissues |
| US5206222A (en) | 1991-05-22 | 1993-04-27 | Vanderbilt University | Methods for the reduction of myocardial reperfusion injury |
| US5407793A (en) | 1991-10-18 | 1995-04-18 | University Of Pittsburgh Of The Commonwealth System Of Higher Education | An aqueous heart preservation and cardioplegia solution |
| RU2025973C1 (en) | 1992-02-10 | 1995-01-09 | Научно-производственное предприятие "Биофарм" | Solution for conservation of live organs |
| US5370989A (en) | 1992-04-03 | 1994-12-06 | The Trustees Of Columbia University In The City Of New York | Solution for prolonged organ preservation |
| US5405742A (en) * | 1993-07-16 | 1995-04-11 | Cyromedical Sciences, Inc. | Solutions for tissue preservation and bloodless surgery and methods using same |
| EP0762852A4 (en) * | 1994-05-25 | 2000-03-08 | Jerry L Jacobson | Method and apparatus for ameliorating aging process |
| US5679706A (en) | 1994-09-30 | 1997-10-21 | Bristol-Myers Squibb Company | Combination of a potassium channel activator and an antiarrhythmic agent |
| US5554497A (en) | 1994-12-12 | 1996-09-10 | Charlotte-Mecklenburg Hospital Authority | Cardioplegic solution for arresting an organ |
| US5656420A (en) | 1995-02-24 | 1997-08-12 | University Of Kentucky Research Foundation | Method for employing the delta opioid dadle to extend tissue survival time during ischemia |
| WO1997016169A1 (en) * | 1995-11-01 | 1997-05-09 | Chiron Corporation | Treatment of a cardiovascular indication by delivery of therapeutics to the pericardial space |
| JP3875295B2 (en) | 1995-11-30 | 2007-01-31 | 功 竹内 | Myocardial protective fluid |
| US5939394A (en) * | 1996-01-18 | 1999-08-17 | Fleming & Company | Methods and compositions for the prevention and treatment of immunological disorders, inflammatory diseases and infections |
| US6043224A (en) | 1996-09-05 | 2000-03-28 | The Massachusetts Institute Of Technology | Compositions and methods for treatment of neurological disorders and neurodegenerative diseases |
| IT1297886B1 (en) | 1997-02-28 | 1999-12-20 | Carmine Antropoli | NIFEDIPINA FOR TOPICAL USE |
| EP1014995A4 (en) | 1997-06-18 | 2005-02-16 | Aderis Pharmaceuticals Inc | Compositions and methods for preventing restenosis following revascularization procedures |
| CN1057192C (en) | 1997-09-10 | 2000-10-11 | 上海长征医院 | Method for preparing preservation liquid for various kinds of living organs and the prepns. thereof |
| US6011017A (en) | 1998-04-15 | 2000-01-04 | Cypros Pharmaceutical Corp. | Method of reducing pulmonary hypertension and atrial fibrillation after surgery using cardiopulmonary bypass |
| ATE344035T1 (en) | 1998-07-16 | 2006-11-15 | Memorial Sloan Kettering Inst | TOPICAL COMPOSITION CONTAINING AN OPIOID ANALGESIC AND AN NMDA ANTAGONIST |
| AU752255B2 (en) | 1998-10-23 | 2002-09-12 | Polyheal Ltd. | Compositions of microspheres for wound healing |
| US6358208B1 (en) | 1998-11-21 | 2002-03-19 | Philipp Lang | Assessment of cardiovascular performance using ultrasound methods and devices that interrogate interstitial fluid |
| US6586413B2 (en) | 1999-11-05 | 2003-07-01 | The United States Of America As Represented By The Department Of Health And Human Services | Methods and compositions for reducing ischemic injury of the heart by administering adenosine receptor agonists and antagonists |
| US20020006435A1 (en) | 2000-01-27 | 2002-01-17 | Samuels Paul J. | Transdermal anesthetic and vasodilator composition and methods for topical administration |
| JP2001261575A (en) | 2000-03-13 | 2001-09-26 | General Hospital Corp | Method for regulating vasoconstriction and its composition |
| US6569615B1 (en) | 2000-04-10 | 2003-05-27 | The United States Of America As Represented By The Department Of Veteran's Affairs | Composition and methods for tissue preservation |
| IL152473A0 (en) | 2000-04-28 | 2003-05-29 | Sloan Kettering Inst Cancer | Topical anesthetic/opioid formulations and uses thereof |
| WO2002026140A1 (en) | 2000-09-26 | 2002-04-04 | Medtronic, Inc. | Medical method and system for directing blood flow |
| WO2006069170A2 (en) | 2004-12-22 | 2006-06-29 | Emory University | Therapeutic adjuncts to enhance the organ protective effects of postconditioning |
| EP1478660A4 (en) | 2002-01-29 | 2005-02-09 | Cognetix Inc | Kappa-pviia-related conotoxins as organ protectants |
| EP1494685B1 (en) | 2002-04-18 | 2008-12-31 | Cv Therapeutics, Inc. | Method of treating arrhythmias comprising administration of an a1 adenosine agonist with a beta blocker |
| AUPS312602A0 (en) | 2002-06-21 | 2002-07-18 | James Cook University | Organ arrest, protection, preservation and recovery |
| US20040229780A1 (en) | 2002-09-20 | 2004-11-18 | Olivera Baldomero M. | KappaM-conopeptides as organ protectants |
| US6921633B2 (en) | 2002-11-18 | 2005-07-26 | Biolife Solutions Incorporated | Methods and compositions for the preservation of cells, tissues or organs in the vitreous state |
| US20040167226A1 (en) | 2002-12-16 | 2004-08-26 | Serafini Tito A. | Methods for the treatment of pain and traumatic injury using benzamides and compositions containing the same |
| GB2436255B (en) | 2002-12-23 | 2007-11-28 | Global Cardiac Solutions Pty L | Organ preconditioning, arrest, protection, preservation and recovery |
| WO2004056180A1 (en) | 2002-12-23 | 2004-07-08 | Global Cardiac Solutions Pty Ltd | Organ preconditioning, arrest, protection, preservation and recovery (1) |
| US6992075B2 (en) | 2003-04-04 | 2006-01-31 | Barr Laboratories, Inc. | C(14) estrogenic compounds |
| CA2561452A1 (en) | 2003-06-02 | 2004-12-16 | Samaritan Pharmaceuticals, Inc. | Neuroprotective benzoate and benzamide compounds |
| US7049309B2 (en) | 2003-10-14 | 2006-05-23 | Bristol-Myers Squibb Company | 3-Thia-4-arylquinolin-2-one potassium channel modulators |
| WO2007030198A2 (en) | 2005-07-11 | 2007-03-15 | Human Biosystems | Improved methods and solutions for storing donor organs |
| CN101500409A (en) * | 2006-05-29 | 2009-08-05 | 低温药理有限公司 | Improved tissue maintenance |
| WO2007137321A1 (en) | 2006-05-29 | 2007-12-06 | Hibernation Therapeutics Limited | Improved tissue maintenance |
| US20130122108A1 (en) * | 2006-06-06 | 2013-05-16 | Robert G Matheny | Compositions for Regenerating Defective or Absent Myocardium |
| KR20090077066A (en) * | 2006-10-06 | 2009-07-14 | 뉴사우스 이노베이션즈 피티와이 리미티드 | Particle formation |
| US20100119554A1 (en) * | 2007-03-02 | 2010-05-13 | Hibernation Therapeutics Limited | Transplants |
| CN100423638C (en) | 2007-03-22 | 2008-10-08 | 南京吉脉生物技术有限公司 | Organ preserving fluid and its prepn |
| JP2010534208A (en) * | 2007-07-25 | 2010-11-04 | ハイバーネイション セラピューティクス リミテッド | Improved organ protection, preservation and recovery |
| CN101496512A (en) * | 2008-02-01 | 2009-08-05 | 扬子江药业集团上海海尼药业有限公司 | Organ preservative fluid and preparation method thereof |
| US20090198145A1 (en) * | 2008-02-06 | 2009-08-06 | Chow Harrison | Compositions, methods, and systems for rapid induction and maintenance of continuous rem sleep |
| CN102726366B (en) | 2011-04-07 | 2014-06-04 | 中国人民解放军第二军医大学 | Organ preservation solution and method for preparing same |
-
2014
- 2014-07-17 WO PCT/AU2014/050131 patent/WO2015006829A1/en active Application Filing
- 2014-07-17 MX MX2016000651A patent/MX2016000651A/en unknown
- 2014-07-17 CA CA2917653A patent/CA2917653A1/en not_active Abandoned
- 2014-07-17 AU AU2014292827A patent/AU2014292827A1/en not_active Abandoned
- 2014-07-17 MX MX2016000649A patent/MX2016000649A/en unknown
- 2014-07-17 CA CA2917645A patent/CA2917645C/en active Active
- 2014-07-17 EP EP14825914.6A patent/EP3021854A4/en not_active Withdrawn
- 2014-07-17 CN CN201480051003.6A patent/CN105579045A/en active Pending
- 2014-07-17 BR BR112016000809A patent/BR112016000809A2/en not_active Application Discontinuation
- 2014-07-17 BR BR112016000804A patent/BR112016000804A2/en not_active Application Discontinuation
- 2014-07-17 BR BR112016000898A patent/BR112016000898A2/en not_active Application Discontinuation
- 2014-07-17 CN CN201480050992.7A patent/CN105722516A/en active Pending
- 2014-07-17 US US14/905,725 patent/US20160166598A1/en not_active Abandoned
- 2014-07-17 WO PCT/AU2014/050133 patent/WO2015006831A1/en active Application Filing
- 2014-07-17 AU AU2014292826A patent/AU2014292826A1/en not_active Abandoned
- 2014-07-17 WO PCT/AU2014/050130 patent/WO2015006828A1/en active Application Filing
- 2014-07-17 WO PCT/AU2014/050128 patent/WO2015006827A1/en active Application Filing
- 2014-07-17 US US14/905,722 patent/US20160158280A1/en not_active Abandoned
- 2014-07-17 EP EP14826665.3A patent/EP3021855A4/en not_active Withdrawn
- 2014-07-17 AU AU2014292825A patent/AU2014292825A1/en not_active Abandoned
- 2014-07-17 CA CA2917629A patent/CA2917629A1/en not_active Abandoned
- 2014-07-17 WO PCT/AU2014/050132 patent/WO2015006830A1/en active Application Filing
- 2014-07-17 EP EP14827107.5A patent/EP3021856B1/en active Active
- 2014-07-17 MX MX2016000650A patent/MX2016000650A/en unknown
- 2014-07-17 CN CN201480051011.0A patent/CN105705151A/en active Pending
-
2016
- 2016-01-19 US US15/000,727 patent/US10786525B2/en active Active
Patent Citations (6)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO2000056145A1 (en) | 1999-03-23 | 2000-09-28 | James Cook University | Organ arrest, protection and preservation |
| WO2001045684A2 (en) * | 1999-12-20 | 2001-06-28 | Glaxo Group Limited | Formulations of adenosine a1 agonists |
| US6271228B1 (en) | 2000-04-28 | 2001-08-07 | Pfizer Inc. | Blood pressure stabilization during hemodialysis |
| WO2003082296A1 (en) | 2002-03-28 | 2003-10-09 | Institut De Cardiologie De Montréal / Montréal Heart Institute | Use of methylene blue and related compounds to prevent or reverse an exaggerated hemodynamic reaction |
| WO2008011670A1 (en) | 2006-07-25 | 2008-01-31 | Hibernation Therapeutics Limited | Trauma therapy |
| WO2011075391A1 (en) | 2009-12-15 | 2011-06-23 | Schering Corporation | Formulations of acadesine |
Non-Patent Citations (18)
| Title |
|---|
| ASGER GRANFELDT ET AL.: "Adenocaine and Mg2+ reduce fluid requirement to maintain hypotensive resuscitation and improve cardiac and renal function in a porcine model of severe hemorrhagic shock", CRITICAL CARE MEDICINE., vol. 40, 1 November 2012 (2012-11-01), pages 3013 - 3025, XP055337980, doi:10.1097/CCM.0b013e31825fd4ed |
| DI EUSANIO, M. ET AL., J.THORAC CARDIOVASC SURG, vol. 125, 2003, pages 849 - 854 |
| DOBSON, G.P.JONES, M.W.: "Adenosine and Lignocaine: a new concept in nondepolarising surgical arrest, protection and preservation", J. THORACIC CARDIOVAS SURGERY, vol. 127, 2004, pages 794 - 805 |
| GIANGRANDE, P. L. F.: "Historical review: The history of blood transfusion", BRITISH JOURNAL HAEMATOLOGY, vol. 110, no. 4, September 2000 (2000-09-01), pages 758 - 767, XP055309389 * |
| GRANFELDT, A.: "Organ dysfunction following regional and global ischemia/reperfusion. Intervention with Postconditioning and Adenocaine", DANISH MEDICAL JOURNAL, vol. 59, no. 8, August 2012 (2012-08-01), pages B4496 |
| GRANFELDT, A.: "Organ dysfunction following regional and global ischemia/reperfusion. Intervention with Postconditioning and Adenocaine", DANISH MEDICAL JOURNAL, vol. 59, no. 8, August 2012 (2012-08-01), pages B4496, XP055308455 * |
| HAYLEY L. LETSON ET AL.: "Ultra-Small Intravenous Bolus of 7.5% NaCI/Mg2+ With Adenosine and Lidocaine Improves Early Resuscitation Outcome in the Rat After Severe Hemorrhagic Shock In Vivo", JOURNAL OF TRAUMA, vol. 71, 1 September 2011 (2011-09-01), pages 708 - 719, XP055337988, doi:10.1097/TA.0b013e3181fa27c7 |
| KRUGER, T.WEIGAND, E.HOFFMANN, I.BLETTNER, M.AEBERT, H.: "Cerebral Protection During Surgery for Acute Aortic Dissection Type A Results of the German Registry for Acute Aortic Dissection Type A (GERAADA", CIRCULATION, vol. 124, 2011, pages 434 - 443 |
| LETSON, H. L. ET AL.: "Reversal of acute coagulopathy during hypotensive resuscitation using small-volume 7.5% NaCI Adenocaine and Mg2+ in the rat model of severe hemorrhagic shock", CRITICAL CARE MEDICINE, vol. 40, no. 8, August 2012 (2012-08-01), pages 2417 - 2422, XP008181904, doi:10.1097/CCM.0b013e31825334c3 |
| LETSON, H. L. ET AL.: "Reversal of acute coagulopathy during hypotensive resuscitation using small-volume 7.5% NaCl adenocaine and Mg2+ in the rat model of severe hemorrhagic shock", CRITICAL CARE MEDICINE, vol. 40, no. 8, August 2012 (2012-08-01), pages 2417 - 2422, XP008181904 * |
| MALHOTRA, S.P.HANLEY, F.L.: "Routine Continuous Perfusion for Aortic Arch Reconstruction in the Neonate", SEMIN THORAC CARDIOVASC SURG PEDIATR CARD SURG ANN, vol. 11, 2008, pages 57 - 60, XP022589916, doi:10.1053/j.pcsu.2007.12.004 |
| MISFIELD, M.LEONTYEV, S.BORGER, M.A.GINDENSPERGER, O.LEHMANN, S.LEGARE, J.F.MOHR, F.W.: "What is the best strategy for brain protection in patients undergoing aortic arch surgery? A single centre experience of 636 patients", ANN THORAC SURG., vol. 93, 2012, pages 1502 - 1508, XP028418885, doi:10.1016/j.athoracsur.2012.01.106 |
| PAXTON, E.S.BACKUS, J.KEENER, J.BROPHY, R.H.: "Shoulder arthroscopy: basic principles of positioning, anaesthesia, and portal anatomy", J AM ACAD ORTHOP SURG., vol. 21, 2013, pages 332 - 342 |
| SAWYNOK, J. ET AL.: "Antidepressants as analgesics: an overview of central and peripheral mechanisms of action", JOURNAL OF PSYCHIATRY AND NEUROSCIENCE, vol. 26, no. 1, 2001, pages 21 - 29, XP055308456 * |
| See also references of EP3021855A4 |
| SINGH, K.ANDERSON, E.HARPER, J.G.: "Overview and management of sternal wound infection", SEMIN PLAST SURG., vol. 25, 2011, pages 25 - 33 |
| SUNDELACRUZ, S.LEVIN, M.KAPLAN, D.L.: "Role of Membrane Potential in the Regulation 10 of Cell Proliferation and Differentiation", STEM CELL REV AND REP, vol. 5, 2009, pages 231 - 246 |
| TANTRY, T.P.MURALISHANKAR, BADAPPA K.K.BHANDARY, S.SHETTY, P.SHENOY, S.P.: "Target-controlled infusion (Propofol) versus inhaled anaesthetic (Sevoflurane) in patients undergoing shoulder arthroscopic surgery", INDIAN J ANAESTH., vol. 57, 2013, pages 35 - 40 |
Cited By (15)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US10111669B2 (en) | 2010-04-21 | 2018-10-30 | The Regents Of The University Of Michigan | Fluoroscopy-independent, endovascular aortic occlusion system |
| US9474882B2 (en) | 2013-02-26 | 2016-10-25 | Prytime Medical Devices, Inc. | Fluoroscopy-independent balloon guided occlusion catheter and methods |
| US10569062B2 (en) | 2013-09-09 | 2020-02-25 | Prytime Medical Devices, Inc. | Low profile occlusion catheter |
| US10232142B2 (en) | 2014-06-10 | 2019-03-19 | Prytime Medical Devices, Inc. | Conduit guiding tip |
| US11135265B2 (en) | 2015-01-30 | 2021-10-05 | Par Pharmaceutical, Inc. | Vasopressin formulations for use in treatment of hypotension |
| US11207372B2 (en) | 2015-01-30 | 2021-12-28 | Par Pharmaceutical, Inc. | Vasopressin formulations for use in treatment of hypotension |
| US11672951B2 (en) | 2015-03-19 | 2023-06-13 | Prytime Medical Devices, Inc. | System and method for low-profile occlusion balloon catheter |
| US11857737B2 (en) | 2015-03-19 | 2024-01-02 | Prytime Medical Devices, Inc. | System and method for low-profile occlusion balloon catheter |
| US10368872B2 (en) | 2016-06-02 | 2019-08-06 | Prytime Medical Devices, Inc. | System and method for low profile occlusion balloon catheter |
| US11253264B2 (en) | 2016-06-02 | 2022-02-22 | Prytime Medical Devices, Inc. | System and method for low profile occlusion balloon catheter |
| US11602592B2 (en) | 2017-01-12 | 2023-03-14 | The Regents Of The University Of California | Endovascular perfusion augmentation for critical care |
| US11596411B2 (en) | 2017-04-21 | 2023-03-07 | The Regents Of The University Of California | Aortic flow meter and pump for partial-aortic occlusion |
| US12011172B2 (en) | 2018-08-06 | 2024-06-18 | Prytime Medical Devices, Inc. | Occlusion catheter system for full or partial occlusion |
| US11633192B2 (en) | 2020-03-16 | 2023-04-25 | Certus Critical Care, Inc. | Blood flow control devices, systems, and methods |
| US12102330B2 (en) | 2021-03-18 | 2024-10-01 | Prytime Medical Devices, Inc. | Vascular occlusion catheter for partial occlusion or full occlusion |
Also Published As
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| US10786525B2 (en) | Method for treating haemorrhage, shock and brain injury | |
| KR101490836B1 (en) | Trauma therapy | |
| WO2008106724A1 (en) | Transplants | |
| JP2014196351A (en) | Improved organ protection, preservation and recovery | |
| JP2010534208A5 (en) |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| 121 | Ep: the epo has been informed by wipo that ep was designated in this application |
Ref document number: 14826665 Country of ref document: EP Kind code of ref document: A1 |
|
| ENP | Entry into the national phase |
Ref document number: 2917629 Country of ref document: CA |
|
| WWE | Wipo information: entry into national phase |
Ref document number: MX/A/2016/000650 Country of ref document: MX |
|
| NENP | Non-entry into the national phase |
Ref country code: DE |
|
| REG | Reference to national code |
Ref country code: BR Ref legal event code: B01A Ref document number: 112016000804 Country of ref document: BR |
|
| ENP | Entry into the national phase |
Ref document number: 2014292825 Country of ref document: AU Date of ref document: 20140717 Kind code of ref document: A |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 2014826665 Country of ref document: EP |
|
| ENP | Entry into the national phase |
Ref document number: 112016000804 Country of ref document: BR Kind code of ref document: A2 Effective date: 20160114 |