WO2010140117A1 - Method and system for providing behavioural therapy for insomnia - Google Patents
Method and system for providing behavioural therapy for insomnia Download PDFInfo
- Publication number
- WO2010140117A1 WO2010140117A1 PCT/IB2010/052440 IB2010052440W WO2010140117A1 WO 2010140117 A1 WO2010140117 A1 WO 2010140117A1 IB 2010052440 W IB2010052440 W IB 2010052440W WO 2010140117 A1 WO2010140117 A1 WO 2010140117A1
- Authority
- WO
- WIPO (PCT)
- Prior art keywords
- patient
- sleep
- score
- insomnia
- structured
- Prior art date
Links
Classifications
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61B—DIAGNOSIS; SURGERY; IDENTIFICATION
- A61B5/00—Measuring for diagnostic purposes; Identification of persons
- A61B5/103—Detecting, measuring or recording devices for testing the shape, pattern, colour, size or movement of the body or parts thereof, for diagnostic purposes
- A61B5/11—Measuring movement of the entire body or parts thereof, e.g. head or hand tremor, mobility of a limb
- A61B5/1118—Determining activity level
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61B—DIAGNOSIS; SURGERY; IDENTIFICATION
- A61B5/00—Measuring for diagnostic purposes; Identification of persons
- A61B5/02—Detecting, measuring or recording pulse, heart rate, blood pressure or blood flow; Combined pulse/heart-rate/blood pressure determination; Evaluating a cardiovascular condition not otherwise provided for, e.g. using combinations of techniques provided for in this group with electrocardiography or electroauscultation; Heart catheters for measuring blood pressure
- A61B5/0205—Simultaneously evaluating both cardiovascular conditions and different types of body conditions, e.g. heart and respiratory condition
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61B—DIAGNOSIS; SURGERY; IDENTIFICATION
- A61B5/00—Measuring for diagnostic purposes; Identification of persons
- A61B5/103—Detecting, measuring or recording devices for testing the shape, pattern, colour, size or movement of the body or parts thereof, for diagnostic purposes
- A61B5/11—Measuring movement of the entire body or parts thereof, e.g. head or hand tremor, mobility of a limb
- A61B5/113—Measuring movement of the entire body or parts thereof, e.g. head or hand tremor, mobility of a limb occurring during breathing
- A61B5/1135—Measuring movement of the entire body or parts thereof, e.g. head or hand tremor, mobility of a limb occurring during breathing by monitoring thoracic expansion
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61B—DIAGNOSIS; SURGERY; IDENTIFICATION
- A61B5/00—Measuring for diagnostic purposes; Identification of persons
- A61B5/24—Detecting, measuring or recording bioelectric or biomagnetic signals of the body or parts thereof
- A61B5/316—Modalities, i.e. specific diagnostic methods
- A61B5/318—Heart-related electrical modalities, e.g. electrocardiography [ECG]
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61B—DIAGNOSIS; SURGERY; IDENTIFICATION
- A61B5/00—Measuring for diagnostic purposes; Identification of persons
- A61B5/48—Other medical applications
- A61B5/4806—Sleep evaluation
- A61B5/4809—Sleep detection, i.e. determining whether a subject is asleep or not
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61B—DIAGNOSIS; SURGERY; IDENTIFICATION
- A61B5/00—Measuring for diagnostic purposes; Identification of persons
- A61B5/48—Other medical applications
- A61B5/4806—Sleep evaluation
- A61B5/4812—Detecting sleep stages or cycles
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61B—DIAGNOSIS; SURGERY; IDENTIFICATION
- A61B5/00—Measuring for diagnostic purposes; Identification of persons
- A61B5/68—Arrangements of detecting, measuring or recording means, e.g. sensors, in relation to patient
- A61B5/6801—Arrangements of detecting, measuring or recording means, e.g. sensors, in relation to patient specially adapted to be attached to or worn on the body surface
- A61B5/6802—Sensor mounted on worn items
- A61B5/6804—Garments; Clothes
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61B—DIAGNOSIS; SURGERY; IDENTIFICATION
- A61B5/00—Measuring for diagnostic purposes; Identification of persons
- A61B5/68—Arrangements of detecting, measuring or recording means, e.g. sensors, in relation to patient
- A61B5/6887—Arrangements of detecting, measuring or recording means, e.g. sensors, in relation to patient mounted on external non-worn devices, e.g. non-medical devices
-
- G—PHYSICS
- G09—EDUCATION; CRYPTOGRAPHY; DISPLAY; ADVERTISING; SEALS
- G09B—EDUCATIONAL OR DEMONSTRATION APPLIANCES; APPLIANCES FOR TEACHING, OR COMMUNICATING WITH, THE BLIND, DEAF OR MUTE; MODELS; PLANETARIA; GLOBES; MAPS; DIAGRAMS
- G09B19/00—Teaching not covered by other main groups of this subclass
-
- G—PHYSICS
- G16—INFORMATION AND COMMUNICATION TECHNOLOGY [ICT] SPECIALLY ADAPTED FOR SPECIFIC APPLICATION FIELDS
- G16H—HEALTHCARE INFORMATICS, i.e. INFORMATION AND COMMUNICATION TECHNOLOGY [ICT] SPECIALLY ADAPTED FOR THE HANDLING OR PROCESSING OF MEDICAL OR HEALTHCARE DATA
- G16H20/00—ICT specially adapted for therapies or health-improving plans, e.g. for handling prescriptions, for steering therapy or for monitoring patient compliance
- G16H20/70—ICT specially adapted for therapies or health-improving plans, e.g. for handling prescriptions, for steering therapy or for monitoring patient compliance relating to mental therapies, e.g. psychological therapy or autogenous training
-
- G—PHYSICS
- G16—INFORMATION AND COMMUNICATION TECHNOLOGY [ICT] SPECIALLY ADAPTED FOR SPECIFIC APPLICATION FIELDS
- G16H—HEALTHCARE INFORMATICS, i.e. INFORMATION AND COMMUNICATION TECHNOLOGY [ICT] SPECIALLY ADAPTED FOR THE HANDLING OR PROCESSING OF MEDICAL OR HEALTHCARE DATA
- G16H50/00—ICT specially adapted for medical diagnosis, medical simulation or medical data mining; ICT specially adapted for detecting, monitoring or modelling epidemics or pandemics
- G16H50/20—ICT specially adapted for medical diagnosis, medical simulation or medical data mining; ICT specially adapted for detecting, monitoring or modelling epidemics or pandemics for computer-aided diagnosis, e.g. based on medical expert systems
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61B—DIAGNOSIS; SURGERY; IDENTIFICATION
- A61B5/00—Measuring for diagnostic purposes; Identification of persons
- A61B5/48—Other medical applications
- A61B5/4806—Sleep evaluation
- A61B5/4815—Sleep quality
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61B—DIAGNOSIS; SURGERY; IDENTIFICATION
- A61B5/00—Measuring for diagnostic purposes; Identification of persons
- A61B5/72—Signal processing specially adapted for physiological signals or for diagnostic purposes
- A61B5/7235—Details of waveform analysis
- A61B5/7264—Classification of physiological signals or data, e.g. using neural networks, statistical classifiers, expert systems or fuzzy systems
- A61B5/7267—Classification of physiological signals or data, e.g. using neural networks, statistical classifiers, expert systems or fuzzy systems involving training the classification device
-
- Y—GENERAL TAGGING OF NEW TECHNOLOGICAL DEVELOPMENTS; GENERAL TAGGING OF CROSS-SECTIONAL TECHNOLOGIES SPANNING OVER SEVERAL SECTIONS OF THE IPC; TECHNICAL SUBJECTS COVERED BY FORMER USPC CROSS-REFERENCE ART COLLECTIONS [XRACs] AND DIGESTS
- Y02—TECHNOLOGIES OR APPLICATIONS FOR MITIGATION OR ADAPTATION AGAINST CLIMATE CHANGE
- Y02A—TECHNOLOGIES FOR ADAPTATION TO CLIMATE CHANGE
- Y02A90/00—Technologies having an indirect contribution to adaptation to climate change
- Y02A90/10—Information and communication technologies [ICT] supporting adaptation to climate change, e.g. for weather forecasting or climate simulation
Definitions
- Patent Application Serial No. 61/184,165 filed June 4, 2009 entitled “System and Method for Managing Insomnia.”
- the invention relates to a system and associated method structured to facilitate cognitive behavioral therapy for a patient having insomnia.
- Sleep disorders are common. At least 10% of the population suffers from a sleep disorder that is clinically significant and of public health importance. Insomnia is by far the most common form of sleep disturbance.
- insomnia definitions include descriptions of sleep-specific symptoms with associated daytime complaints.
- Sleep symptoms typically include a difficulty initiating sleep, difficulty maintaining sleep, final awakening that occurs much earlier than desired or sleep that is non-restorative or of generally poor quality. Waking symptoms are associated with daytime complaints related to fatigue, sleepiness, mood disturbance, cognitive difficulties and social or occupational impairment.
- insomnia is treated by medication.
- the market for sleeping pills is about 4.6B US$.
- Other forms of treatment such as sleep restriction therapy are less wide-spread although evidence suggests that they are more effective on the long run than pharmaceutical treatment alone.
- a standard diagnostic method for assessing the nature and the severity of the sleep problem a so-called sleep log or sleep diary, i.e. a questionnaire usually on paper, is used in most cases; also an actigraph can be used as an alternative to a sleep log.
- the main drawback of this sleep log is that its accuracy is affected by a subjective bias of the patient, e.g. for patients it is often difficult to remember sleep and wake periods during the night correctly.
- U.S. Patent Application Publication No. 2004/0225179 discloses automated behavioral methods and systems for treating insomnia that use passive means for determining wake/sleep states and is incorporated herein by reference.
- Insomnia is a prevalent sleep disturbance in the general population.
- patients tend to not seek treatment or are diagnosed by a non sleep specialist, e.g. a GP, without the use of a standard and proper method for assessing the nature and the severity of the sleep problem. This usually results in the underestimation of the reality of the sleep problem and/or the prescription of sleeping pills, although a drug-free therapy - the cognitive behavioural therapy for insomnia (CBT-I) - has been shown to be as effective and more sustainable. Further, a more accurate assessment and a tailored therapy may lead to a higher compliance and consequently to a better medical outcome.
- CBT-I cognitive behavioural therapy for insomnia
- An object of the disclosed concept is to provide a system structured to facilitate cognitive behavioral therapy for a patient having insomnia, the system including a communication assembly structured to provide for electronic communication, a sensor system having at least one sensor, the sensor system structured to detect sleeping activity data and to provide a sensor system signal incorporating the sleeping activity data, the sensor system coupled to, and in electronic communication with, the communication assembly, a first processing unit coupled to, and in electronic communication with, the communication assembly, the first processing unit structured to receive the sensor system signal and to convert the sleeping activity data into sleep pattern data, a second processing unit having an input assembly and structured to gather patient input data, the second processing unit coupled to, and in electronic communication with, the communication assembly, a third processing unit coupled to, and in electronic communication with, the communication assembly, the third processing unit structured to receive the sleep pattern data and the patient input data, perform an analysis thereon thereby creating a patient sleep profile, a fourth processing unit coupled to, and in electronic communication with, the communication assembly, the fourth processing unit structured to analyze the patient sleep profile and to provide a course of therapy related to
- a further object of the disclosed concept is to provide a method of providing cognitive behavioral therapy for insomnia, the method including the steps of monitoring a patient's sleep utilizing a sensor system having at least one unobtrusive sensor, the sensor system structured to detect sleeping activity data, gathering patient input data, combining the patient input data and the sleeping activity data to create a patient sleep profile, analyzing a patient's sleep profile to determine a course of therapy, and presenting the course of therapy to the patient on a display.
- the term “patient” does not only apply on human beings, but also on animals. Further, the term “patient” does not mean that the respective person/animal is disease ridden, thus, also healthy people will be referred to as “patients.”
- the term “sleep/wake classification” refers to the classification of the epoch of interest as “wake” or “sleep,” resulting from the probability of belonging to the respective class, or the classification "true” or “false” given as an output of the classifier but also refers to the display of the classifier results on a user interface or any device.
- the term “pNN50” refers to the percentage of the number of interval differences of adjacent NN-Intervals greater than 50 ms
- the term “SDNN” refers to the standard deviation of all NN-Intervals
- the term “SDSD” refers to the Standard deviation between distances between adjacent intervals
- the term “RR mean” refers to mean duration of the RR-Intervals
- the term “HR mean” refers to the mean heart rate
- LF refers to the low frequency range, as defined by heart rate variability standards
- the term “HF” refers to the high frequency range, as defined by heart rate variability standards
- the term “RMSSD” refers to root mean square successive differences
- the term “HRV” refers to heart rate variability.
- FIG. 1 schematically shows the general principle of the invention
- FIG. 2 shows a schematic flowchart of the feature extraction method of a first preferred embodiment of the invention
- FIG. 3 shows a schematic flowchart of the sleep/wake classification method of a first preferred embodiment of the invention
- Fig. 4 shows the sleep restriction algorithm based on the method of the present invention
- FIG. 5 schematically shows the elements of the invention
- FIG. 6 shows a schematic flowchart of the method of providing cognitive behavioral therapy for insomnia
- Fig. 7 shows a schematic flowchart related to the sleep scheduling module
- FIG. 8 shows a schematic flowchart related to the association bed-sleep module
- FIG. 9 shows a schematic flowchart related to the cognitive restructuring module
- Fig. 10 shows a schematic flowchart related to the coping strategy module
- Fig. 11 shows a schematic flowchart related to the relaxation module
- Fig. 12 shows a schematic flowchart related to the lifestyle module.
- the system for sleep/wake classification 100 comprises unobtrusive in- bed sensors for vital body sign monitoring 101 of the heart activity from the ECG, and/or the body movements from a bed foil sensor or the like as will be described in the following.
- a further step is the pre-processing unit 102 for filtering and artifact removal during preparation of the signals, a feature extraction unit 103 extracting in particular features from the ECG and/or the body movements signal alone or in combination, then there is a sleep/wake classifier unit 104 for classification of the sleep /wake status according to all the input features, sleep efficiency calculation unit 105 for calculating the time asleep compared to the time in bed, used as input for the patient sleep restriction algorithm, device 106 providing, for example, rules for a healthier sleep to the patient.
- the output of the sleep/wake classification 104, sleep efficiency calculation 105 and sleep restriction algorithm device 106 can be used to provide feedback to the patient 107 or to the medical professional, who could also get information from additional sources like the sleep log questions for subjective parameters 109.
- the sensor is a ferro-electret foil placed underneath the patient's thorax to measure heart rate, respiration and body movements.
- a piezo-resistive strain gauge glued onto a slat underneath the mattress in the patient's thorax region can be used to measure heart rate, respiration and body movements.
- ECG preferably a textile ECG integrated as a pillow and foot mat electrode in the bed.
- the ECG sensor could be combined with a respiration signal, measured with a standard (inductive or piezo- resistive) band around the thorax and/or the abdomen.
- This type of sensor can be also integrated into textiles (e.g. a T-shirt) to make it more unobtrusive.
- the ECG sensor could be combined with an accelerometer signal.
- the device can be a wrist-worn device, but preferably a 2D or 3D accelerometer is placed on the patient's trunk to measure body movements. Also, this type of sensor can be integrated into textiles (e.g. a T-shirt) to make it more unobtrusive.
- the processing unit comprises several steps as can be seen in Figure 1. These are the preprocessing of the raw data, feature extraction and the sleep/wake classification. In the following paragraphs the different alternatives for each of these steps will be described in more detail.
- the signal pre-processing device 102 of Figure 1 includes one or more of the following steps which can be passed through serially, parallel or repeatedly: appropriate filtering of the signal(s); and artifact removal.
- the feature extraction device 103 includes extraction of features from the ECG and a respiration signal comprising:
- the following features are derived: statistical heart rate variability parameters from the time domain (e.g. mean heart rate, SDNN, RMSSD etc.); parameters from the heart rate variability (HRV) spectrum (e.g. LF, HF); multi-scale sample entropy; and progressive detrended fluctuation analysis.
- HRV heart rate variability
- the slat sensor or the inductive/piezo-resistive band - the spectrum is calculated and the LF and HF power are extracted as features.
- the mean breathing rate is determined.
- the feature extraction device 103 allows in case of both, the ECG signal and a respiration signal are available, to calculate the coherent power of both spectra as an additional feature.
- the ratio of heart rate and breathing rate can be derived as an additional feature.
- an activity index is derived based on large body movements.
- the preferred embodiment of the present invention further suggests that for the next step - the sleep/wake classification 104 - the activity index and at least one additional feature relating to the cardiac and/or respiratory status are a preferable combination as input for the classification process.
- a vector, of at least one feature, and preferably all or at least a sub-set of the above-mentioned features is generated for each epoch of interest, e.g. each 1 -minute segment of data.
- this vector is fed into a sleep/wake classifier 104 which is based on a standard pattern recognition approach with supervised learning, as will be described in Figure 3.
- the following approaches can preferably be used: Bayesian linear or quadratic discriminant classifier; support vector machine; k-Nearest-Neighbour (kNN) method; Neural Network; and Hidden Markov Model.
- the parameters of the classifier are trained on a large database of representative data.
- the input unit and the display unit are preferably combined in the preferred embodiment of the present invention in one user interface device 107.
- This device can be a normal laptop PC, a tablet PC with a touch screen, a handheld device such as a PDA or a mobile phone.
- the processing unit can also be part of this device.
- the feedback to the patient can contain one or more of the following parameters: time in bed, total sleep time, total wake time, sleep efficiency, sleep latency, number and durations of awakenings, or a simplified hypnogram.
- the feedback to the medical professional can be given via the same user interface 108.
- the patient's data can be (automatically) sent to the physician via the Internet or GSM, UMTS, EDGE, GPRS, or any other Internet or mobile phone standard or system.
- the feedback to the medical professional should contain all of the above- mentioned parameters. Furthermore, it should also contain the patient's answers to the subjective sleep log questions so that he can compare the subjective and objective data which gives him important information for the appropriate therapy approach. This is, for example, especially important in case of sleep-state misperception, a type of insomnia where objective sleep data reflect a normal sleep pattern but the patient himself does not recognize that he has slept.
- the ECG signal provided by an ECG sensor 200 undergoes a pre-processing 201, wherein the preprocessing consists in R-peak detection, ectopic beat removal, linear interpolation and resampling at a predefined frequency, preferably at 4 Hz.
- the resulting RR-interval series is then considered and heart rate variability parameters, according to the standard, are assessed in frequency and time domains.
- the power spectral estimation is updated on a shorter time scale, e.g. every new detected R-peak of the ECG.
- pNN50 percentage of the number of interval differences of adjacent NN-Intervals greater than 50 ms
- SDNN standard deviation of all NN- Intervals
- SDSD standard deviation of successive differences between adjacent intervals
- RMSSD root mean square successive differences
- RR mean mean duration of the RR-Intervals
- HR mean mean of the instantaneous heart rate
- Non-linear parameters are also extracted from the RR-interval time series in 206 by the application of two methods.
- the first non-linear calculation method used in 207 is progressive detrended fluctuation analysis which allows to gradually integrate the signal before detrending over windows of length 64. Further, the partial sums of the squared signal are then considered and this provides the resulting differentiated time series in 208 from which we extract a new feature 209, defined as the maximum value over the considered epoch, preferably a one-minute epoch but which can be any predefined epoch duration.
- the second non-linear calculation method applied to the RR-interval series provides the multiscale sample entropy.
- the series is coarse-grained at scales 1 and 2 in 210 and 5-minute segments are considered.
- the bed foil signal provided by bed foil sensor 213 is undergoing a pre-processing 214 which consists of noise reduction and calibration.
- the use of low pass filtering 215 leads to the breathing signal. Peak identification on this signal allows to deduce the breath interval series, which is also linearly interpolated and resampled at a predefined rate, preferably at 4 Hz in 216.
- the power spectrum 217 is computed using preferably an autoregressive model with advanced detrending.
- the power spectrum is then split and normalized in 218 in the low- frequency band LF (0.04-0.15 Hz) and in the high frequency band HF (0.15-0.4 Hz), which are used to define the spectral features LF norm respi and LF/HF ratio respi.
- the detection of small and large energy artefacts in 219 allows to define a heuristic activity index over one-minute epochs, also used as a feature in 220.
- the band-pass filtering in 221 delivers the so-called ballistocardiogram, which represents the mechanical heart activity. This signal could be an interesting alternative to the ECG signal to get the heart rate variability signal.
- the RR-interval and the breath interval series are combined in 222 by estimating the squared coherence function over 5- minute epochs centred on the one-minute epoch of interest.
- This coherence function is multiplied by the autospectrum of the RR-interval series and integrated along the frequency axis.
- the resulting feature in 223 is the amount of coherent power in %.
- a preferred embodiment contains the features 203, 205, 209, 212, 223, 218, 220, which form the components of the feature vector used in the classification process which is further described in Figure 3.
- Figure 3 is a preferred embodiment of the method for sleep/wake classification.
- Step 303 represents information coming from the feature extraction process providing a vector with at least one element, which belongs to the test data set.
- the decision is based on a supervised learning classifier 301, which is trained with a training data set 302.
- the classifier 304 decides on the basis of a Bayesian linear or quadratic discriminant classifier, a support vector machine or the k-Nearest-Neighbour (kNN) classifier and with a supervised learning approach based on the training data set, whether the patient is awake or asleep. The more representative the training data are, the better the accuracy and performance of classification 304.
- the sleep restriction therapy is a non-pharmacological method that can be used to treat insomnia either alone or in combination with pharmacological treatment. There is a natural tendency among poor sleepers to increase the amount of time spent in bed in an effort to provide more opportunity for sleep, a strategy that is more likely to result in fragmented and poor quality sleep.
- the sleep restriction therapy consists of curtailing the amount of time spent in bed to the actual amount of time asleep. Time in bed is subsequently adjusted on the basis of the sleep efficiency calculation for a given period of time, which is usually the preceding week. For example, if a person reports sleeping an average of 6 hours per night out of 8 hours spent in bed, the initial prescribed sleep window would be 6 hours.
- step 401 the medical practitioner initializes wake-up-time and go-to- bed time.
- step 402 data is collected for five days, which also includes information from questionnaires.
- step 403 the mean sleep efficiency of the last five days is calculated.
- 404 a case decision is made, deciding whether the mean sleep efficiency is lower than 80%, 80 to 90% or greater than 90%.
- step 406 the patient is asked to shorten the time in bed by 15 minutes, in case the mean sleep efficiency is greater than 90 %, in step 405 the patient is asked to prolong time in bed by 15 minutes.
- step 402 the collection of sleep information for the next five days.
- step 407 positive feedback is given to the patient and in step 408 the wake -up-time and the go-to-bed time will be kept for one more day and the process continues at step 403.
- the disclosed concept may also be identified as a system 1000 structured to facilitate cognitive behavioral therapy for a patient having insomnia and may utilize the method set forth below. Prior to discussing the system 1000 and method, the following definitions are noted.
- unobtrusive sensor means a sensor that is either not attached directly to the patient's body, e.g. by an adhesive, or is wireless.
- a sensor that is not coupled to the patient's body includes, for example, a ferro-electret foil disposed immediately adjacent, or in contact with, the patient's thorax is an "unobtrusive sensor” because it is not attached to the patient and the patient may move freely.
- Other “unobtrusive sensors” include a piezoresistive strain gage coupled to the patient's bed, an ECG sensor embedded in fabric, e.g. a pillow, bedding, pajamas, nightcap or a radar/video system structured to detect movement.
- An "unobtrusive sensor” that may be coupled to the patient's body includes any small/light sensor that may be installed on a bracelet or similar construct.
- One example of such an unobtrusive sensor is an accelerometer. Any sensor that has a wire extending between the patient and a device is not an “unobtrusive sensor.”
- “sleeping activity data” is data, and preferably biometric data, representing a measurable action, whether voluntary or involuntary, that is an indication of a patient's state of consciousness, i.e. asleep or awake.
- the "points" associated with questions (1) and (2) may be combined through simple addition, whereas the "points," e.g. number of cups of coffee consumed, may be a multiplier.
- the final combined score for an assessment is typically compared to one or more predetermined threshold values associated with that assessment. For example, one assessment may determine the level or severity of the patient's insomnia and another assessment may determine the type of insomnia associated with the patient.
- Named assessments include, but are not limited to: Epworth Sleepiness Scale (ESS), Pre-Sleep Arousal Scale, Sleep Disturbance Questionnaire, Sleep Hygiene Practice Scale, Caffeine Knowledge Quiz, The Sleep Behavior Self-Rating Scale, The Glasgow Content of Thoughts Inventory, The Glasgow Sleep Effort Scale, Pittsburgh Sleep Quality Index (PSQI), and the Multidimensional Fatigue Inventory (MFI).
- ESS Epworth Sleepiness Scale
- Pre-Sleep Arousal Scale Pre-Sleep Arousal Scale
- Sleep Disturbance Questionnaire Sleep Hygiene Practice Scale
- Caffeine Knowledge Quiz The Sleep Behavior Self-Rating Scale
- the Glasgow Content of Thoughts Inventory The Glasgow Sleep Effort Scale, Pittsburgh Sleep Quality Index (PSQI), and the Multidimensional Fatigue Inventory (MFI).
- PSQI Pittsburgh Sleep Quality Index
- MFI Multidimensional Fatigue Inventory
- a “threshold value” may also be a range of values. That is, a
- threshold value may exist as a maximum value, a minimum value, or a range of (un)acceptable values.
- the system 1000 structured to facilitate cognitive behavioral therapy for a patient having insomnia includes a communication assembly 1002, a sensor system 1004, a first processing unit 1006, second processing unit 1008, third processing unit 1010, a fourth processing unit 1012, and a display 1014.
- the communication assembly 1002 is structured to provide for electronic communication between the components identified above. That is, each component is coupled to, and in electrical communication with, the communication assembly 1002.
- the communication assembly 1002 and the components may be wirelessly coupled to the various components.
- the communication assembly 1002 is preferably coupled to, and in electrical communication with, an electronic communication network 1001, such as, but not limited to, the Internet.
- the sensor system 1004 has at least one sensor 1020.
- the sensor system 1004 is structured to detect sleeping activity data and to provide a sensor system signal incorporating the sleeping activity data.
- “sleeping activity data” includes at least, heart rate data, respiratory rate data and patient body movement data.
- data from such sensors 1020 e.g. motion data detected by an actigraph and heart rate data detected by an ECG, may be combined to determine, or estimate, if the patient is awake or asleep.
- the ECG sensor associated with the disclosed method is an unobtrusive sensor, i.e.
- sensors that may be used include, but are not limited to inductance plethysmography sensors structured to detect respiratory effort and Emfit foil, structured to measure ballistocardiography (cardiac activity, respiratory activity and body motion activity).
- the sensor system 1004 that is each at least one sensor 1020, is coupled to, and in electronic communication with, the communication assembly 1002.
- Each at least one sensor 1020 is an unobtrusive sensor structured to produce a sensor signal having at least one feature, as set forth above.
- the at least one sensor 1020 may be, but is not limited to, an ECG sensor 1022 and/or an actigraph sensor 1024.
- the ECG sensor 1022 is structured to detect heart rate data and respiratory rate data.
- the heart rate data and respiratory rate data being a feature incorporated into an ECG sensor 1022 signal.
- the actigraph sensor 1024 is structured to detect patient body movement data.
- the patient body movement data being a feature incorporated into an actigraph sensor 1024 signal. Specific types of the at least one sensor 1020 are discussed above.
- the at least one sensor 1020 may be a single accelero meter, a single actigraph, etc.
- Each processing unit i.e. the first, second, third and fourth processing units
- each processing unit 1006, 1008, 1010, 1012 each include operational elements such as, but not limited to, a programmable logic circuit (PLC) and a communication system (neither shown), as is known in the art.
- the operational elements of each processing unit 1006, 1008, 1010, 1012 may also include a memory device (not shown) such as, but not limited to, random access memory (RAM), read-only memory (ROM), flash memory, and/or a hard drive, which may be a disk or solid state.
- the memory device is structured to store one or more sets of executable instructions, hereinafter routines 1030, as well as collected data, other data provided with the routines 1030, and data downloaded via the electronic communication network 1001.
- any data stored on each processing unit 1006, 1008, 1010, 1012 may be communicated to a remote location, such as, but not limited to a medical professional's office, via the communication assembly 1002 and electronic communication network 1001.
- data and/or routines 1030 may be downloaded to each processing unit 1006, 1008, 1010, 1012 from a remote location, such as, but not limited to a medical professional's office, via the communication assembly 1002 and electronic communication network 1001. It is understood that the operational elements of each processing unit 1006, 1008, 1010, 1012 operate cooperatively to perform any function that the processing unit is structured to accomplish.
- each processing unit 1006, 1008, 1010, 1012 are preferably disposed in a housing (shown schematically).
- the operational elements of two or more processing units 1006, 1008, 1010, 1012 may be disposed in a shared housing (not shown) and may operate cooperatively. That is, for example, routines 1030 for each processing unit 1006, 1008, 1010, 1012 may be stored on a single storage device.
- At least one processing unit 1006, 1008, 1010, 1012 has a PLC that is not a general purpose PLC.
- the first processing unit's 1006 PLC is not a general purpose PLC.
- the first processing unit 1006 corresponds to the pre-processing unit 102 described above. That is, the first processing unit 1006 is structured to perform the steps associated with the pre-processing unit 102 described above.
- the first processing unit 1006 is coupled to, and in electronic communication with, the communication assembly 1002.
- the first processing unit 1006 is structured to receive sensor system signal, via the communication assembly 1002, and to convert the sleeping activity data into sleep pattern data.
- Sleep pattern data includes a patient's time in bed, a patient's total sleep time, a patient's total wake time, a patient's sleep efficiency, a patient's sleep onset latency, a patient's awakenings after sleep onset and a patient's snooze time.
- time in bed means the time the patient spends in bed, whether asleep or awake.
- total sleep time is that portion of the time in bed that the patient is asleep.
- sleep onset latency is the time between the patient getting into bed and first falling asleep.
- wake after sleep onset is that portion of the time in bed that the patient is awake from the first time he/she fell asleep to the moment he/she finally woke up in the morning.
- snooze time is the duration from the final awakening to the time when the patient gets out of bed.
- total wake time is that portion of the time in bed that the patient is awake.
- the first processing unit 1006 is structured to process the heart rate data, respiratory rate data, and patient body movement data to determine at least one of the patient's time in bed, the patient's total sleep time, the patient's total wake time, the patient's sleep efficiency, the patient's sleep onset latency, the patient's awakenings after sleep onset and the patient's snooze time.
- the second processing unit 1008 corresponds to the user interface device 107 described above. That is, the second processing unit 1008 is structured to perform the steps associated with the user interface device 107 described above.
- the second processing unit 1008, preferably, includes the display 1014.
- the second processing unit 1008 includes a routine 1030 that is structured to present the user interface 108 on the display 1014.
- the second processing unit 1008, preferably, includes an input assembly 1034 having one or more input devices such as, but not limited to, a keyboard 1036 and a mouse 1038 (or trackball, or touch screen, or any other device that provides a mouse-like functionality).
- the patient may enter patient input data via the input assembly 1034 and the user interface 108.
- the user interface 108 is structured to present one or more assessments, discussed below, and to allow the user to input data into a sleep log.
- the second processing unit 1008 is coupled to, and in electronic communication with, the communication assembly 1002.
- the third processing unit 1010 corresponds to the feature extraction unit 103, the sleep/wake classifier unit 104 and the sleep efficiency calculation unit 106 described above. That is, the third processing unit 1010 is structured to perform the steps associated with the feature extraction unit 103, the sleep/wake classifier unit 104 and the sleep efficiency calculation unit 106 described above.
- the third processing unit 1010 is coupled to, and in electronic communication with, the communication assembly 1002.
- the third processing unit 1010 is structured to receive the sleep pattern data and the patient input data, via the communication assembly 1002, and to perform an analysis thereon. The analysis creates a patient sleep profile.
- a "patient sleep profile" is a collection of data including objective data, such as the patient body movement data, and subjective data, such as the patient input data.
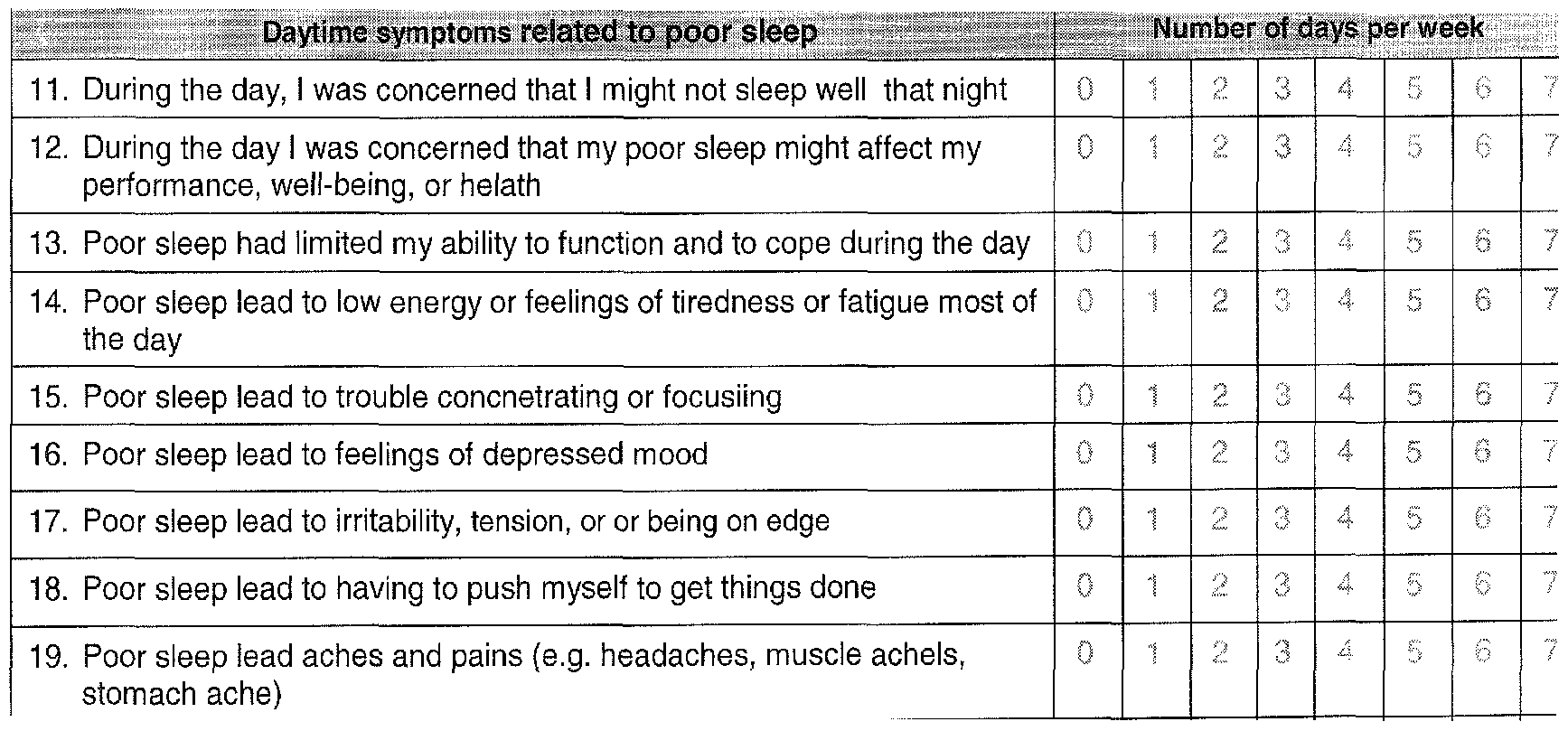
- the patient sleep profile includes the patient's sleep history, sleep patterns, qualitative and quantitative measures of insomnia, identification of insomnia-related factors and identification of daytime consequences of insomnia.
- Daytime consequences of insomnia include, but are not limited to, poor daytime energy, poor cognitive functioning (e.g. concentration, focus, attention, and memory) and poor mood and motivation.
- a qualitative measure of insomnia includes, but is not limited to, a subjective estimation of sleep quality e.g. poor to excellent or as on a Likert scale of 1 to 10.
- a quantitative measure of insomnia includes, but is not limited to, the Insomnia Severity Index (ISI) score, discussed in detail below, subjective and objective estimates of Sleep Onset Latency, Wake After Sleep Onset, and Snooze time.
- ISI Insomnia Severity Index
- Such quantitative measures of insomnia may be compared to a standard threshold, e.g. the Sleep Onset Latency threshold is set to 30 minutes. Such a comparison may be used to assess the type of sleep disturbance (problem with sleep initiation, sleep maintenance or early awakenings, etc.).
- subjective and objective estimates of Sleep Efficiency may be compared to standard thresholds (e.g. 90%) to assess whether or not the patient sleeps in a consolidated way.
- the third processing unit 1010 is structured to send the sleep pattern data, the patient input data and the patient sleep profile to a medical professional via the electronic communications network 1001.
- the fourth processing unit 1012 corresponds to the sleep restriction algorithm device 106 described above. That is, the fourth processing unit 1012 is structured to perform the steps associated with the sleep restriction algorithm device 106 described above.
- the fourth processing unit 1012 is coupled to, and in electronic communication with, the communication assembly 1002.
- the fourth processing unit is structured to analyze the patient sleep profile. The analysis performed by the fourth processing unit 1012 is discussed below.
- the fourth processing unit 1012 is further structured to provide a course of therapy related to the patient sleep profile. That is, the fourth processing unit 1012 includes a memory device 1050 having stored thereon a plurality of interactive therapeutic instruction modules 1060, 1062, 1064, 1066, 1068, 1070.
- the therapeutic instruction modules 1060, 1062, 1064, 1066, 1068, 1070 are, generally, associated with insomnia related factors.
- Insomnia related factors include, but are not limited to behavioral and cognitive factors.
- behavioral factors include, but are not limited to, sleep restriction, scheduling of bedtime and wake time.
- Behavioral factors may note a change in the patient's pattern, irregular sleep/wake times and/or when a patient enters in a compensatory strategy, e.g. going to bed earlier and/or sleeping in and/or napping so as to compensate for a bad night's sleep.
- Behavioral factors also include stimulus control, i.e. association of bed-sleep or when the conditioning between bed and sleep ceases.
- bed and bedtime become cues for activity rather than cues for sleep.
- the patient may lie awake in bed, which confuses the connection in the brain between bed and sleep and maintains wakefulness.
- Other behavioral factors include the patient's pre-sleep routine and other habits that may impact sleep, e.g., alcohol, caffeine, nicotine, dinner habits, bedroom environment, etc.
- Cognitive factors include, but are not limited to, the patient's mind racing during the night, i.e. hyperarousal at bedtime, and/or worries, anxiety about sleep, e.g., amplification about consequences of insomnia, perceived control and predictability of sleep, unrealistic expectations about sleep.
- the 1070 contains three parts: (1) therapeutic advice, given on the first day a patient accesses a module, (2) the general information delivered in daily tips on the remaining days of the module, and (3) a goal setting section, accessible on the first day a patient accesses the module.
- the therapeutic advice consists of recommendations/interventions which are based on the standard CBT-I.
- the therapeutic advice and daily tips targets those factors that maintain the problems or make them worse by a particular patient and may be related to the goals identified by the patient. That is, while the general, or global, goal is to improve sleep, the patient may know of a specific problem and identify a specific goal related to that problem. For example, the patient may wish to learn to fall asleep more easily and/or learn to fall back to sleep more easily after waking in the middle of the sleep cycle.
- the patient may wish to learn how to feel more refreshed in the morning, improve their daytime energy, improve their daytime performance, improve their cognitive functioning (concentration, focus, attention and memory) and/or improve their mood and motivation.
- the patient may wish to identify their actual sleep pattern or determine how many hours of sleep they have during the night.
- the coaching and/or other advice may be related to the global goal or one or more of the more specific goals.
- the fourth processing unit 1012 is further structured to organize the selection and order of the therapeutic instruction modules based upon the patient's sleep profile. Finally, the fourth processing unit 1012 is structured to present the organized therapeutic instruction modules on the display 1014.
- the display 1014 is coupled to, and in electronic communication with, the communication assembly 1002.
- the display 1014 is structured to present the user interface 108, discussed above, as well as any other information.
- ISI Insomnia Severity Index
- IFQ Insomnia Frequency Questionnaire
- the sleep log includes both questions/statements rated on a scale, and questions/statements to which the response is a time period measured in hours and minutes.
- the sleep log includes the following questions/statements:
- the patient may receive cognitive behavioral therapy for insomnia according to a method having the following steps. Initially, the method includes the step of monitoring 2000 a patient's sleep utilizing a sensor system 1004 having at least one unobtrusive sensor 1020. As noted above, the sensor system 1004 is structured to detect sleeping activity data.
- the method further includes the steps of gathering 2002 patient input data, combining 2006 the patient input data and the sleeping activity data to create a patient sleep profile, analyzing 2008 a patient sleep profile to determine a course of therapy, and presenting 2010 the course of therapy to the patient on a display 1014.
- the step of monitoring 2000 a patient's sleep utilizing a sensor system having at least one unobtrusive sensor includes the step of utilizing 2020 an ECG sensor and an actigraph sensor.
- the ECG sensor 1022 is structured to detect heart rate data and respiratory rate data
- the actigraph sensor 1024 is structured to detect patient body movement data.
- the step of monitoring 2000 a patient's sleep utilizing a sensor system having at least one unobtrusive sensor further includes the step of processing 2022 the heart rate data, respiratory rate data, and patient body movement data to determine at least one of: the patient's time in bed, the patient's total sleep time, the patient's total wake time, the patient's sleep efficiency, the patient's sleep onset latency, the patient's awakenings after sleep onset and the patient's snooze time.
- the step of gathering 2002 patient input data includes the steps of: gathering
- the patient input data is input via the second processing unit 2008 and, more specifically, via the input assembly 1034 and the user interface 108.
- the step of analyzing 2008 a patient sleep profile to determine a course of therapy may include the steps of: analyzing 2038 the patient input data and the sleeping activity data to identify the factors contributing to the patients insomnia, identifying 2039 the type of insomnia associated with the patient, analyzing 2040 the patient input data and the sleeping activity data to determine the severity of the patient's insomnia, analyzing 2042 the patient input data to determine the severity of the effect of the patient's insomnia on daytime activities, analyzing 2044 the patient input data to determine the type of insomnia suffered by the patient, and, based on the severity of the patient's insomnia, the severity of the effect of the patient's insomnia on daytime activities, and the type of insomnia suffered by the patient, recommending 2046 to the patient one of the following: referral to a medical professional for treatment, recommending an interactive course of therapy to the patient, recommending no treatment.
- the therapy is, preferably, provided to the patient via the display 1014 which presents the user interface 108. That is, the steps of analyzing 2008 the patient sleep profile to determine a course of therapy and presenting 2010 the course of therapy to the patient on a display 1014 include the steps of: providing 2050 a plurality of interactive therapeutic instruction modules, each module related to an aspect of insomnia, based on the patient sleep profile, determining 2052 which of the interactive therapeutic instruction modules are relevant to the patient's insomnia, determining 2054 the sequence of the interactive therapeutic instruction modules to be presented to the patient, presenting, 2056 in the predetermined sequence, the interactive therapeutic instruction modules to the patient on a display 1014.
- the plurality of interactive therapeutic instruction modules include a sleep scheduling module 1060, an association bed-sleep module 1062, a cognitive restructuring module 1064, a coping strategy module 1066, a relaxation module 1068, and a lifestyle module 1070.
- the specific modules each have additional processes as discussed below.
- the interactive therapeutic instruction modules 1060, 1062, 1064, 1066, 1068, 1070 may be (1) stored on the fourth processing unit 1012, i.e. in the storage device for the fourth processing unit 1012, (2) downloaded to the fourth processing unit 1012 via the electronic communication network 1001 and the communication assembly 1002, or (3) a combination thereof. That is, the fourth processing unit 1012 may store a portion of each interactive therapeutic instruction module 1060, 1062, 1064, 1066, 1068, 1070 and have updates or additional information downloaded as well.
- the method of providing cognitive behavioral therapy for insomnia includes the further steps of: providing 2060 a sleep scheduling assessment structured to determine a first and a second sleep scheduling score, determining 2062 the patient's first and second sleep scheduling scores, and determining 2064 whether patient has an irregular sleep schedule.
- the determination 2062 of the patient's first and second sleep scheduling scores may be based on both objective and subjective data.
- objective data such as, but not limited to, sleep efficiency data collected by the sensors, as discussed above.
- Subjective data may be based on an assessment such as the following questions/statements:
- These ratings are converted into the patient's first and second sleep scheduling scores, e.g. by assigning a score to the answer and combining the score with objective data. Based on the factors that are determined, e.g. if patient's first sleep scheduling score is greater than a first sleep scheduling threshold value, the method further includes providing 2066 sleep schedule coaching, and/or, if the patient has an irregular sleep schedule and if patient's second sleep scheduling score is greater than a second sleep scheduling threshold value, providing 2068 sleep schedule coaching. In this module
- the step of coaching is accomplished by providing information to the patient.
- the information is provided via the display 1014 and in the form of text messages, e-mail, instant messages, etc.
- the coaching messages are, preferably, formatted as reminders, suggested therapeutic actions, progress reports, etc., and are typically related to a goal, as discussed above.
- the method of providing cognitive behavioral therapy for insomnia includes the further steps of: providing 2070 an association bed-sleep assessment structured to determine an association bed-sleep score, determining 2072 the patient's association bed-sleep score, and, if patient's association bed-sleep score is greater than an association bed-sleep threshold value, providing 2074 association bed-sleep coaching.
- the association bed- sleep assessment may include such questions/statements as:
- the method of providing cognitive behavioral therapy for insomnia includes the further steps of: providing 2080 a first sleep concept assessment structured to determine a first sleep concept score and determining 2082 the patient's first sleep concept score. If the patient's first sleep concept score is greater than a first sleep concept threshold value, performing 2084 a second sleep concept assessment to determine an amplification score, a perceived control score, and an unrealistic expectation score.
- Targeted coaching is provided related to any aspect of the sleep concept assessment wherein the patient is over the associated threshold value. That is, if patient's amplification score is greater than an amplification threshold value, providing 2086 amplification coaching.
- the sleep concept assessment may include such questions/statements as:
- the method of providing cognitive behavioral therapy for insomnia includes the further steps of: providing 2090 a first coping strategy assessment structured to determine a coping strategy score, determining 2092 a coping strategy score and, if patient's coping strategy score is greater than a coping strategy threshold value, providing 2094 coping strategy coaching.
- the coping strategy assessment may include such questions/statements as:
- the method of providing cognitive behavioral therapy for insomnia includes the further steps of: providing 2100 a relaxation assessment structured to determine a transition time score, a worry time score, and a behavioral score, determining 2102 a transition time score, a worry time score, and a behavioral score. If the patient's transition time score is greater than a transition time threshold value, the method includes the step of providing 2104 transition time coaching. If the patient's worry time score is greater than a worry time threshold value, the method includes the step of providing 2106 worry time coaching. If the patient's behavioral score is greater than a behavioral threshold value, the method includes the step of providing 2108 behavioral coaching.
- the relaxation assessment may include such questions/statements as:
- the method of providing cognitive behavioral therapy for insomnia includes the further steps of: providing 2110 a lifestyle assessment structured to determine a physical activity score, an alcohol score, a caffeine score, a napping score, a nicotine score, an intake score (i.e. food and/or calorie intake score), and an environment score and determining 2111 a physical activity score, an alcohol score, a caffeine score, a napping score, a nicotine score, an intake score, and an environment score. If the patient's physical activity score is greater than a physical activity threshold value, the method includes the step of providing 2112 physical activity coaching.
- the method includes the step of providing 2114 alcohol coaching. If the patient's caffeine score is greater than a caffeine threshold value, the method includes the step of providing 2116 caffeine coaching. If the patient's napping score is greater than a napping threshold value, the method includes the step of providing 2118 napping coaching. If the patient's nicotine score is greater than a nicotine threshold value, the method includes the step of providing 2120 nicotine coaching. If the patient's intake score is greater than or less than the intake threshold value (or range), the method includes the step of providing 2122 intake coaching. That is, if the patient is eating too much or too little, the patient will be beyond the intake threshold range. If the patient's environment score is greater than an environment threshold value, the method includes the step of providing 2124 environment coaching.
- the lifestyle assessment may include, but is not limited to, such questions/statements as:
- the method is, preferably, an iterative process wherein the patient's sleep profile is updated 2130 so as to reflect the patient's current level of insomnia. While the patient input data and the sleeping activity data may be updated every day, preferably the interactive course of therapy is updated regularly, but less frequently than daily. Preferably, the interactive course of therapy is updated weekly. Once the patient's patient sleep profile has been updated, the step of analyzing 2008 a patient sleep profile to determine a course of therapy is repeated.
- the step of analyzing 2008 a patient sleep profile to determine a course of therapy may also include the steps of: having 2050 a medical professional review the sleep pattern data, the patient input data and the patient sleep profile, and having 2052 the medical professional provide direct feedback to the patient via the electronic communications network 1001. These steps may be repeated after an update of the sleep pattern data, the patient input data and the patient sleep profile.
Landscapes
- Health & Medical Sciences (AREA)
- Life Sciences & Earth Sciences (AREA)
- Engineering & Computer Science (AREA)
- Public Health (AREA)
- Medical Informatics (AREA)
- General Health & Medical Sciences (AREA)
- Biomedical Technology (AREA)
- Physics & Mathematics (AREA)
- Pathology (AREA)
- Heart & Thoracic Surgery (AREA)
- Molecular Biology (AREA)
- Surgery (AREA)
- Animal Behavior & Ethology (AREA)
- Biophysics (AREA)
- Veterinary Medicine (AREA)
- Physiology (AREA)
- Cardiology (AREA)
- Business, Economics & Management (AREA)
- Dentistry (AREA)
- Oral & Maxillofacial Surgery (AREA)
- Primary Health Care (AREA)
- Epidemiology (AREA)
- General Physics & Mathematics (AREA)
- Theoretical Computer Science (AREA)
- Anesthesiology (AREA)
- Child & Adolescent Psychology (AREA)
- Educational Administration (AREA)
- Entrepreneurship & Innovation (AREA)
- Educational Technology (AREA)
- Psychology (AREA)
- Social Psychology (AREA)
- Pulmonology (AREA)
- Developmental Disabilities (AREA)
- Hospice & Palliative Care (AREA)
- Psychiatry (AREA)
- Data Mining & Analysis (AREA)
- Databases & Information Systems (AREA)
- Measurement Of The Respiration, Hearing Ability, Form, And Blood Characteristics Of Living Organisms (AREA)
- Tourism & Hospitality (AREA)
- Measuring And Recording Apparatus For Diagnosis (AREA)
Abstract
Description




Claims
Priority Applications (7)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| JP2012513716A JP5775868B2 (en) | 2009-06-04 | 2010-06-01 | System for providing behavioral therapy for insomnia and control method thereof |
| RU2011154352/14A RU2568354C2 (en) | 2009-06-04 | 2010-06-01 | Behaviour therapy method and system applicable for insomnia management |
| AU2010255354A AU2010255354A1 (en) | 2009-06-04 | 2010-06-01 | Method and system for providing behavioural therapy for insomnia |
| US13/375,325 US8979730B2 (en) | 2009-06-04 | 2010-06-01 | Method and system for providing behavioural therapy for insomnia |
| CN201080024189.8A CN102448368B (en) | 2009-06-04 | 2010-06-01 | Method and system for providing behavioural therapy for insomnia |
| EP10727937A EP2437652A1 (en) | 2009-06-04 | 2010-06-01 | Method and system for providing behavioural therapy for insomnia |
| BRPI1009049A BRPI1009049A2 (en) | 2009-06-04 | 2010-06-01 | "system designed to facilitate cognitive behavioral therapy for a patient with insomnia" |
Applications Claiming Priority (2)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| US18416509P | 2009-06-04 | 2009-06-04 | |
| US61/184,165 | 2009-06-04 |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| WO2010140117A1 true WO2010140117A1 (en) | 2010-12-09 |
Family
ID=42617401
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| PCT/IB2010/052440 WO2010140117A1 (en) | 2009-06-04 | 2010-06-01 | Method and system for providing behavioural therapy for insomnia |
Country Status (8)
| Country | Link |
|---|---|
| US (1) | US8979730B2 (en) |
| EP (1) | EP2437652A1 (en) |
| JP (1) | JP5775868B2 (en) |
| CN (1) | CN102448368B (en) |
| AU (1) | AU2010255354A1 (en) |
| BR (1) | BRPI1009049A2 (en) |
| RU (1) | RU2568354C2 (en) |
| WO (1) | WO2010140117A1 (en) |
Cited By (13)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| CN102488495A (en) * | 2011-12-19 | 2012-06-13 | 陈心广 | Digitalized intelligent evaluation method for nicotine dependence |
| CN102551664A (en) * | 2010-12-17 | 2012-07-11 | 成功大学 | Sleep analysis method, sleep analysis table and sleep analysis system |
| GB2488521A (en) * | 2011-02-16 | 2012-09-05 | Cascom Ltd | Activity recognition in living species using tri-axial acceleration data |
| CN102908711A (en) * | 2011-08-02 | 2013-02-06 | 索尼公司 | Sleep aid device and method, program and recording medium |
| CN103892797A (en) * | 2012-12-31 | 2014-07-02 | 中国移动通信集团公司 | Signal processing method and device for sleep structure analysis |
| FR3008300A1 (en) * | 2013-07-12 | 2015-01-16 | Ile Marc Frouin Soc Civ | DEVICE FOR MONITORING A PHYSIOLOGICAL CONDITION AND ALERT THROUGH AN INTELLIGENT CLOTHING WITH INTEGRATED BIOMETRIC SENSORS, AN APPLICATION AND A CLOUD SYSTEM |
| US20150080756A1 (en) * | 2012-01-27 | 2015-03-19 | The University Of Sydney | Estimating arousal states |
| TWI553584B (en) * | 2014-10-24 | 2016-10-11 | 國立清華大學 | Evaluation system, method and computer program product of relaxation state |
| US9633175B2 (en) | 2013-02-05 | 2017-04-25 | Big Health Ltd | Interactive system for sleep improvement |
| WO2018001758A1 (en) | 2016-06-27 | 2018-01-04 | Koninklijke Philips N.V. | Determination system and method for determining a sleep stage of a subject |
| JP2018519967A (en) * | 2015-07-21 | 2018-07-26 | コーニンクレッカ フィリップス エヌ ヴェKoninklijke Philips N.V. | Method and system for automatic labeling of activities in ECG data |
| KR20190092765A (en) | 2018-01-31 | 2019-08-08 | 박성규 | Method for providing insomnia mediation service and apparatus therefor |
| CN114191684A (en) * | 2022-02-16 | 2022-03-18 | 浙江强脑科技有限公司 | Sleep control method and device based on electroencephalogram, intelligent terminal and storage medium |
Families Citing this family (76)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| JP5803169B2 (en) * | 2011-03-14 | 2015-11-04 | オムロンヘルスケア株式会社 | Sleep evaluation apparatus and sleep evaluation method |
| US9152768B2 (en) * | 2011-09-26 | 2015-10-06 | Hill-Rom Services, Inc. | Method and system for patient care management |
| JP5788293B2 (en) * | 2011-10-31 | 2015-09-30 | オムロンヘルスケア株式会社 | Sleep evaluation apparatus and sleep evaluation program |
| US9339691B2 (en) | 2012-01-05 | 2016-05-17 | Icon Health & Fitness, Inc. | System and method for controlling an exercise device |
| JP6522342B2 (en) * | 2012-01-06 | 2019-05-29 | シグニファイ ホールディング ビー ヴィ | Emergency response and tracking using lighting networks |
| US10856800B2 (en) * | 2012-06-08 | 2020-12-08 | United States Government As Represented By The Department Of Veterans Affairs | Portable polysomnography apparatus and system |
| CA2925804A1 (en) * | 2012-09-26 | 2014-04-03 | Seth D. Feuerstein | Combination methods and compositions including sleep therapeutics for treating mood |
| EP2969058B1 (en) | 2013-03-14 | 2020-05-13 | Icon Health & Fitness, Inc. | Strength training apparatus with flywheel and related methods |
| US11813076B2 (en) | 2013-03-15 | 2023-11-14 | Sleepme Inc. | Stress reduction and sleep promotion system |
| US11883606B2 (en) | 2013-03-15 | 2024-01-30 | Sleep Solutions Inc. | Stress reduction and sleep promotion system |
| US11602611B2 (en) | 2013-03-15 | 2023-03-14 | Sleepme Inc. | System for enhancing sleep recovery and promoting weight loss |
| US11896774B2 (en) | 2013-03-15 | 2024-02-13 | Sleep Solutions Inc. | System for enhancing sleep recovery and promoting weight loss |
| EP3937107A1 (en) | 2013-05-21 | 2022-01-12 | Tomer Ben-Kiki | Systems and methods for providing on-line services |
| US10813584B2 (en) | 2013-05-21 | 2020-10-27 | Happify, Inc. | Assessing adherence fidelity to behavioral interventions using interactivity and natural language processing |
| US20190129941A2 (en) | 2013-05-21 | 2019-05-02 | Happify, Inc. | Systems and methods for dynamic user interaction for improving happiness |
| CN104720746B (en) * | 2013-12-20 | 2017-06-20 | 中国移动通信集团公司 | A kind of sleep stage determines method and system |
| WO2015100429A1 (en) | 2013-12-26 | 2015-07-02 | Icon Health & Fitness, Inc. | Magnetic resistance mechanism in a cable machine |
| US9655559B2 (en) * | 2014-01-03 | 2017-05-23 | Vital Connect, Inc. | Automated sleep staging using wearable sensors |
| US9579060B1 (en) | 2014-02-18 | 2017-02-28 | Orbitol Research Inc. | Head-mounted physiological signal monitoring system, devices and methods |
| US10433612B2 (en) | 2014-03-10 | 2019-10-08 | Icon Health & Fitness, Inc. | Pressure sensor to quantify work |
| US9694156B2 (en) | 2014-06-05 | 2017-07-04 | Eight Sleep Inc. | Bed device system and methods |
| US9186479B1 (en) | 2014-06-05 | 2015-11-17 | Morphy Inc. | Methods and systems for gathering human biological signals and controlling a bed device |
| US10426989B2 (en) | 2014-06-09 | 2019-10-01 | Icon Health & Fitness, Inc. | Cable system incorporated into a treadmill |
| WO2015195965A1 (en) | 2014-06-20 | 2015-12-23 | Icon Health & Fitness, Inc. | Post workout massage device |
| JP6385470B2 (en) * | 2014-06-30 | 2018-09-05 | コーニンクレッカ フィリップス エヌ ヴェKoninklijke Philips N.V. | Device, system and computer program for detecting the health condition of a subject |
| US20160192218A1 (en) * | 2014-07-14 | 2016-06-30 | Under Armour, Inc. | Techniques for classifying sleep sessions |
| US20160034671A1 (en) * | 2014-07-29 | 2016-02-04 | Elwha Llc | Method and Apparatus for Designating Patients According to Sleep Patterns |
| US20160035056A1 (en) * | 2014-07-29 | 2016-02-04 | Elwha Llc | Method and Apparatus for Designating Patients According to Sleep Patterns |
| EP3195243A4 (en) * | 2014-07-29 | 2018-04-04 | Elwha LLC | Method and apparatus for designating patients according to sleep patterns |
| US20160035057A1 (en) * | 2014-07-29 | 2016-02-04 | Elwha Llc | Method and Apparatus for Designating Patients According to Sleep Patterns |
| WO2016083294A1 (en) * | 2014-11-24 | 2016-06-02 | Tarkett Gdl | Monitoring system with pressure sensor in floor covering |
| WO2016087983A1 (en) * | 2014-12-03 | 2016-06-09 | Koninklijke Philips N.V. | System and method for increasing the restorative value of a nap |
| JP6761417B2 (en) * | 2014-12-19 | 2020-09-23 | コーニンクレッカ フィリップス エヌ ヴェKoninklijke Philips N.V. | Dynamic wearable device behavior based on schedule detection |
| JP2016122348A (en) * | 2014-12-25 | 2016-07-07 | オムロン株式会社 | Life style improvement apparatus, life style improvement method and life style improvement system |
| JP6485037B2 (en) * | 2014-12-25 | 2019-03-20 | オムロン株式会社 | Sleep improvement system and sleep improvement method using the system |
| US10391361B2 (en) | 2015-02-27 | 2019-08-27 | Icon Health & Fitness, Inc. | Simulating real-world terrain on an exercise device |
| US10542961B2 (en) | 2015-06-15 | 2020-01-28 | The Research Foundation For The State University Of New York | System and method for infrasonic cardiac monitoring |
| WO2017053728A1 (en) * | 2015-09-23 | 2017-03-30 | Emfit, Corp. | Heart rate monitoring device, system, and method for increasing performance improvement efficiency |
| US10213145B1 (en) * | 2015-10-01 | 2019-02-26 | Cerner Innovation, Inc. | Context-aware post traumatic stress disorder monitoring and intervention |
| CN113499062A (en) * | 2015-10-07 | 2021-10-15 | 普莱柯迪尔公司 | Method and apparatus for generating information indicative of a cardiac condition |
| US10154932B2 (en) | 2015-11-16 | 2018-12-18 | Eight Sleep Inc. | Adjustable bedframe and operating methods for health monitoring |
| US10105092B2 (en) | 2015-11-16 | 2018-10-23 | Eight Sleep Inc. | Detecting sleeping disorders |
| WO2017136464A1 (en) | 2016-02-01 | 2017-08-10 | Prevencio, Inc. | Diagnostic and prognostic methods for cardiovascular diseases and events |
| US10272317B2 (en) | 2016-03-18 | 2019-04-30 | Icon Health & Fitness, Inc. | Lighted pace feature in a treadmill |
| US10625137B2 (en) | 2016-03-18 | 2020-04-21 | Icon Health & Fitness, Inc. | Coordinated displays in an exercise device |
| US10493349B2 (en) | 2016-03-18 | 2019-12-03 | Icon Health & Fitness, Inc. | Display on exercise device |
| CN107920753B (en) * | 2016-05-09 | 2021-08-27 | 皇家飞利浦有限公司 | Sleep monitoring |
| US10325514B2 (en) * | 2016-06-02 | 2019-06-18 | Fitbit, Inc. | Systems and techniques for tracking sleep consistency and sleep goals |
| US20180085050A1 (en) * | 2016-09-28 | 2018-03-29 | Arizona Board Of Regents On Behalf Of The University Of Arizona | Systems and methods for individualized sleep optimization |
| US10671705B2 (en) | 2016-09-28 | 2020-06-02 | Icon Health & Fitness, Inc. | Customizing recipe recommendations |
| MX2019004220A (en) * | 2016-10-11 | 2019-08-26 | Sustainable Medicine Inc | Insomnia treatment assistance device and insomnia treatment assistance program. |
| US20180113991A1 (en) * | 2016-10-26 | 2018-04-26 | Sarah Davidson | Interactive Apparatus and Devices for Personal Symptom Management and Therapeutic Treatment Systems |
| WO2018077844A1 (en) | 2016-10-28 | 2018-05-03 | Telefonica Innovacion Alpha S.L. | System and a method for enabling responsive cognitive behavioral therapy |
| EP3609390A4 (en) * | 2017-04-14 | 2020-09-16 | Emfit Ltd. | Wearable sensor and system thereof |
| CN107169272B (en) * | 2017-05-04 | 2020-03-27 | 北京心海导航教育科技股份有限公司 | Cognitive behavior training method and system |
| CN107657748A (en) * | 2017-10-20 | 2018-02-02 | 深圳市华达康科技有限公司 | A kind of Internet of Things intelligent sharing mattress adds hotel's ecological chain operation system and method |
| TWI698223B (en) * | 2017-11-20 | 2020-07-11 | 金寶電子工業股份有限公司 | Wearable device capable of recognizing doze-off stage and recognition method thereof |
| CN108010569A (en) * | 2017-12-28 | 2018-05-08 | 曹亮明 | A kind of assistant interventional psychosomatic disease and the intelligent physical therapeutic system of insomnia |
| GB2584242B (en) | 2018-01-09 | 2022-09-14 | Eight Sleep Inc | Systems and methods for detecting a biological signal of a user of an article of furniture |
| GB2584241B (en) | 2018-01-19 | 2023-03-08 | Eight Sleep Inc | Sleep pod |
| SE1850792A1 (en) * | 2018-06-26 | 2020-01-28 | ||
| WO2020082115A1 (en) * | 2018-10-22 | 2020-04-30 | Alertness CRC Ltd | Decision support software system for sleep disorder identification |
| WO2020087114A1 (en) * | 2018-10-29 | 2020-05-07 | Alertness CRC Ltd | Personalised sleep scheduler |
| US11382560B2 (en) * | 2019-03-28 | 2022-07-12 | The Trustees Of The University Of Pennsylvania | Systems and methods for sleep optimization |
| JP2022551816A (en) * | 2019-09-21 | 2022-12-14 | マイカーディオ エルエルシー | Systems and methods for specifying REM and wakefulness states |
| EP4051091B1 (en) | 2019-10-31 | 2023-08-02 | ResMed Sensor Technologies Limited | Systems for insomnia screening and management |
| US20210282706A1 (en) * | 2020-03-16 | 2021-09-16 | Koninklijke Philips N.V. | Characterizing stimuli response to detect sleep disorders |
| US11837106B2 (en) * | 2020-07-20 | 2023-12-05 | Koninklijke Philips N.V. | System and method to monitor and titrate treatment for high altitude-induced central sleep apnea (CSA) |
| CN112717254B (en) * | 2020-12-24 | 2022-10-04 | 重庆适领科技有限公司 | Control method of intelligent aromatherapy fragrance expander system |
| JP6928413B1 (en) * | 2021-03-09 | 2021-09-01 | サスメド株式会社 | Insomnia treatment support device, insomnia treatment support system and insomnia treatment support program |
| US20220344057A1 (en) * | 2021-04-27 | 2022-10-27 | Oura Health Oy | Method and system for supplemental sleep detection |
| KR20220156466A (en) * | 2021-05-18 | 2022-11-25 | 연세대학교 원주산학협력단 | System for improving sleep quality and method using the same |
| CN113288095B (en) * | 2021-05-24 | 2022-07-08 | 南京优博一创智能科技有限公司 | Sleep health management method and system for calculating sleep cycle based on physical activity and heart rate information |
| CN113398424A (en) * | 2021-07-13 | 2021-09-17 | 正岸(北京)科技有限公司 | Insomnia treatment system and working method thereof |
| US20240082532A1 (en) * | 2022-09-08 | 2024-03-14 | Sleep Number Corporation | Bed with features for determination of insomnia risk |
| CN117224098B (en) * | 2023-09-15 | 2024-02-20 | 广州麦笛亚医疗器械有限公司 | Evaluation method, system, equipment and storage medium for heart rate variability |
Citations (2)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| EP0773504A1 (en) | 1995-11-08 | 1997-05-14 | Oxford Medical Limited | Improvements relating to physiological monitoring |
| WO2004078132A2 (en) | 2003-02-28 | 2004-09-16 | Consolidated Research Of Richmond, Inc. | Automated insomnia treatment system |
Family Cites Families (10)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| JP2000000214A (en) * | 1998-06-15 | 2000-01-07 | Arata Nemoto | Sleeping monitor device |
| ES2515092T3 (en) * | 2003-12-11 | 2014-10-29 | Sunovion Pharmaceuticals Inc. | Combination of a sedative and a neurotransmitter modulator and methods of improving sleep quality and treating depression |
| US7524279B2 (en) * | 2003-12-31 | 2009-04-28 | Raphael Auphan | Sleep and environment control method and system |
| US8403865B2 (en) * | 2004-02-05 | 2013-03-26 | Earlysense Ltd. | Prediction and monitoring of clinical episodes |
| US20070118054A1 (en) | 2005-11-01 | 2007-05-24 | Earlysense Ltd. | Methods and systems for monitoring patients for clinical episodes |
| JP2006006355A (en) * | 2004-06-22 | 2006-01-12 | Sony Corp | Processor for biological information and video and sound reproducing device |
| CN101032402A (en) * | 2006-03-10 | 2007-09-12 | 通用电气公司 | Device, system and method for detecting human's movement |
| US20080275349A1 (en) * | 2007-05-02 | 2008-11-06 | Earlysense Ltd. | Monitoring, predicting and treating clinical episodes |
| US7637859B2 (en) * | 2007-06-08 | 2009-12-29 | Sony Ericsson Mobile Communications Ab | Sleeping mode accessory |
| WO2009061455A1 (en) * | 2007-11-07 | 2009-05-14 | Somerset Medical Center | A method and system for identification and management of patients for sleep disorders |
-
2010
- 2010-06-01 EP EP10727937A patent/EP2437652A1/en not_active Ceased
- 2010-06-01 RU RU2011154352/14A patent/RU2568354C2/en active
- 2010-06-01 CN CN201080024189.8A patent/CN102448368B/en active Active
- 2010-06-01 BR BRPI1009049A patent/BRPI1009049A2/en not_active Application Discontinuation
- 2010-06-01 JP JP2012513716A patent/JP5775868B2/en active Active
- 2010-06-01 WO PCT/IB2010/052440 patent/WO2010140117A1/en active Application Filing
- 2010-06-01 US US13/375,325 patent/US8979730B2/en active Active
- 2010-06-01 AU AU2010255354A patent/AU2010255354A1/en not_active Abandoned
Patent Citations (2)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| EP0773504A1 (en) | 1995-11-08 | 1997-05-14 | Oxford Medical Limited | Improvements relating to physiological monitoring |
| WO2004078132A2 (en) | 2003-02-28 | 2004-09-16 | Consolidated Research Of Richmond, Inc. | Automated insomnia treatment system |
Non-Patent Citations (1)
| Title |
|---|
| See also references of EP2437652A1 |
Cited By (18)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| CN102551664A (en) * | 2010-12-17 | 2012-07-11 | 成功大学 | Sleep analysis method, sleep analysis table and sleep analysis system |
| GB2488521A (en) * | 2011-02-16 | 2012-09-05 | Cascom Ltd | Activity recognition in living species using tri-axial acceleration data |
| CN102908711A (en) * | 2011-08-02 | 2013-02-06 | 索尼公司 | Sleep aid device and method, program and recording medium |
| CN102488495A (en) * | 2011-12-19 | 2012-06-13 | 陈心广 | Digitalized intelligent evaluation method for nicotine dependence |
| US20150080756A1 (en) * | 2012-01-27 | 2015-03-19 | The University Of Sydney | Estimating arousal states |
| CN103892797A (en) * | 2012-12-31 | 2014-07-02 | 中国移动通信集团公司 | Signal processing method and device for sleep structure analysis |
| US9633175B2 (en) | 2013-02-05 | 2017-04-25 | Big Health Ltd | Interactive system for sleep improvement |
| FR3008300A1 (en) * | 2013-07-12 | 2015-01-16 | Ile Marc Frouin Soc Civ | DEVICE FOR MONITORING A PHYSIOLOGICAL CONDITION AND ALERT THROUGH AN INTELLIGENT CLOTHING WITH INTEGRATED BIOMETRIC SENSORS, AN APPLICATION AND A CLOUD SYSTEM |
| TWI553584B (en) * | 2014-10-24 | 2016-10-11 | 國立清華大學 | Evaluation system, method and computer program product of relaxation state |
| JP2018519967A (en) * | 2015-07-21 | 2018-07-26 | コーニンクレッカ フィリップス エヌ ヴェKoninklijke Philips N.V. | Method and system for automatic labeling of activities in ECG data |
| WO2018001758A1 (en) | 2016-06-27 | 2018-01-04 | Koninklijke Philips N.V. | Determination system and method for determining a sleep stage of a subject |
| CN109328034A (en) * | 2016-06-27 | 2019-02-12 | 皇家飞利浦有限公司 | For determining the determination system and method for the sleep stage of object |
| RU2704787C1 (en) * | 2016-06-27 | 2019-10-30 | Конинклейке Филипс Н.В. | System and method of determining for determining a stage of sleep of a subject |
| US10624574B2 (en) | 2016-06-27 | 2020-04-21 | Koninklijke Philips N.V. | Determination system and method for determining a sleep stage of a subject |
| KR20190092765A (en) | 2018-01-31 | 2019-08-08 | 박성규 | Method for providing insomnia mediation service and apparatus therefor |
| KR102141804B1 (en) * | 2018-01-31 | 2020-08-06 | 박성규 | Method for providing insomnia mediation service and apparatus therefor |
| CN114191684A (en) * | 2022-02-16 | 2022-03-18 | 浙江强脑科技有限公司 | Sleep control method and device based on electroencephalogram, intelligent terminal and storage medium |
| CN114191684B (en) * | 2022-02-16 | 2022-05-17 | 浙江强脑科技有限公司 | Sleep control method and device based on electroencephalogram, intelligent terminal and storage medium |
Also Published As
| Publication number | Publication date |
|---|---|
| BRPI1009049A2 (en) | 2016-03-08 |
| RU2011154352A (en) | 2013-07-20 |
| US20120238800A1 (en) | 2012-09-20 |
| JP2012528655A (en) | 2012-11-15 |
| CN102448368A (en) | 2012-05-09 |
| EP2437652A1 (en) | 2012-04-11 |
| JP5775868B2 (en) | 2015-09-09 |
| CN102448368B (en) | 2015-05-27 |
| RU2568354C2 (en) | 2015-11-20 |
| AU2010255354A1 (en) | 2012-02-02 |
| US8979730B2 (en) | 2015-03-17 |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| US8979730B2 (en) | Method and system for providing behavioural therapy for insomnia | |
| EP2265173B1 (en) | Method and system for sleep/wake condition estimation | |
| Paalasmaa et al. | Unobtrusive online monitoring of sleep at home | |
| RU2634624C2 (en) | System and method for determination of human sleep and sleep stages | |
| US9519755B2 (en) | Method and system for evaluating a physiological state depicting a person's resources | |
| US8666482B2 (en) | Method, system and software product for the measurement of heart rate variability | |
| RU2704787C1 (en) | System and method of determining for determining a stage of sleep of a subject | |
| WO2008096307A1 (en) | Sleep management | |
| KR101383199B1 (en) | Well-being pillow system | |
| CN111820879A (en) | Health evaluation management method suitable for chronic disease patients | |
| JP2014039586A (en) | Sleep improvement support device | |
| Paalasmaa | Monitoring sleep with force sensor measurement | |
| GB2469547A (en) | Measurement of heart rate variability | |
| Alharbi | Non-invasive Wearable Solutions to Identify Individuals with Mild Cognitive Impairments from Healthy Controls | |
| Ryser | Movement-based sleep detection–a wearable sensor system to assess quantity and quality of sleep | |
| TW202403777A (en) | Health state determination method and health state determination system | |
| Williams | Investigating the Relationship between Sleep and Wake Behavior Using Machine Learning and Smart Home Sensors | |
| Wongdhamma | Statistical models for detecting existence of obstructive sleep apnea, predicting its severity, and forecasting future episodes |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| WWE | Wipo information: entry into national phase |
Ref document number: 201080024189.8 Country of ref document: CN |
|
| 121 | Ep: the epo has been informed by wipo that ep was designated in this application |
Ref document number: 10727937 Country of ref document: EP Kind code of ref document: A1 |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 2010727937 Country of ref document: EP |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 2012513716 Country of ref document: JP |
|
| NENP | Non-entry into the national phase |
Ref country code: DE |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 9707/CHENP/2011 Country of ref document: IN |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 2010255354 Country of ref document: AU |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 2011154352 Country of ref document: RU |
|
| ENP | Entry into the national phase |
Ref document number: 2010255354 Country of ref document: AU Date of ref document: 20100601 Kind code of ref document: A |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 13375325 Country of ref document: US |
|
| REG | Reference to national code |
Ref country code: BR Ref legal event code: B01A Ref document number: PI1009049 Country of ref document: BR |
|
| ENP | Entry into the national phase |
Ref document number: PI1009049 Country of ref document: BR Kind code of ref document: A2 Effective date: 20111130 |